cambridge.org/jlo
Main Article
Dr O Erdur takes responsibility for the integrity of the content of the paper
Cite this article:Erdur O, Gul O, Ozturk K. Evaluation of upper oesophageal sphincter in unilateral vocal fold paralysis. J Laryngol Otol 2019;133:149–154. https://doi.org/10.1017/ S0022215119000045
Accepted: 17 September 2018 First published online: 1 February 2019
Key words:
Unilateral Vocal Cord Paralysis; Aspiration, Respiratory; Dysphagia; Manometry; Upper Esophageal Sphincter
Author for correspondence: Dr Omer Erdur,
Selcuk University Medical Faculty Hospital, Alaeddin Keykubad Campus, 42075 Yeni Istanbul Caddesi, Konya, Turkey E-mail:[email protected]
© JLO (1984) Limited, 2019
unilateral vocal fold paralysis
O Erdur, O Gul and K OzturkDepartment of Otolaryngology, Selcuk University Medical Faculty Hospital, Konya, Turkey Abstract
Objective. To evaluate dysphagia and manometric changes in the upper oesophageal sphinc-ter in patients with unilasphinc-teral vocal fold paralysis.
Methods. Thirty patients with unilateral vocal fold paralysis due to vagal nerve paralysis scheduled for evaluation were enrolled in the study group; 24 healthy subjects were included in the control group. Upper oesophageal sphincter basal and residual pressure, relaxation time, and pharyngeal pressure values were evaluated by manometry. All patients completed the Turkish Eating Assessment Tool 10 questionnaire, the MD Anderson dysphagia question-naire and the reflux symptom index form.
Results. Swallowing assessment questionnaires and reflux symptom index results were signifi-cantly higher in the study group. Upper oesophageal sphincter basal and relaxation pressures were lower in the study group. Upper oesophageal sphincter relaxation time was shorter in the study group, but pressure values recorded from the pharynx were higher.
Conclusion. Upper oesophageal sphincter manometric pressure was lower in patients with unilateral vocal fold paralysis. A hypotonic sphincter likely contributes to dysphagia and aspiration.
Introduction
Glottic mobility and competence play important roles during deglutition and phonation. Unilateral vocal fold paralysis is an important cause of glottic immobility. Unilateral vocal fold paralysis related voice, voice-related quality of life and respiratory problems are well described in the literature.1–3However, few studies have focused on swallowing and aspir-ation problems.4,5 Aspiration reportedly occurs in about half of patients with unilateral vocal fold paralysis.6,7 Vagal nerve paralysis is an aetiological factor in approximately 6 per cent of patients with dysphagia.8 However, glottic insufficiency is the main cause of swallowing problems in patients with unilateral vocal fold paralysis.7,9,10
The cricopharyngeal muscle is the principal structure of the high-pressure area of the upper oesophageal sphincter. This muscle is active during rest and inactive during swal-lowing, allowing food passage to the oesophagus. Although the innervation of the crico-pharyngeal muscle and upper oesophageal sphincter is controversial, the recurrent laryngeal nerve, pharyngeal branches of the vagus and the pharyngeal plexus are consid-ered to participate.11,12The upper oesophageal sphincter is the most important area in oropharyngeal dysphagia and is usually evaluated by anatomical tests; its physiology is interpreted indirectly. In addition, it is difficult to assess this area either endoscopically or radiologically.
Manometry provides the most beneficial results in patients with oropharyngeal dys-phagia.13 Manometric evaluation of the upper oesophageal sphincter yields objective data that may explain the underlying physiology. Although high-resolution manometers have become available in recent years, conventional solid-state manometers are still thought to be reliable.14We hypothesised that the upper oesophageal sphincter would be affected manometrically in patients with unilateral vocal fold paralysis because of vagal nerve paralysis, and that this effect would contribute to the swallowing pathology. In this study, we evaluated the upper oesophageal sphincter pressure and dysphagia of patients with unilateral vocal fold paralysis in comparison with that of healthy controls.
Materials and methods
Our study protocol was approved by the ethics committee (number 2016/129). Patients diagnosed with unilateral vocal fold paralysis due to vagal nerve pathology from January 2016 to October 2017 were informed of the study, and those who were willing were included in the study.
Patients aged less than 18 years and those with a disease onset less than 6 months prior were excluded from the study. Patients were also excluded if they had: a history of vocal medialisation, laryngeal cancer or previous laryngeal resection, neurological deficits other than vagal paralysis that may contribute to swallowing pathology, an inability to complete
manometric evaluation, and/or a history of exposure to radi-ation or any other additional pathology.
The control group consisted of age- and sex-matched healthy volunteers with normal swallowing and healthy vocal folds.
Diagnoses of vocal fold paralysis were made based on flex-ible fibre-optic endoscopic examination findings. At our voice and swallowing pathologies clinic, all patients with unilateral vocal fold paralysis undergo a functional endoscopic swallow-ing evaluation and a modified barium oesophagus study to identify swallowing impairments. Thus, the enrolled patients underwent conventional solid-state manometry after func-tional endoscopic swallowing evaluation. Control patients underwent functional endoscopic swallowing evaluation fol-lowed by manometric evaluation.
Manometric assessment
Before the procedure, patients confirmed that they did not use any medication that could affect the evaluation. The flexible manometry probe integrated in the swallowing unit (KayPentax, Lincoln Park, New Jersey, USA) was used. The solid-state mano-metry probe (model CTS3; Galtek, Hackensack, New Jersey, USA) was 100 cm in length, 2.1 mm in diameter and met the required catheter standards (Figure 1).
Pressure measurements were made using three sensors, of which the first was placed in the upper oesophageal sphincter 3–5 cm proximal to the sphincter. The manometer catheter is shown in Figure 2. The display was set at a frequency of 500 Hz and a pressure of −100 to + 250 mmHg. Before the procedure, the catheter was calibrated using a manometry cali-bration kit (Medical Measurements, Hackensack, New Jersey, USA).
The patient’s head was held in the neutral position. The endoscope was inserted through the nasal cavity, and an assist-ant inserted the manometry catheter through the other nostril to allow the probe to reach the hypopharynx and the high-pressure zone. By moving the probe forward and backward, the first sensor was positioned in the high-pressure zone of the upper oesophageal sphincter for 10 seconds to assess upper oesophageal sphincter basal pressure. Patients per-formed dry swallows, and wave recordings were taken by com-puter to measure the upper oesophageal sphincter residual pressure and relaxation time. The other sensors received sig-nals from the pharynx. Sensors 2 and 3 recorded
simultaneously during swallowing to evaluate pharyngeal peak pressure.
During the procedure, an assistant stabilised the catheter. All procedures were repeated at least three times and per-formed by the same two experienced physicians to optimise measurements.
Evaluation scales
Patients in the study and control groups completed the
Turkish version of the Eating Assessment Tool 10
(‘T-EAT-10’) swallowing questionnaire,15 the MD Anderson dysphagia questionnaire and the reflux symptom index.16 Two experienced physicians evaluated penetration aspiration scale scores based on functional endoscopic swallowing evalu-ation records.
Results
The study and control groups included 30 and 24 patients, respectively. The study group consisted of 15 men (50 per cent) and 15 women (50 per cent), with a mean age of 53.43 ± 11.113 years. The control group consisted of 13 men (54.2 per cent) and 11 women (45.8 per cent), with a mean age of 48.54 ± 13.062 years. No significant difference in sex or age was observed between the groups ( p > 0.05).
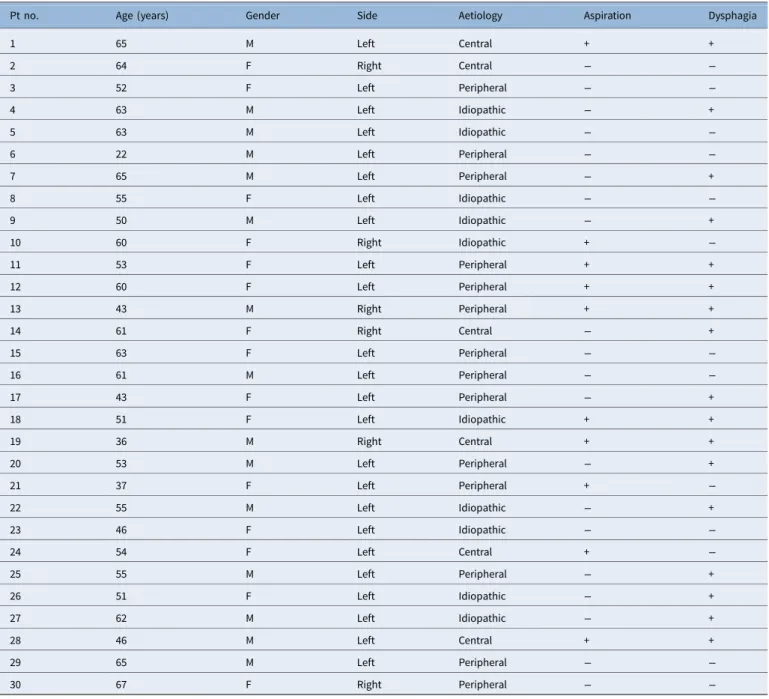
Vocal fold paralysis was most frequent on the left side (n = 24, 80 per cent). Aspiration was observed in 10 of the 30 study group patients (33.3 per cent). Dysphagia was observed in 17 of the 30 patients (56 per cent) (Table 1). The scores of the Turkish version of the Eating Assessment Tool 10, MD Anderson dysphagia questionnaire, reflux symptom index and penetration aspiration scale were significantly higher in the study group compared with the control group (Table 2).
Fig. 1.The manometry catheter used in our clinic.
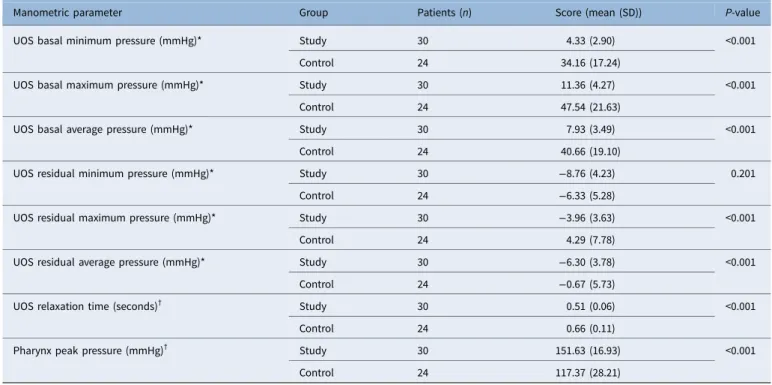
The mean values, standard deviations and statistical com-parisons of the manometric data of the two groups are
shown in Table 3. The minimum, maximum and average
upper oesophageal sphincter basal pressures were lower in the study group than in the control group ( p < 0.001). The sphincter relaxation time was significantly shorter in the study group than in the control group ( p < 0.001). The min-imum upper oesophageal sphincter residual pressure did not differ significantly ( p = 0.201), but the maximum and average upper oesophageal sphincter residual pressures were signifi-cantly lower in the study group than in the control group ( p < 0.001). The mean peak pressure of the two sensors in the pharynx during swallowing was significantly higher in the study group ( p < 0.001).
Discussion
Patients with unilateral vocal fold paralysis have considerable swallowing and reflux problems. Manometric evaluation of the upper oesophageal sphincter region revealed decreased basal and residual pressures and upper oesophageal sphincter relaxation duration in patients with vocal fold paralysis. Peak pharynx pressure during swallowing was higher on pharyngeal
Table 1.Patients’ demographics, with aspiration and dysphagia status
Pt no. Age (years) Gender Side Aetiology Aspiration Dysphagia
1 65 M Left Central + + 2 64 F Right Central − − 3 52 F Left Peripheral − − 4 63 M Left Idiopathic − + 5 63 M Left Idiopathic − − 6 22 M Left Peripheral − − 7 65 M Left Peripheral − + 8 55 F Left Idiopathic − − 9 50 M Left Idiopathic − + 10 60 F Right Idiopathic + − 11 53 F Left Peripheral + + 12 60 F Left Peripheral + + 13 43 M Right Peripheral + + 14 61 F Right Central − + 15 63 F Left Peripheral − − 16 61 M Left Peripheral − − 17 43 F Left Peripheral − + 18 51 F Left Idiopathic + + 19 36 M Right Central + + 20 53 M Left Peripheral − + 21 37 F Left Peripheral + − 22 55 M Left Idiopathic − + 23 46 F Left Idiopathic − − 24 54 F Left Central + − 25 55 M Left Peripheral − + 26 51 F Left Idiopathic − + 27 62 M Left Idiopathic − + 28 46 M Left Central + + 29 65 M Left Peripheral − − 30 67 F Right Peripheral − −
Pt no. = patient number; M = male; F = female;‘+’ = positive; ‘−’ = negative
Table 2.Evaluation scale data Evaluation scale Group Patients (n) Score (mean (SD)) P-value T-EAT-10* Study 30 10.63 (9.72) 0.001 Control 24 2.58 (3.43) MD Anderson* Study 30 17.76 (12.64) <0.001 Control 24 3.33 (4.58) RSI† Study 30 20.33 (11.68) 0.001 Control 24 10.62 (7.74) PAS* Study 30 3.40 (2.67) <0.001 Control 24 1.2 (0.41)
*Mann–Whitney U test;†independent two-sample t-test. SD = standard deviation; T-EAT-10 =
Turkish version of the Eating Assessment Tool 10; RSI = reflux symptom index; PAS = penetration aspiration scale
recordings. The data in this study enabled identification of the hypotonic upper oesophageal sphincter area in patients with unilateral vocal fold paralysis.
Aspiration and penetration scores improve during treat-ments seeking to improve voice parameters in patients with unilateral vocal fold paralysis.5,17However, in some patients, dysphagia and aspiration continue even after glottic closure.4,17 Therefore, glottic gape may not be the sole cause of dysphagia and aspiration problems in this population.10,17 Few studies have addressed this issue, and other contributing factors are not fully understood. Physiological changes in the upper oesophageal sphincter region may play a role in deglutition problems, as the vagus nerve participates in the innervation of this area.
Deglutition problems and manometric changes in the upper oesophageal sphincter in vocal immobility remain debated, and only a few relevant studies have appeared. Henderson et al. evaluated eight patients with vocal fold par-alysis using a water-perfusion manometer, but the results were unsatisfactory.18Wilson et al. evaluated the upper oesophageal sphincter in patients with unilateral vocal fold paralysis and healthy controls using a solid-state conventional manometer.19 They found that the basal pressure was lower in those with central vagal pathologies, while the residual pressure was lower in peripheral and idiopathic cases.
Recently, Pinna et al. evaluated the swallowing pathologies of 16 patients with peripheral vagal paralysis, and compared their results with the data obtained in previous studies using a high-resolution manometer.20The residual pressure in the upper oesophageal sphincter was low in one-third of these patients and normal in the remaining two-thirds. Patients with aspiration had lower basal, residual and epiglottal upper oesophageal sphincter pressures. Patients with dysphagia had a lower epiglottal pressure and higher basal upper oesophageal sphincter pressure. The authors concluded that dysphagia was associated with decreased pharyngeal pressure, while aspir-ation was associated with decreased upper oesophageal sphinc-ter pressures.20
In this study, the minimum, maximum and mean upper oesophageal sphincter basal pressures were significantly lower in patients with unilateral vocal fold paralysis than in controls ( p < 0.001), likely due to inadequate muscle contrac-tion caused by paralysis and vocal fold immobility. Such hypo-tonicity of the sphincter during rest can lead to secondary problems such as laryngopharyngeal reflux. In support of this notion, reflux symptom index scores indicative of reflux were significantly higher in the study group.
Whereas the minimum upper oesophageal sphincter residual pressure of the study subjects was similar to that of the controls ( p = 0.201), the maximum and mean values were significantly lower ( p < 0.001). These results suggest that the upper oesophageal sphincter muscles also have diffi-culty during relaxation. Relaxation of the upper oesophageal sphincter depends on inhibition of the cricopharyngeal muscle and other upper oesophageal sphincter muscles; this relaxation opens the oesophagus to allow the passage of food. Our find-ings suggest that the upper oesophageal sphincter cannot attain sufficient relaxation, and this may hamper the passage of food. The measurement of relaxation pressure is difficult, and values can show marked variation among swallows. For this reason, the average of measurements obtained during multiple swallows was used in the present study. In addition, the pressure values obtained differ according to the type and quantity of food. In our study, both groups performed three dry swallows.
Domer et al. evaluated the upper oesophageal sphincter diameter in a barium swallow study and found that the diam-eter was smaller, but not significantly so, in patients with uni-lateral vocal fold paralysis.10 The cited authors also reported pharyngeal weakness in patients with unilateral vocal fold par-alysis, and concluded that this may contribute to swallowing impairment. Some studies have shown pharyngeal weakness to be involved in swallowing impairment in patients with uni-lateral vocal fold paralysis.7
Wilson et al. reported that pharyngeal pressures were higher in patients with unilateral vocal fold paralysis, albeit
Table 3.Manometric data
Manometric parameter Group Patients (n) Score (mean (SD)) P-value
UOS basal minimum pressure (mmHg)* Study 30 4.33 (2.90) <0.001
Control 24 34.16 (17.24)
UOS basal maximum pressure (mmHg)* Study 30 11.36 (4.27) <0.001
Control 24 47.54 (21.63)
UOS basal average pressure (mmHg)* Study 30 7.93 (3.49) <0.001
Control 24 40.66 (19.10)
UOS residual minimum pressure (mmHg)* Study 30 −8.76 (4.23) 0.201
Control 24 −6.33 (5.28)
UOS residual maximum pressure (mmHg)* Study 30 −3.96 (3.63) <0.001
Control 24 4.29 (7.78)
UOS residual average pressure (mmHg)* Study 30 −6.30 (3.78) <0.001
Control 24 −0.67 (5.73)
UOS relaxation time (seconds)† Study 30 0.51 (0.06) <0.001
Control 24 0.66 (0.11)
Pharynx peak pressure (mmHg)† Study 30 151.63 (16.93) <0.001
Control 24 117.37 (28.21)
not significantly so.19 Moreover, pharyngeal pressures were higher in patients with peripheral lesions and lower in those with central lesions. High-resolution manometric studies have yielded markedly different results.21Pinna et al. evaluated patients with vagal paralysis using a high-resolution manom-eter; the epiglottal pressure was higher in half of the patients.20 The epiglottal pressure was lower in patients with aspiration than in those without aspiration. Moreover, patients with dys-phagia had lower epiglottal pressure than did patients without dysphagia.
In our study, the mean peak pressure values obtained in the pharynx were significantly higher in patients with unilateral vocal fold paralysis compared with healthy controls. This is likely a result of compensation of the pharyngeal muscles. Such compensation may explain the high pharyngeal pressures detected in the present study. The healthy contralateral pha-ryngeal muscles and other muscles not innervated by the vagus may compensate for the weakness over time. We excluded acute stage patients from this study; we included only patients in whom paralysis had developed more than six months prior. However, the pharyngeal pressures reported in previous studies indicate that the mean values of the study and control groups in this study were normally distributed.22 Bhatia and Shah reported that the relaxation duration dur-ing swallowdur-ing was 0.6–1.0 seconds.23In our study, the relax-ation durrelax-ations were 0.51 seconds in the study group and 0.66 seconds in the control group ( p < 0.001). All patients were assessed during dry swallowing, as the amount of bolus can affect the relaxation duration. Wilson et al. reported that the durations of contractions in the pharynx and upper oesopha-gus were shorter in patients with unilateral vocal fold paralysis than in controls.19
Aspiration has been detected in 33–42 per cent of patients with unilateral vocal fold paralysis.6,7 Aspiration must be investigated and treated in such patients, as it may cause aspir-ation pneumonitis. Aspiraspir-ation was observed in 33.3 per cent of our patients. The penetration aspiration scale scores of the patients with unilateral vocal fold paralysis were significantly higher than those of the controls. The swallowing and dyspha-gia assessment scales, the Turkish version of the Eating Assessment Tool 10, and the MD Anderson questionnaire scores were significantly higher in the study group.
• The upper oesophageal sphincter is the most important area for oropharyngeal dysphagia
• The cricopharyngeal muscle is the upper oesophageal sphincter’s main structure and is innervated by the recurrent laryngeal nerve
• The upper oesophageal sphincter was evaluated in unilateral vocal fold paralysis patients to understand its effect on swallowing pathology in these patients
• Manometric evaluation revealed decreased basal and residual pressures and upper oesophageal sphincter relaxation duration
• Peak pharynx pressure during swallowing was higher on pharyngeal recordings
• The study data enabled identification of a hypotonic upper oesophageal sphincter area in unilateral vocal fold paralysis patients
This study has some limitations, the most important of which is the small number of patients enrolled. However, the formation of a homogeneous study group is difficult because
of the rarity of unilateral vagal paralysis. Manometric evaluation is not yet part of clinical examinations of these patients; thus, only volunteers were included in this study. In addition, the procedure is not tolerated by all patients. Electromyography was not utilised to determine the site and level of the vagal lesion causing vocal fold paralysis. However, this study aimed to evaluate dysphagia and the upper oesophageal sphincter in patients with vocal fold immobility. Additional studies with lar-ger numbers of patients are required to enhance our under-standing of swallowing problems in patients with unilateral vocal fold paralysis.
In conclusion, more than half of the unilateral vocal fold paralysis patients had dysphagia and one-third had aspiration. Upper oesophageal sphincter pressure values were lower in patients with unilateral vocal fold paralysis. Hypotonic sphinc-ter may contribute to swallowing impairment in patients with unilateral vocal fold paralysis.
Competing interests. None declared
References
1 Behrman A. Evidence-based treatment of paralytic dysphonia: making sense of outcomes and efficacy data. Otolaryngol Clin North Am 2004;37:75–104
2 Asik MB, Karasimav O, Birkent H, Merati AL, Gerek M, Yildiz Y. Airway and respiration parameters improve following vocal fold medialization: a prospective study. Ann Otol Rhinol Laryngol 2015;124:972–7
3 Spector BC, Netterville JL, Billante C, Clary J, Reinisch L, Smith TL. Quality-of-life assessment in patients with unilateral vocal cord paralysis. Otolaryngol Head Neck Surg 2001;125:176–82
4 Nayak VK, Bhattacharyya N, Kotz T, Shapiro J. Patterns of swallowing fail-ure following medialization in unilateral vocal fold immobility. Laryngoscope 2002;112:1840–4
5 Cates DJ, Venkatesan NN, Strong B, Kuhn MA, Belafsky PC. Effect of vocal fold medialization on dysphagia in patients with unilateral vocal fold immobility. Otolaryngol Head Neck Surg 2016;155:454–7
6 Leder SB, Suiter DM, Duffey D, Judson BL. Vocal fold immobility and aspiration status: a direct replication study. Dysphagia 2012;27:265–70 7 Jang YY, Lee SJ, Jeon JY, Lee SJ. Analysis of video fluoroscopic swallowing
study in patients with vocal cord paralysis. Dysphagia 2012;27:185–90 8 Leder SB, Ross DA. Incidence of vocal fold immobility in patients with
dysphagia. Dysphagia 2005;20:163–9
9 Tabaee A, Murry T, Zschommler A, Desloge RB. Flexible endoscopic evaluation of swallowing with sensory testing in patients with unilateral vocal fold immobility: incidence and pathophysiology of aspiration. Laryngoscope 2005;115:565–9
10 Domer AS, Leonard R, Belafsky PC. Pharyngeal weakness and upper esophageal sphincter opening in patients with unilateral vocal fold immo-bility. Laryngoscope 2014;124:2371–4
11 Sasaki CT, Kim YH, Stevenson H, Czibulka A. Motor innervation of the human cricopharyngeus muscle. Ann Otol Rhinol Laryngol 1999;108:1132–9
12 Mu L, Sanders I. The innervation of the human upper esophageal sphinc-ter. Dysphagia 1996;11:234–8
13 Hila A, Castell JA, Castell DO. Pharyngeal and upper esophageal sphincter manometry in the evaluation of dysphagia. J Clin Gastroenterol 2001;33:355–61
14 Herbella FA, Patti MG. Can high resolution manometry parameters for achalasia be obtained by conventional manometry? World J Gastrointest Pathophysiol 2015;6:58–61
15 Demir N, Arslan SS, Karaduman AA. Reliability and validity of the Turkish Eating Assessment Tool (T-EAT-10). Dysphagia 2016;31:644–9 16 Belafsky PC, Postma GN, Koufman JA. Laryngopharyngeal reflux
symp-toms improve before changes in physical findings. Laryngoscope 2001;111:979–81
17 Bhattacharyya N, Kotz T, Shapiro J. Dysphagia and aspiration with unilat-eral vocal cord immobility: incidence, characterization, and response to surgical treatment. Ann Otol Rhinol Laryngol 2002;111:672–9
18 Henderson RD, Boszko A, VanNostrand AW, Pearson FG. Pharyngoesophageal dysphagia and recurrent laryngeal nerve palsy. J Thorac Cardiovasc Surg 1974;68:507–12
19 Wilson JA, Pryde A, White A, Maher L, Maran AG. Swallowing performance in patients with vocal fold motion impairment. Dysphagia 1995;10:149–54 20 Pinna BR, Herbella FAM, de Biase N, Vaiano TCG, Patti MG.
High-resolution manometry evaluation of pressures at the pharyngo-upper esophageal area in patients with oropharyngeal dysphagia due to vagal par-alysis. Dysphagia 2017;32:657–62
21 Nativ-Zeltzer N, Logemann JA, Zecker SG, Kahrilas PJ. Pressure topog-raphy metrics for high resolution pharyngeal esophageal manofluorogra-phy—a normative study of younger and older adults. Neurogastroenterol Motil 2016;28:721–31
22 Leonard R, Rees CJ, Belafsky P, Allen J. Fluoroscopic surrogate for pharyn-geal strength: the pharynpharyn-geal constriction ratio (PCR). Dysphagia 2011;26:13–17
23 Bhatia SJ, Shah C. How to perform and interpret upper esophageal sphinc-ter manometry. J Neurogastroensphinc-terol Motil 2013;19:99–103