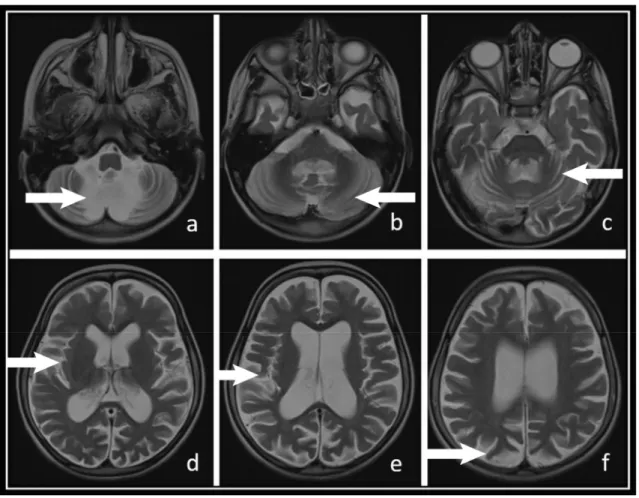
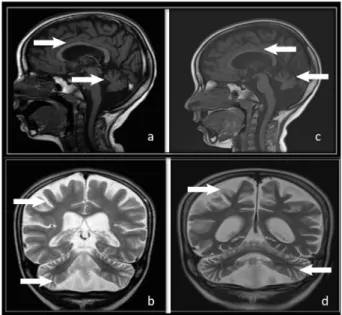
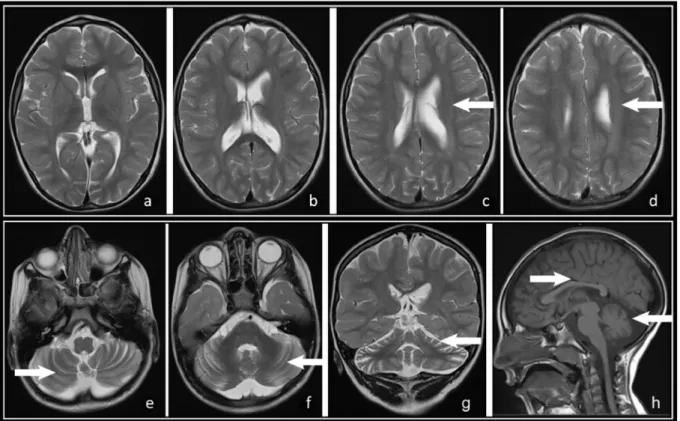
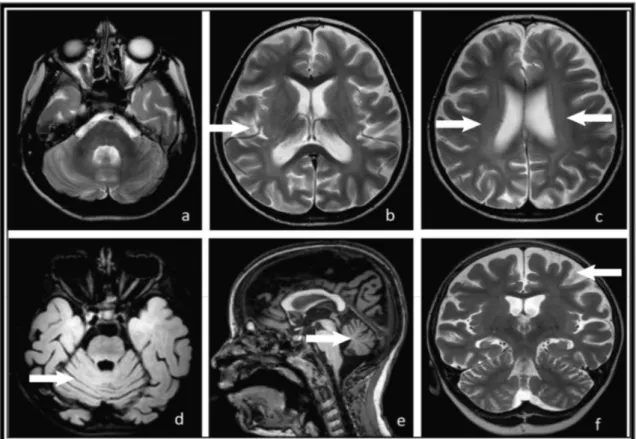
MRI in CLN2 disease patients: Subtle features that support an early diagnosis
Tam metin
Şekil

Benzer Belgeler
AT’nin ihmal edilmemesi konusunda siyasal çevrelere uyanlarda bulunan Vehbi Koç, bu arada ilgili çevrelere mesaj vermeyi de ihmal etmemişti: “AT’nin bizim gibi büyük
Anlad~~~m kadar~yla CIEPO (Osmanl~~ Öncesi ve Osmanl~~ Ara~t~rmalar~) Ba~kan~~ Jean Louis Bacque-Grammont, bu kongre içinde bir CIEPO seksi- yonu açabilmek için beni ve CIEPO'ya
With this, the research problem identified as an existing weakness in the directed knowledge base at the extent of the impact of virtual reality technology on the architectural
doza ba¤l› olarak artt›¤›na dair Jauhari ve ark (8) yafllar› 22-25 yafl aral›¤›nda de¤iflen, 7 olgunun yedikleri bal sonras› zehirlendiklerini, tüketilen bal
Sağlık Bakanlığı Türkiye Halk Sağlığı Ku- rumu Aile Hekimliği Uygulamasında Önerilen PSM ve Tarama Testleri Kılavuzunda ise öneriler AAFP ve USPSTF’ye
Bu çal›flmada, Türkiye’de yaklafl›k yar›m yüzy›ll›k sü- reçte, birinci basamak temelli çal›flan bir hekimin tuttu¤u hasta kay›tlar›ndan aile
Fakihler süt emmeden dolayı emen çocuk ile emziren kadın ve onun belli yakınları arasında hısımlığın meydana geldiğinde hemfikir olmakla bir- likte
hiçbir faktör anlamlı prognostik faktör olarak bulu- namazken, çok değişkenli analizde, nükleer atipi, FIGO klinik evresi, artmış mitoz oranı, ameliyat öncesi ya
