Although cochlear implantation has been almost a standard otological procedure worldwide, it may still create a dilem-ma for the surgeon in some unusual instances such as Seckel syndrome, the presence of a cardiac pacemaker for complete atrioventricular block, aural atresia, and in the presence of concurrent pathologies.
Seckel syndrome is a rare constellation of malformations which is presumably inherited as an autosomal recessive trait. The primary characteristic features of Seckel syndrome are: intrauterine and postnatal dwarfism, severe microcephaly, orofacial dysmorphism with characteristic “Bird-headed” appearance, prominent beaked nose, micrognathia, variable mental retardation and the presence of other malformations, especially of the skeleton (1,2). Abnormalities associated with cardiovascular, hematopoietic, endocrine and central nervous systems were also reported in Seckel syndrome (3).
Congenital aural atresia is a relatively common congenital anomaly in otology. It is estimated to occur in approximately 1 out of every 10,000 to 20,000 births. Hypoplasia of the exter-nal auditory caexter-nal, often associated with abnormalities of the auricle, middle ear and the inner ear structures, is the charac-teristic feature of aural atresia (4,5). It is unilateral in 70% to 85% of cases and the right ear is affected more frequently than the left (6). Intracranial arachnoid cysts are presumably con-genital malformations that are believed to form by the split-ting of the arachnoid membrane because of a circumscribed increased pulsation of the cerebrospinal fluid (7,8). Arachnoid cysts constitute approximately 1% of all intracranial lesions. The most common location of these lesions is the middle cra-nial fossa, with the posterior fossa being the second most com-mon location. The clinical entities presented above are rare, and cochlear implantation in these entities is an extraordinary Background: Although cochlear implantation has
been almost a standard otological procedure world-wide, it may still create a dilemma for the surgeon in some unusual instances such as Seckel syndrome, aural atresia and posterior fossa arachnoid cyst.
Case Report: Three extraordinary cases of cochlear
implantation were reported. The first case was a case of Seckel syndrome with a cardiac pacemaker due to complete atrioventricular block. The second case had posterior fossa arachnoid cyst that had retrosigmoid cyst removal and cochlear implantation simultane-ously. The last case had cochlear implantation in the ear with congenital aural atresia. All cases could be
im-planted successfully with full electrode insertion and good audiological outcome. Delayed facial paralysis that occurred in the patient with arachnoid cyst re-solved spontaneously.
Conclusion: This study addressed the efficiency of
cochlear implantation in cases of Seckel syndrome, complete atrioventricular block managed with cardiac pacemaker, congenital aural atresia and posterior fossa arachnoid cyst. In addition, the retrosigmoid approach and cochlear implantation can be performed simultane-ously.
Keywords: Cardiac pacemaker, cochlear implant,
con-genital aural atresia, seckel syndrome, subarachnoid cyst
Cochlear Implantation in Extraordinary Cases
1Department of Otorhinolaryngology, Gaziantep University Faculty of Medicine, Gaziantep, Turkey 2Department of Otorhinolaryngology, Medipol University Faculty of Medicine, İstanbul, Turkey
3Audiology Unit, Gazi University Faculty of Medicine, Ankara, Turkey
Fatih Çelenk
1, Raşit Cevizci
2, Şenay Altınyay
3, Yıldırım Ahmet Bayazıt
2Address for Correspondence: Dr. Raşit Cevizci, Department of Otorhinolaryngology, Medipol University Faculty of Medicine, İstanbul, Turkey Phone: +90 505 914 53 66 e-mail: [email protected]
Received: 24.10.2014 Accepted: 27.11.2014 • DOI: 10.5152/balkanmedj.2015.15937 Available at www.balkanmedicaljournal.org
condition. In this study, we presented the results of our experi-ence in the implanted patients who had these clinical condi-tions.
CASE PRESENTATION
In each of three pediatric cases, the child was evaluated before and after cochlear implantation after informed con-sent was taken. Audiological assessment included behav-ioral audiometry (with and without a hearing aid), auditory brain stem response (ABR), otoacoustic emissions (OAE), tympanometry and acoustic reflexes. Speech recognition assessments included Speech Awareness Threshold (SAT). The Evaluation of Auditory Responses to Speech (EARS) test battery was performed (Turkish version) 1, 3, 6, 12, 18, 24 and 36 months after implantation. The closed-set tests included the LiP, the Monosyllable Trochee Polysyl-lable Test (MTP) in three levels of difficulty (3, 6 and 12 mono-, bi- and polysyllabic words), a monosyllabic word test (4, 12 words) and a closed-set sentence level test with two levels of difficulty. Open-set tests were performed as early as 12 months after implantation. The open-set tests included a monosyllabic word test, the Languages-specific Sentence Test (L.S.) and the Glendonald Auditory Screen-ing Procedure (GASP). In the first few months followScreen-ing implantation, low level tests such as the LiP or the MTP-Test were performed.
Case 1
A 3-year-old boy was referred to our clinic with pre-lingual deafness. His antenatal history and familial properties were un-remarkable. He had typical clinical features of Seckel syndrome including dwarfism, mental retardation, severe microcephaly and bird-like appearance (Figure 1). He also had postnatal growth retardation and cardiac problems which were attributed to complete atrioventricular block. At the age of 1 his cardiac symptoms arose as part of a complete atrioventricular block and he was managed by a cardiac pacemaker. His family real-ized that he had a hearing problem because of his progressive apathy. Audiological evaluation revealed profound hearing loss bilaterally, and cochlear implantation was planned. A pediatric psychiatry consultation revealed that patient was mentally nor-mal. His temporal bone computed tomography (CT) revealed the patency of the cochlea with normal external ear canal, mas-toid, middle ear and inner ear. A magnetic resonance imaging (MRI) study could not be performed because of the cardiac pacemaker. Cochlear implantation with Medel (Pulsar) was ap-plied to the right ear (opposite site to the cardiac pacemaker) of the patient under general anesthesia. The patient was consulted by the pediatric cardiology department preoperatively and no cardiological contraindications were found. Since the patient had a cardiac pacemaker, a bipolar diathermy was preferred for safety. No significant electrocardiographic (ECG) changes were encountered during the operation. The patient was dis-charged 3 days after the operation. In the postoperative follow-up no audiological problem or cardiac complication occurred. He had device failure one year after implantation. Therefore, cochlear implant revision was performed under general anes-thesia. During the same operation, his cardiac pacemaker was also changed by the cardiac surgeons. Postoperative period was uneventful, and he was discharged from the hospital the day after the operation. Post-operative mean hearing level with co-chlear implant was 35 dB and SAT was 30 dB. He had steady improvement over time on LIP test, and the score improved to 100%. Monosyllabic-Trochee-Polysyllabic Test (MTP) score increased by 100% at 12 months after implantation.
Case 2
A 7-year-old female patient was referred to our clinic as a candidate of cochlear implantation owing to her congenital pre-lingual deafness. She had been using hearing aids since the age of 27 months. Her physical examination was normal. Audiological assessment revealed profound preoperative au-diological evaluation with a pure tone average (PTA) of 98 dB for the right and 105 dB for the left ear. There was an SAT of 90 dB for right and 95 dB for the left ear. Tympanometry was normal. Acoustic reflexes and OAEs were absent bilaterally. ABR testing revealed no reproducible waveforms.
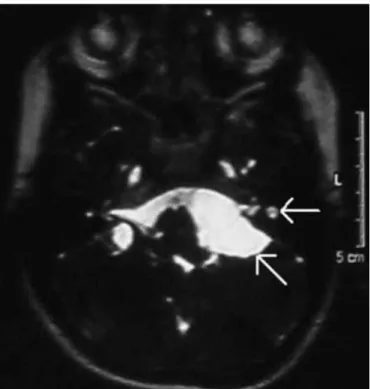
Her temporal bone computed tomography (CT) and magnet-ic resonance imaging (MRI) demonstrated cochlear patency. T2 weighted MRI scans revealed an 18 x 30 mm cystic mass which is suspicious of a subarachnoid cyst in the pontocer-ebellar angle as an incidental finding (Figure 2). It was press-ing the bulbus and stretchpress-ing the 7th-8th cranial nerve complex. The left retrosigmoid approach was performed under general anesthesia. An arachnoid cyst was removed via the retrosig-moid approach. The cochlear implantation was performed as a standard approach in the pre-sigmoid area. First of all, the sub-arachnoid cyst was excised. The cyst wall was attached to the 7th, 8th, 9th, 10th and 11th cranial nerves. It was dissected from nerves, leaving all of them intact. Then, the cochlear implant (Medel, Pulsar) was applied with full insertion of the elec-trodes. Reconstruction of retrosigmoid dura was performed by water-tight closure with 5-0 Vicryl sutures. The mastoid air cells and open air cells in the petrous bone were obliter-ated with bone wax. When the dural closure was considered to be water-tight, layered wound closure was performed. A tight mastoid dressing was maintained for 3 days after the opera-tion. Since we performed retrosigmoid craniotomy to excise the subarachnoid cyst, lumbar drainage was placed in order to prevent cerebrospinal fluid leak. On the seventh day of the postoperative period, a cerebrospinal fluid (CSF) leak began from the incision field. An area of wound breakdown was de-veloped which was managed by daily debridement and sterile dressings. CSF leakage and wound defect were improved
af-ter 10 days. On the tenth day of the postoperative period, left total peripheral facial palsy occurred. Since the facial nerve was spared both during excision of the cyst and cochlear im-plantation, this clinical entity was diagnosed as delayed facial palsy which sometimes occurs following otoneurological pro-cedures. Since the facial nerve was preserved, no diagnostics tests were carried out. The patient was followed-up without any medical or surgical treatment. Facial palsy resolved com-pletely within 3 months. One month after operation, the im-plant was activated without any problem.
After 12 months post-implantation, her mean hearing level was 35 dB and SAT was 30 dB. The child showed steady im-provement over time on LIP test and the score improved by 100%. The MTP score increased to 96%, the Monosyllable Closed-Set Test score improved to 88%, Open-Set Test score improved to 48%, Glendonald Auditory Screening Procedure (GASP) score improved to 30%, and the closed set sentence test A1 score improved to 72% 12 months after implantation.
Case 3
A 4 year-old girl was referred to our department for the treatment of hearing loss. She also had hypertellurism, saddle nose, and congenital aural atresia in the left ear. These findings could not be classified into a specific syndrome. The physical examination was otherwise normal. The patient had normal cognition. Audiological evaluation including otoacoustic em-misions and auditory brain stem response revealed profound hearing loss in both ears, and she did not benefit from ampli-fication with hearing aids. High-resolution CT of the temporal bone revealed aural atresia in the left ear with normal cochlea, large vestibule and lateral semicircular canal, and a sclerotic mastoid (Figure 3). The middle ear cleft was small in the left ear. The ossicles were dysplastic. The right ear was normal. Magnetic resonance imaging showed cochlear nerves and pat-ent cochlear lumens on both sides. Cochlear implantation was performed on atretic side using a Medel (Pulsar) device. Atret-ic ear was preferred in order to permit the patient to use a hear-ing aid on the contralateral ear. The incisions were performed in the retroauricular skin and periosteum, and the mastoid cor-tex was exposed. There was no tympanic ring. Mastoidectomy was performed following sinodural angle and tegmen tympani, and the body of the incus was exposed. The mastoidectomy was completed. There was a globular labyrinth and cleft-like middle ear. The ossicles were found to be deformed. There was stapes remnant in the ear. The remnants of the incus and malleus were removed. The tympanic segment of the facial nerve was identified, and the mastoid segment was exposed by drilling the bone over the mastoid segment of the nerve. The facial nerve was bending more anteriorly before the stylomas-toid foramen and leaning the temporal bone toward the tem-FIG. 2. Left ear of the child. Note the arachnoid cyst in the
poromandibular joint. The round window was fully exposed. The electrode was fully inserted through the round window as confirmed by transorbital and Stenver’s graphs. The external acoustic meatus was not opened. The incisions were closed. The atresia was not opened. The patient was discharged the day after the operation. Post-operative mean hearing level with the cochlear implant was 35 dB and SAT was 30 dB. She had steady improvement over time on LIP test, and the score improved to 100%. The MTP score increased by 100% 12 months after implantation.
DISCUSSION
Cochlear implants have been used to treat sensorineural hearing loss worldwide. There are many factors that should be considered for cochlear implant candidacy such as age, mental and physical health, audiological testing, cause and duration of deafness, capacity and ability to be reeducated, and social status (5,9). In addition, one may have to perform cochlear implantation in rare instances.
More than sixty cases of Seckel syndrome have been report-ed in the literature (3), but there is no publication regarding togetherness with congenital sensorineural hearing loss which was managed by cochlear implantation. This is the first report on cochlear implantation in Seckel syndrome. There are a few cases in the literature where cardiac problems were reported in Seckel syndrome. These problems include ventricular and
atrial septal defects, pulmonary artery atresia, overriding aorta, patent ductus arteriosus, atrial enlargement, atrioven-tricular canal defect and pulmonary hypertension (10-13). Our case had complete atrioventricular block and was managed by a cardiac pacemaker. To our knowledge, this is the first case of Seckel syndrome with complete atrioventricular block. Cochlear implantation in a patient with cardiac pacemaker has a distinctive position owing to the possibility of electri-cal interference. There is only one previous report of cochlear implantation in the presence of a cardiac pacemaker where no problem was encountered in the patient (14). This is the second case of cochlear implantation in a patient with cardiac pacemaker. Similarly, we did not encounter any cardiological problem both during the operation and after the “switch on” procedure of the cochlear implant. Both implant and cardiac pacemaker functioned without interference.
Although inner ear and the labyrinthine windows have different embryological development and origins from the external auditory canal, abnormalities such as an absence of the oval and round windows occur occasionally in aural atresia (15,16). Inner ear abnormalities are estimated to oc-cur in approximately 10% of cases of aural atresia (17). Ab-normalities of the facial nerve are often associated with ear malformations. There is a correlation between the degree of abnormalities of the auricle and the external auditory canal and the extent of facial nerve abnormality (4). In our patient with congenital aural atresia, there was no stapes and oval window, and the facial nerve was leaning the temporal bone toward the temporomandibular joint despite the presence of a normally appearing auricle. There is only one reported case of cochlear implantation in a patient with congenital aural atresia with successful results (6). To the best of our knowledge, our patient is the second case of congenital aural atresia that had cochlear implantation. The patient had atresia in the left ear while there was a patent external auditory canal on the right side. The atretic ear was preferred for implantation because the morphologies of both inner ears were similar on HRCT and MRI. In addition, the possibility of future improvements in the treatment of sensorineural hearing loss should be con-sidered, and it would be better to reserve the anatomically nor-mal ear for this possibility.
Most arachnoid cysts are located in the middle cranial fos-sa, particularly in the temporosylvian area (18). Localizations in the posterior fossa, the suprasellar cistern, the collicular region, the cerebellopontine angle and the cerebellar hemi-spheres are rare (7). Most cases are incidental imaging find-ings while symptomatic lesions may present with headache, seizure or focal neurological deficit (19). Some may be associ-ated with other clinical situations, such as a carotid jugular fis-tula, dissection of the contralateral carotid artery and hemifa-FIG. 3. Left sided congenital aural atresia in the child. Note the aural
cial atrophy and thus represent a generalized connective tissue disorders (20). When an arachnoid cyst is located in the poste-rior fossa, the presenting symptoms are frequently ontological (7). In addition, they may cause nonspecific symptoms includ-ing headache, dizziness and generalized unsteadiness (21). Unilateral or bilateral hypoacusia, vertigo and tinnitus have also been reported (7). CT and MRI are the preferred tools for the diagnosis of arachnoid cysts. The indications for surgery and the type of surgical treatment remain controversial topics (22). Arachnoid cysts are usually asymptomatic and conserva-tive management with regular follow-up based on radiologi-cal evaluation will identify indications for surgery. Surgiradiologi-cal indications include rapidly growing cysts, compression and displacement of the surrounding neurovascular structures and symptomatic patients. The surgical procedures include drain-age, total or partial removal of the cyst, shunting or fistuliza-tion of the cyst to the subarachnoid space (23). The posterior fossa arachnoid cyst can also be treated by endoscopic decom-pression (21). The cyst was removed in our patient because it was large, filling the pontocerebellar region and stretching the cranial nerves. Since the patient was a child, the cyst would possibly enlarge in time, and would necessitate surgery in the future. Two-stage operation was not necessary for this patient. Cochlear implantation and subarachnoid cyst excision were successfully applied with a single incision and a single anes-thetic procedure simultaneously. In addition, follow-up with MRI would not be practical because of MRI incompatibility of the cochlear implants. This is the first report of cochlear implantation in a patient with posterior fossa arachnoid cyst.
In conclusion, although cochlear implantation has been a standard surgery, it can be performed successfully in extraor-dinary cases as well. This study addressed the efficiency of cochlear implantation in cases of Seckel syndrome, complete atrioventricular block managed with cardiac pacemaker, con-genital aural atresia and posterior fossa arachnoid cyst. In ad-dition, retrosigmoid approach and cochlear implantation can be performed simultaneously.
Cochlear implantation can be performed in cases of Seckel syndrome, complete atrioventricular block managed with a cardiac pacemaker, congenital aural atresia and posterior fossa arachnoid cyst with successful results.
Ethics Committee Approval: N/A.
Informed Consent: Written informed consent was obtained from
the patients.
Peer-review: Externally peer-reviewed.
Author contributions: Concept - Y.A.B, F.Ç; Design - F.Ç.;
Su-pervision - Y.A.B, Resource - Ş.A, Y.A.B, F.Ç, R.C; Materials - Ş.A,
Y.A.B, F.Ç, R.C; Data Collection &/or Processing - Ş.A, Y.A.B, F.Ç, R.C; Analysis &/ or Interpretation - Ş.A, Y.A.B, F.Ç, R.C; Literature Search - Ş.A, Y.A.B, F.Ç, R.C; Writing - Y.A.B, F.Ç, R.C.; Critical Reviews - Ş.A, Y.A.B, F.Ç, R.C.
Conflict of Interest: No conflict of interest was declared by the
authors.
Financial Disclosure: The authors declared that this study has
re-ceived no financial support.
REFERENCES
1. Seymen F, Tuna B, Kayserili H. Seckel syndrome: report of a case. J Clin Pediatr Dent 2002;26:305-9.
2. Di Blasi S, Belvedere M, Pintacuda S, Di Blasi U, Ferotti N, Galante S, et al. Seckel’s syndrome: a case report. J Med 1993;24:75-96.
3. Arnold SR, Spicer D, Kouseff B, Lacson A, Gilbert-Barness E. Seckel-like syndrome in three siblings. Pediatr Dev Pathol 1999;2:180-7. [CrossRef]
4. Chang SO, Min YG, Kim CS, Koh TY. Surgical management of con-genital aural atresia. Laryngoscope 1994;104:606-11. [CrossRef]
5. Francis HW, Niparko JK. Cochlear implantation update. Pediatr
Clin North Am 2003;50:341-61. [CrossRef]
6. Lin K, Marrinan MS, Shapiro WH, Kenna MA, Cohen NL. Combined microtia and aural atresia: issues in cochlear implan-tation. Laryngoscope 2005;115:39-43. [CrossRef]
7. Haberkamp TJ, Monsell EM, House WF, Levine SC, Piazza L. Diagnosis and treatment of arachnoid cysts of the posterior fossa. Otolaryngol Head Neck Surg 1990;103:610-4.
8. Brooks ML, Mayer DP, Sataloff RT, Myers DL, Spiegel JR, Ruiz S. Intracanalicular arachnoid cyst mimicking acoustic neuroma: CT and MRI. Comput Med Imaging Graph 1992;16:283-5. [CrossRef]
9. Marsot-Dupuch K, Meyer B. Cochlear implant assessment: im-aging issues. Eur J Radiol 2001;40:119-32. [CrossRef]
10. Fukuda S, Morishita Y, Hashiguchi M, Taira A. Seckel’s syn-drome associated with atrial septal defect: a case report and re-view of the literature in Japan. Kyobu Geka 1991;44:411-3. 11. Howanietz H, Frisch H, Jedlicka-Kohler I, Steger H. Seckel dwarfizm
based on a personal case. Klin Padiatr 1989;201:139-41. [CrossRef]
12. Rappen U, von Brenndorff AI. Cardiac symptoms in 2 patients with Seckel syndrome. Monatsschr Kinderheilkd 1993;141:584-6. 13. O’Driscoll M, Ruiz-Perez VL, Woods CG, Jeggo PA, Goodship
JA. A splicing mutation affecting expression of ataxia-telangi-ectasia and Rad3-related protein (ATR) results in Seckel syn-drome. Nat Genet 2003;33:497-501. [CrossRef]
14. Triglia JM, Beliaeff M, Faugere G. Cochlear implantation in a pacemaker patient. Laryngoscope 1996;106:1184-6. [CrossRef]
15. Schuknecht HF. Congenital aural atresia. Laryngoscope 1989;99:908-17. [CrossRef]
16. Glasscock ME 3rd, Schwaber MK, Nissen AJ, Jackson CG. Management of congenital ear malformations. Ann Otol Rhinol
17. Cressman WR, Pensak ML. Surgical aspects of congenital aural atresia. Otolaryngol Clin North Am 1994;27:621-33.
18. Gallassi R, Ciardulli C, Ferrara R, Lorusso S, Galassi E, Luga-resi E. Asymptomatic large arachnoid cyst of the middle cra-nial fossa. A clinical and neuropsychological study. Eur Neurol 1985;24:140-4. [CrossRef]
19. Galassi E, Tognetti F, Gaist G, Fagioli L, Frank F, Frank G. CT scan and metrizamide CT cisternography in arachnoid cysts of the middle cranial fossa: classification and pathophysiological aspects. Surg Neurol 1982;17:363-9. [CrossRef]
20. Schievink WI, Piepgras DG, Nichols DA, (1995) Spontaneous carotid-jugular fistula and carotid dissection in a patient with
multiple intracranial arachnoid cysts and hemifacial atrophy: a generalized connective tissue disorder? J Neurosurg
1983:546-9. [CrossRef]
21. Ottaviani F, Neglia CB, Scotti A, Capaccio P. Arachnoid cyst of the cranial posterior fossa causing sensorineural hearing loss and tinnitus: a case report. Eur Arch Otorhinolaryngol 2002;259:306-8.
22. Samii M, Carvalho GA, Schuhmann MU, Matthies C. Arachnoid cysts of the posterior fossa. Surg Neurol 1999;51:376-82. [CrossRef]
23. Thinakara-Rajan T, Janjua A, Srinivasan V. Posterior fossa arachnoid cyst presenting with isolated sensorineural hearing loss. J Laryngol Otol 2006;120:979-82. [CrossRef]