Demet ‹lhan ALGIN, O¤uz Osman ERD‹NÇ*, Özkan ALATAfi**, Aysun TOKER***,
Ömer ÇOLAK**, Setenay ÖNER****
Dumlup›nar Üniversitesi T›p Fakültesi, Nöroloji Anabilim Dal›, Kütahya
Eskiflehir Osmangazi Üniversitesi T›p Fakültesi, *Nöroloji, **Biokimya ve ****Bioistatistik Anabilim Dal›, Eskiflehir ***Yoncal› Fizik Tedavi ve Hidroterapi Hastanesi, Kütahya, Turkey
Effects of Oxcarbazepine on Plasma Homocysteine,
Vitamin B12, Folic Acid Levels
Okskarbazepinin Plazma Homosistein, Vitamin B12, Folik Asid De¤erleri Üzerine Etkisi
Address for Correspondence/Yaz›flma Adresi: Dr. Demet ‹lhan Alg›n, Dumlup›nar Üniversitesi T›p Fakültesi, Nöroloji Anabilim Dal›, Kütahya, Turkey E-mail: [email protected] Received/Gelifl tarihi: 02.04.2009 Accepted/Kabul tarihi: 28.04.2009
© Archives of Neuropsychiatry, Published by Galenos Publishing. All rights reserved. / © Nöropsikiyatri Arflivi Dergisi, Galenos Yay›nc›l›k taraf›ndan bas›lm›flt›r. Her hakk› sakl›d›r. ABSTRACT
Objective: It is known that plasma homocysteine (Hcy), folic acid (FA) and vitamin B12 (vit B12) levels are affected by antiepileptic drugs (AED). The aim of this study was to assess the effects of oxcarbazepine (OXC) on plasma Hcy, FA and vit B12 levels.
Method: A total of 42 epileptic outpatients receiving AED therapy were selected. Patients were divided into four different groups according to their medications. The patients of group 1 received OXC for less than 1 year (n=12), group 2 received OXC for more than 1 year (n=11), group 3 received OXC with valproate (VPA) for more than 1 year (n=9), group 4 received VPA monotherapy (n=10 ). A control group of 30 healthy subjects without any AED medication were also included. The plasma Hcy, FA and vit B12 levels of the groups were statistically compared with each other using one way ANOVA method. Results: The levels of plasma Hcy for the groups 1, 2, 3, 4 and the controls were 10.7±4.1 μmol/l, 15.5±10.7 μmol/l, 12.7±4.10 μmol/l, 10.2±2.9 μmol/l, 10.6±4.7 μmol/l respectively. No differences have been found between HS, FA and vit B12 levels statistically (p>0.05).
Conclusion: According to the findings of our study, it seems that OXC does not have any influence on plasma Hcy, FA and vit B12 levels when folate nutriture is adequate. (Archives of Neuropsychiatry 2009; 46: 49-51)
Key words: Homocysteine, folic acid, vitamin B12
ÖZET
Amaç: Homosistein(HS), folik asid (FA) ve vitamin B12’nin (vit B12) antiepileptik ilaçlardan (AED) etkilendi¤i bilinir. Biz bu çal›flma ile Okskarbazepinin (OXC) plazma HS, FA ve vit B12 de¤erlerine etkisini de¤erlenmeyi amaçlad›k. Yöntem: Toplam 42 epileptik hastam›zdan AED tedavi alanlar seçildi. Hastalar ald›klar› ilaçlara göre farkl› dört gruba ayr›ld›. Hastalar grup 1; 1 y›ldan daha az sürede OXC alanlar (n=12), grup 2; 1 y›ldan daha uzun süredir OXC alanlar (n=11), grup 3; 1 y›ldan daha uzun süredir OXC ile valproat (VPA) alanlar (n=9), grup 4; VPA monoterapsi alanlardan (n=10) olufluyordu. Kontrol grubu herhangi bir AED almayan 30 sa¤l›kl› bireyi içeriyordu. Gruplar aras›nda plazma HS, FA ve vitamin B12 de¤erleri birbirleri ile one way ANOVA metodu ile istatiksel olarak karfl›laflt›r›ld›.
Bulgular: Plazma HS de¤erleri gruplar 1, 2, 3, 4 ve kontroller aras›nda s›rayla 10.7±4.1 μmol/l, 15.5±10.7 μmol/l, 12.7±4.10 μmol/l, 10.2±2.9 μmol/l, 10.6±4.7 μmol/l’idi. HS, FA ve vit B12 de¤erleri aras›nda istatiksel olarak anlaml› bir fark bulunmad› (p>0.05).
Sonuç: Bizim çal›flmam›z›n bulgular›na göre, FA deste¤i yeterli oldu¤unda OXC’in plazma Hcy, FA ve vit B12 de¤erleri üzerinde herhangi bir etkisi gözlen-medi. (Nöropsikiyatri Arflivi 2009; 46: 49-51)
Anahtar kelimeler: Homosistein, folik asid, vitamin B12
Introduction
Elevated plasma concentrations of total Hcy are associated with increased risk of coronary artery disease, peripheral vascular disease and trombosis (1). Hcy is rapidly oxidized to Hcy and Hcy lactone in the plasma with a reaction that produces reactive oxygen species. These oxidative substances can cause endothelial damage that leads to atherosclerosis and vascular disease (2,3).
Hcy metabolized through the transsulfuration and transmethylation pathways, where folate, vitamin B-12 and vitamin B-6 are involved as a substrate or cofactor. A recent study identifies that vascular diseases are associated with epilepsy. Therefore, hyperhomocysteinemia may be caused by the deficiency of one of the vitamins or the combination, and these deficiencies have been frequently associated with the administration of AED (4).
Many studies conducted have shown that drug treatment such as lipid-lowering drugs, insulin, drugs used in rheumatoid arthritis, and anticonvulsants may have an adverse effect on plasma total Hcy concentrations. Although the underlying mechanisms for the effects on Hcy concentrations of these drugs remains unclear, it is believed that many drugs alter Hcy concentrations by interfering in the metabolism of folate or vitamins B12 or B6 or by altering renal function (5).
The aim of this study was to assess the effects of OXC on plasma HS, FA and vit B12 levels.
Method
The patients were classified according to International League against Epilepsy (Commission on Classification and Terminology of the International League Against Epilepsy, 1989).
A total of 42 patients with idiopathic epilepsy, followed at the Department of Neurology in Eskiflehir Osmangazi University Medical Faculty, were studied. Patients were divided into four different groups according to their medications. The patients of group 1 received OXC for less than 1 year (n=12), group 2 received OXC for more than 1 year (n=11), group 3 received OXC with valproate (VPA) for more than 1 year (n=9), group 4 received VPA monotherapy (n=10). A control group of 30 healthy subjects without any AED medication were also included. Presence of epilepsy due to ischemic stroke, history of cardiac and peripheral vascular disease, diabetes mellitus, anemia, pregnancy and renal or thyroid disease were exclusion criteria. Subjects using folic acid antagonists and vitamins, as well as vegetarians were also excluded.
Biochemical Analysis
Following an overnight fasting period, blood samples were obtained between 8 and 10 a.m. before receiving the morning dose of the anti-epileptic drug. Venous blood was taken from the antecubital vein in a sitting position. Serum was immediately separated by centrifugation after discharging. The supernatant was removed and stored at -20 °C until assay. Serum homocysteine, vit B12 and folic acid concentrations were measured by immunoassay method using commercial kits. Reference values for the kits were 5-15μmol/L for homocysteine, 3-17 ng/mL for fo-lic acid and 100-700 pg/mL for vit B12. The values above the 15 μmol/L were accepted as hyperhomocysteinemia.
Statistical Analysis
All statistical analyses were performed using the SPSS ver-sion 10.0.7 for Windows computer software package. A level of
p< 0.05 was considered statistically significant. Correlation of the total scores between two successive administrations was statistically measured with one way ANOVA method.
Results
Forty-two patients (20 women, 22 men) with a mean age of 45.8 years and 30 healthy controls (16 women, 14 men) with a mean age of 45 years were included in this study. Mean duration of disease was 5.4 years (3 month-8 years) in all patients. Gender and sex ratio were similar in the two groups.
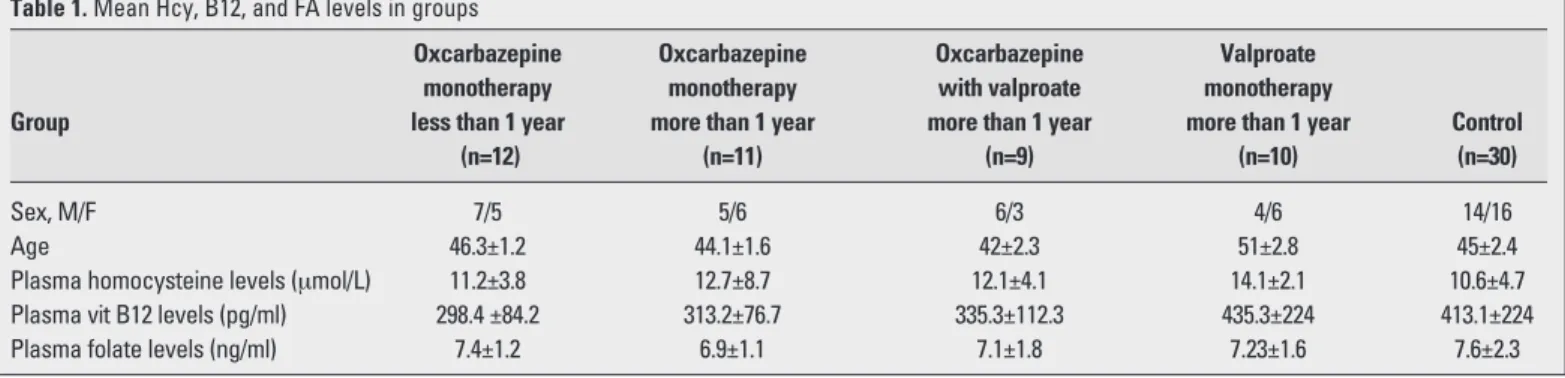
Mean HMC, FA, and vit B12 levels were determined as 10.6±4.7μmol/l (5-15 μmol/l), 7.6±2.3 ng/ml (3-17 ng/ml), 413.1± 224 pg/ml (180-900 pg/ml) in control group; 11.2±3.8 μmol/l, 7.4±1.2 ng/ml, 298.4±84.2 pg/ml in group 1, 12.7±8.7 μmol/l, 6.9±1.1 ng/ml, 313.2±76.7 pg/ml in group 2, 12.1±4.1 μmol/l, 7.1±1.8 ng/ml, 335.3±112.3 pg/ml in group 3 and 14.1±2.1 μmol/l, 7.23±1.6 ng/ml, 435.3±224 pg/ml in group 4, respectively (Table1).
Mean plasma homocysteine concentrations in patients who received VPA monotherapy more than 1 year were significantly higher than those in patients who received OXC. However, there were no significant differences found in concentrations of homocysteine between patients and controls (p>0.05).
No significant differences between the patients groups and controls were found in terms of plasma vit B12 and FA levels (p>0.05).
Discussion
AED have been shown to increase serum Hcy by lowering blood folate levels. The increase of Hcy levels in patients treated with CBZ and VPA are well documented. To our knowledge, small number of data are available concerning the link between Hcy levels and OXC treatment. OXC was developed through structural variation of carbamazepine in order to avoid side effects from metabolites, significant differences have emerged between the two drugs. The mechanism of action mainly involves blockade of sodium currents but differs from CBZ by modulating different types of calcium channels. In contrast to CBZ, which is oxidized by the cytochrome P-450 system, OXC undergoes reductive metabolism at its ketomoiety to form monohydroxy derivative, which is glucuronidated and excreted in the urine. Involvement of the hepatic cytochrome P450-dependent enzymes in the metabolism of OXC is minimal (6,7).
Table 1. Mean Hcy, B12, and FA levels in groups
Oxcarbazepine Oxcarbazepine Oxcarbazepine Valproate
monotherapy monotherapy with valproate monotherapy
Group less than 1 year more than 1 year more than 1 year more than 1 year Control
(n=12) (n=11) (n=9) (n=10) (n=30)
Sex, M/F 7/5 5/6 6/3 4/6 14/16
Age 46.3±1.2 44.1±1.6 42±2.3 51±2.8 45±2.4
Plasma homocysteine levels (μmol/L) 11.2±3.8 12.7±8.7 12.1±4.1 14.1±2.1 10.6±4.7
Plasma vit B12 levels (pg/ml) 298.4 ±84.2 313.2±76.7 335.3±112.3 435.3±224 413.1±224
Plasma folate levels (ng/ml) 7.4±1.2 6.9±1.1 7.1±1.8 7.23±1.6 7.6±2.3
Alg›n et al.
Effects of Oxcarbazepine on Plasma Homocysteine, Vitamin B12, Folic Acid Levels
Archives of Neuropsychiatry 2009; 46: 49-51 Nöropsikiyatri Arflivi 2009; 46: 49-51
Data regarding anti-epileptic drugs and their effect on Hcy metabolism have been controversial. Some studies reported elevated Hcy levels with CBZ (8,9,10,11) and VPA (8,9,11) use. Ho-wever, others reported no changes in Hcy levels with CBZ (12) and VPA (13,14).
Badiou et al. have found that plasma Hcy levels were significantly higher in CBZ-treated patients than in OXC-treated patients (15). In our study, no differences were determined between the patients with patients and control group (p>0.05). However Hcy levels were also elevated in patients treated with VPA monotherapy for more than 1 year, but did not reach significance (p>0.05).
Tamura et al found results similar to those observed in our study. They studied on plasm Hcy, FA, Vit B12 and VitB6 levels in patients taking phenytoin, lamotrigine, CBZ and VPA monotherapy. Hyperhomocysteinemia was observed only in seven of 62 patients (%11.3). Three of them were in phenytoine group, three of them were in CBZ and one was in lamotrigine group. Folate levels were higher while homocysteine levels were normal in VPA (4).
The literature on vit B12 status in patients under treatment with AEDs is controversial. Decreased (16), normal (9,12), and increased (4,17,18) vit B12 levels have been reported in patients with epilepsy. In our study, vit B12 serum concentrations did not differ significantly between patients and controls (p>0.05).
Folic acid promotes cellular growth and maturation of red blood cells, and deficiency of folic asid is associated with reduced growth and with megaloblastic anemia (19), eventhough megaloblastic changes in the bone marrow due to folate deficiency are found in a certain segment of patients receiving AED (2,19).
It is well known that FA deficiency occurs in some epileptic patients taking AED such as VA and CBZ. Although the mechanisms by which anticonvulsants induce FA deficiency are unclear, the proposed mechanisms can be summarized as interference with the intestinal absorption of FA, induction of enzymes in the liver and finally deplete FA, and interference with the metabolism of FA co-enzymes (11,20)
Data from several investigations showed that valproic acid is associated with either low (8,9) or normal (13) folic acid levels. Some studies also revealed that carbamazepine use was associa-ted with low folic acid status (8,9,10). In our study, no differences were determined between the patients and control group.
The reason for the difference between their findings and ours is unknown. It may be possible to attribute it to the difference in the practice of folic acid fortification for commonly consumed foods between countries. Our data suggest that hyperhomocysteinemia is not a serious clinical concern in epileptic patients when folate nutriture is adequate.
As a conclusion, findings of normal levels of plasma Hcy, vit B12 and FA levels in patients taking OXC is important. However
further studies are needed to give more detailed and more definitive results. OXC treatment could constitute an advantage in patients with other factors influencing Hcy levels and/or at high risk.
References
1. Barton DP, Rene M. Homocysteinemia and risk of atherosclerosis. The Endokrinologist 1998; 8:170-7.
2. D’angelo A, Selhub J. Homocysteine and thrombotic disease. Blood 1997; 90:1-11.
3. Hankey GJ, Eikelenboom P. Homocysteine and vascular disease. Lancet 1999; 354:407-13.
4. Tamura T, Aiso K, Johnston EK et al. Homocysteine, folate, vitamin B12 and vitamin B6 in patients receiving antiepileptic drug monotherapy. Epilepsy Research 2000; 40:7-15.
5. Dierkes J, Westphal S. Effect of drugs on homocysteine concentrations. Semin Vasc Med 2005; 5:124-39.
6. Schmidt D, Elger CE. How is oxcarbazepine different from carbamazepine? Nervenarzt 2004; 75:153-60.
7. May TW, Korn-Merker E, Rambeck B. Clinical pharmacokinetics of oxcarbazepine. Clin Pharmacokinet 2003; 42:1023-42.
8. Vilaseca MA, Monros E, Arthuch R et al. Anti-epileptic drug treatment in children: hyperhomocysteinemia. B-vitamins and the 677C→T mutation of the methylenetetrahydrofolate reductase gene. Eur J Paediatr Neurol 2000; 4:269-77.
9. Verrotti A, Pasceralla R, Trotta D et al. Hyperhomocysteinemia in children treated with sodium valproate and carbamazepine. Epilepsy Res 2000; 41:253-7.
10. Apeland T, Mansoor MA, Strandjord RE et al. Folate, homocysteine and methionine loading in patients on carbamazepine. Acta Neurol Scand 2001; 103:294-9.
11. Karabiber H, Sonmezgoz E, Ozerol et al. Effects of valproate and carbamazepine on serum levels of homocysteine, Vitamin B12, and folic acid. Brain Dev 2003; 25:113-5.
12. Schwaninger M, Ringle P, Winter R et al. Elevated plasma concentra-tions of homocysteie in antiepileptic drug treatment. Epilepsia 1999; 40:345-50.
13. Apeland T, Mansoor MA, Strandjord RE et al. Antiepileptic drugs as independent predictors of plasma total homocysteine levels. Epilepsy Res 2001; 47:27-35.
14. Kurul S, Unalp A, Yifl U. Homocysteine levels in epileptic children receiving antiepileptic drugs. J Child Neurol 2007; 22:1389-92. 15. Badiou S, Breton H, Peyriere H et al. Comparison of carbamazepine
and oxcarbazepine effects on aminothiol levels. Eur J Clin Pharmacol 2008; 64:83-7.
16. Krause KH, Bonjour JP, Berlit P et al. Effect of long-term treatment with antiepileptic drugs on the vitamin status. Drug Nutr Interact 1988; 5:317-43.
17. Dastur DK, Dave UP. Effect of prolonged anticonvulsant medication in epileptic patients: serum lipids, vitamins B6, B12, and folic acid, proteins, and fine structure of liver. Epilepsia 1987; 28:147-59. 18. May RB, Sunder TR. Hematologic manifestations of long-term
valproate therapy. Epilepsia 1993; 34:1098-101.
19. Morrell JM. Folic acid and epilepsy. Epilepsy Currents 2002; 2:31-4. 20. Sener U, Zorlu Y, Karaguzel O et al. Effects of common anti-epileptic
drug mono-therapy on serum levels of homocysteine, vitamin B12, folic acid and vitamin B6. Seizure 2006; 15:79-85.
Archives of Neuropsychiatry 2009; 46: 49-51 Nöropsikiyatri Arflivi 2009; 46: 49-51
Alg›n et al.