https://doi.org/10.1177/1359105317742194 Journal of Health Psychology 2018, Vol. 23(14) 1769 –1780 © The Author(s) 2017 Article reuse guidelines: sagepub.com/journals-permissions DOI: 10.1177/1359105317742194 journals.sagepub.com/home/hpq
Introduction
According to the World Health Organization (WHO) (1996), menopause is defined as per-manent discontinuation of menstruation as a result of losing ovarian activity. It usually occurs at the age of 45–54 years and the mean age of onset is 51 years (Özkan, 2008). Physiological alterations during this period include vasomotor symptoms such as hot flushes, sweating, palpitation, headache and insomnia, musculoskeletal pain, depression, loss of attention, memory impairment, low sex drive, vaginal atrophy, and urinary problems during early period. In addition, there is an increased incidence of osteoporosis, cardiovas-cular diseases, and cancer during late period (Görgel and Çakıroglu, 2007).
Menopausal period is a specific time period associated with aging which may cause social
and psychological alterations, as well as biologi-cal alterations in females (Khoei et al., 2014). It is well-known that over 460 million women worldwide is above 50 years of age, and by the year 2030, it is estimated that 1.2 billion women would be at the menopausal or postmenopausal period, and it has been estimated to increase 4.7 million annually (Khoei et al., 2014). Therefore, menopausal and postmenopausal periods constitute approximately one-third of a
Sexual function and
quality-of-life-related problems during the
menopausal period
Ebru Gozuyesil , Sule Gokyildiz Surucu
and Sultan Alan
Abstract
This study aims to evaluate the relationship between the sexual functions and quality of life and the problems during menopausal period. This descriptive, cross-sectional study included a total of 317 women. The mean total Female Sexual Function Index score was 18.8 ± 8.7, while the mean total Sexual Quality of Life Questionnaire-Female score was 72.7 ± 13.7. Sexual dysfunction was found in 82 percent. There was a positive significant correlation between the total Female Sexual Function Index scores and total Sexual Quality of Life Questionnaire-Female scores (p < 0.05). Our study results suggest that women do not often experience serious menopausal symptoms, but have sexual dysfunction with a moderate sexual quality of life.
Keywords
menopause, nursing, quality of life, sexual dysfunction, Turkey
Cukurova University, Turkey
Corresponding author:
Ebru Gozuyesil, Abdi Sütcü Vocational School of Health Services, Cukurova University, Cukurova Universitesi Sağlık Hizmetleri Meslek Yüksekokulu Balcali Kampusu, Saricam, 01330 Adana, Turkey.
woman’s life. The most important condition to increase the quality of life in women above 50 years of age is, thus, to identify menopause and to overcome problems to live this period healthy (Kömürcü and İşbilen, 2011).
In many women with insufficient health care during menopausal period, chronic diseases develop, and quality of life is adversely affected due to being unable to cope with menopausal complaints (Nehir et al., 2009).
Female sexual function is an important com-ponent for the quality of life, which is affected by several physiological, psychological, and sociocultural factors (Khoei et al., 2014; Özerdoğan et al., 2009). During menopausal period, reduced circulating levels of estrogen, progesterone, and testosterone due to reduced ovarian functions may lead to reduced sexual drive, fantasy, arousal and orgasm capacity, vaginal dryness, and loss of lubrication. Defensive contraction of pubocoxygeal muscle due to atropy during postmenopausal period is one of the reasons of vaginismus and painful sexual contact (Özerdoğan et al., 2009). Sexual complaints which are frequently reported in females during this period are related to the altered sexual drive (Khoei et al., 2014; Özerdoğan et al., 2009). Female sexual dys-function (FSD) is a common health problem, which has an increasing prevalence (Özerdoğan et al., 2009).
FSD is defined as the persistent/recurring decrease in sexual desire or arousal, the diffi-culty/inability to achieve an orgasm, and/or the feeling of pain during sexual intercourse (Varma et al., 2005). Insufficient orgasm during sexual contact is a major component affecting the quality of life in females and is a health prob-lem which has an increasing prevalence with aging (Özerdoğan et al., 2009).
Although the prevalence of FSD is estimated to be 40–50 percent, the methodologies and the ratio according to the geographical distribution may significantly vary (Da Silva Lara et al., 2009). In recent years, the number of studies related to FSD increases day by day in Turkey. In a previous study of Özerdoğan et al. (2009) investigating sexual dysfunction, prevalence,
depression, and other related factors in women aged at 40–65 years, the prevalence of FSD was found to be 68.8 percent. In another study of Yangın et al. (2008), in which the relationship between sexual functions and depression during menopausal period was investigated, the inci-dence of FSD was 65 percent. In the study of Kömürcü and İşbilen (2011), which was con-ducted in 113 postmenopausal women, the inci-dence of FSD was found to be 57.5 percent. In healthy women, the incidence of FSD varies between 43.4 and 52.2 percent (Aslan et al., 2008; Cayan et al., 2016; Ege et al., 2010; Erbil, 2011; Tekin et al., 2014).
Considering the fact that sexual function and quality of life affect each other depending on age during menopausal period, in this study, we aimed to evaluate the relationship between menopausal problems and sexual functions and quality of life in women aged between 40 and 60 years.
Methods
Study design
This descriptive, cross-sectional study was con-ducted in females aged between 40 and 60 years who were admitted to Cukurova University, Balcalı Hospital, Menopause outpatient clinic.
Study sample
The universe of the study consisted of a total of 880 females who were admitted to Cukurova University, Balcali Hospital, Menopause outpa-tient clinic. The sample of the study consisted of 317 females who were admitted to the outpa-tient clinic between 15 October 2015 and 15 March 2016 and met the inclusion criteria of the study. In this study, 36 percent of females who were admitted to the Menopause outpatient clinic were included. The majority of females included in this study consisted of those who were admitted to the outpatient clinic for rou-tine examinations (i.e. mammography, bone densitometry, and blood tests) which must be done during the menopausal period.
Inclusion criteria were as follows: women aged between 40 and 60 years who accepted to participate in the study and lived in the city center, who were literate at least, who were married, who have menopausal symptoms, and who had active sexual life for the last month, were included to the study. The women with regular menstrual cycle and pregnant women were not included to the study.
The study inclusion criteria were determined according to the Stages of Reproductive Aging Workshop (STRAW) classification (Soules et al., 2001). According to this, pre-menopause: presence of at least one cyclic bleeding within past 3 months and absence of any change in menstrual cycle in the recent year; peri-meno-pause: presence of at least one menstrual bleed-ing within the last 3 months and presence of irregular menstrual cycle in the recent year; and post-menopause: absence of menstrual bleed-ing in the recent year (Soules et al., 2001). After giving brief information related to the aim and content of the study to each participant, a writ-ten informed consent was obtained.
Data collection
Data were collected using the Patient Information Form, Menopause Rating Scale (MRS), Female Sexual Function Index (FSFI), and Sexual Quality of Life Questionnaire-Female (SQLQ-F) form.
The patient information form
This form which was developed by the investi-gators was composed of a total of 32 questions. Questions for some descriptive, obstetric, and menopausal features of the women were included in the form.
MRS
The MRS scale, translated and validated by Schneider et al. (2000), includes a total of 11 items constituting menopausal complaints. For each item, there were options such as 0: absent, 1: mild, 2: moderate, 3: severe, and 4: very
severe. There was three subdimensions of the Likert scale as somatic, psychological, and uro-genital complaints (Heinemann et al., 2004; Schneider et al., 2000). The validity and reliabil-ity of the scale was performed by Gürkan (2005). The lowest score in the scale was “0,” while the highest score was “44.” Increased total scores in the scale indicate increased severity of the com-plaints and adverse effects on the quality of life. Internal consistency coefficient for all scale was found to be 0.84 (Çoban et al., 2008; Gürkan, 2005). The internal consistency coefficient for this study was found to be 0.86.
FSFI
The FSFI is a short interview form including 19 multi-dimensional items which could be answered by oneself and which was developed to evaluate basic dimensions of female sexual function including desire, arousal, lubrication, orgasm, satisfaction, and pain (Rosen et al., 2000; Wiegel et al., 2005).
In the scale which was developed by Rosen et al. (2000), there was score of six dimensions constituting sexual functions in addition to the total score. As six dimensions of sexual func-tion, sexual desire (two questions), arousal (four questions), lubrication (four questions), orgasm (three questions), sexual satisfaction (three questions), and pain during sexual con-tact (three questions) were interrogated. In the scale, the answers of the questions of each dimension of sexual function were scored in the range of 0–5 points. Increased scores indicate the improvement in sexual function. “0” score means that the individual had no sexual contact within the past month. The lowest total score that could be obtained in the scale was 2, the highest score was 36 (Rosen et al., 2000). Wiegel et al. (2005) has reported the cut-off value of FSFI to determine FSD as 26.55. The validity and reliability study to adapt the scale to Turkish was performed by Aygin and Aslan (2005). According to this, it was found that FSFI is a valid and reliable tool for evaluation of sexual function in Turkish women (Aygin and Aslan, 2005).
SQLQ-F
The SQLQ-F is a scale which the validity and reliability was performed by Symonds et al. (2005). The scale is a scale which could be used for all women above age 18 years; however, the validity and reliability study of the original scale performed in women aged between 18 and 65 years. The scale is an easily applied six-party Likert-type which can be answered by oneself, and it is composed of 18 items. It is expected that each item would be answered by consider-ing the sexual life within last 4 weeks. In the original scale, it is reported that each item could be scored between 1 and 6 or between 0 and 5. In this study, 1–6 score system (1 = completely agree, 2 = agree in a large extent, 3 = partially agree, 4 = partially disagree, 5 = disagree in a large extent, 6 = completely disagree) was used. The score interval of the scale is between 18 and 108. The high score in the scale demonstrates that the quality of sexual life is good (Symonds et al., 2005; Tugut and Gölbaşı, 2010).
The validity and reliability study for adapta-tion of the scale to Turkish was performed by Tugut and Gölbaşi (2010). According to this, SQLQ-F was found as a valid and reliable tool for evaluation of quality of sexual life in Turkish woman (Tugut and Gölbaşı, 2010).
In this study, the women were taken to a separate room during filling the questionnaire, and it was provided that the women filled the questionnaire by oneself. The questionnaire was completed at approximately 20–30 min.
Statistical analysis
Statistical analysis was performed using SPSS 22.0 software (SPSS Inc., Chicago, IL, USA). Descriptive data were expressed in mean, stand-ard deviation, and frequency. One-way analysis of variance (ANOVA) test was used for inter-group comparison of normally distributed quantitative data, while the Tukey’s honest sig-nificant difference (HSD) test was used to ana-lyze significant differences. In comparison of normally distributed parameters between two groups, the Student’s t-test was used and in
assessment of correlation between the parame-ters, the Pearson correlation analysis was used. The Cronbach’s alpha coefficient was calcu-lated for reliability of the scales. A p < 0.05 was considered statistically significant with a confi-dence interval (CI) of 95 percent.
Ethical considerations
The study was conducted in accordance with the principles of the Declaration of Helsinki. The study protocol was approved by Cukurova University Medicine Faculty Ethics Committee.
Results
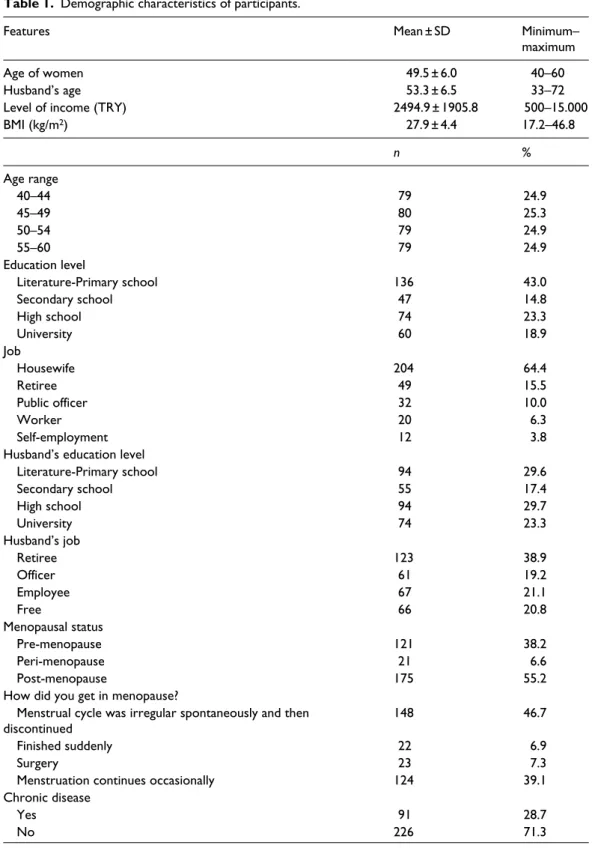
Demographic characteristics of the participants are shown in Table 1. The mean total MRS score was 15.4 ± 8.7 (Table 2), and the Cronbach’s alpha coefficient of the scale was 0.864.
The mean FSFI score of 82 percent of the women was below the cut-off value of 26.55. The mean total FSFI score was 18.8 ± 8.7, (Table 2), and the Cronbach’s alpha coefficient of the scale was 0.968. The mean total score of SQLQ-F was 72.7 ± 13.7 (Table 2), and the Cronbach’s alpha coefficient of the scale was 0.767.
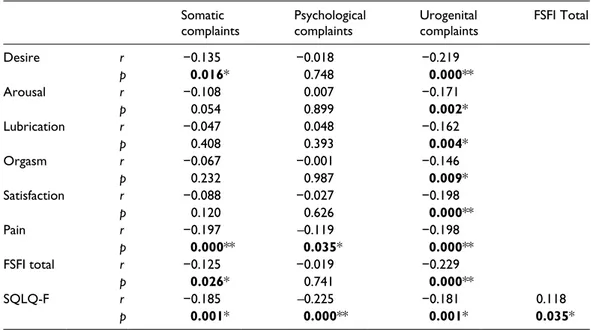
There was a negative correlation between the MRS subdimension, somatic complaints, and desire (p = 0.016), pain (p = 0.000) score, total FSFI score (p = 0.026), and total SQLQ-F (p = 0.001) score, indicating statistical signifi-cance (Table 3).
There was a negative correlation between the MRS subdimension, psychological com-plaints, and FSFI subdimension, pain score (p = 0.035) and total SQLQ-F score (p = 0.000), indicating statistical significance (Table 3). A negative significant correlation was found between MRS subdimension, urogenital com-plaints, and all subdimensions of FSFI (desire, arousal, lubrication, orgasm, satisfaction, and pain) (p < 0.05), total FSFI score (p = 0.000), and total SQLQ-F score (p = 0.001) (Table 3). However, a positive significant correlation was found between the total FSFI scores and total SQLQ-F scores (p = 0.035) (Table 3).
Table 1. Demographic characteristics of participants.
Features Mean ± SD Minimum–
maximum
Age of women 49.5 ± 6.0 40–60
Husband’s age 53.3 ± 6.5 33–72
Level of income (TRY) 2494.9 ± 1905.8 500–15.000
BMI (kg/m2) 27.9 ± 4.4 17.2–46.8 n % Age range 40–44 79 24.9 45–49 80 25.3 50–54 79 24.9 55–60 79 24.9 Education level Literature-Primary school 136 43.0 Secondary school 47 14.8 High school 74 23.3 University 60 18.9 Job Housewife 204 64.4 Retiree 49 15.5 Public officer 32 10.0 Worker 20 6.3 Self-employment 12 3.8
Husband’s education level
Literature-Primary school 94 29.6 Secondary school 55 17.4 High school 94 29.7 University 74 23.3 Husband’s job Retiree 123 38.9 Officer 61 19.2 Employee 67 21.1 Free 66 20.8 Menopausal status Pre-menopause 121 38.2 Peri-menopause 21 6.6 Post-menopause 175 55.2
How did you get in menopause?
Menstrual cycle was irregular spontaneously and then
discontinued 148 46.7
Finished suddenly 22 6.9
Surgery 23 7.3
Menstruation continues occasionally 124 39.1
Chronic disease
Yes 91 28.7
No 226 71.3
Table 2. Mean scores of the MRS, FSFI, and SQLQ-F. Minimum– maximum Mean ± SD MRS subdomains Somatic 0–16 5.7 ± 3.6 Psychological 0–16 6.3 ± 3.9 Urogenital 0–11 3.3 ± 2.6 Total 0–40 15.4 ± 8.7 FSFI subdomains Desire 0–6 2.6 ± 1.1 Arousal 0–6 2.7 ± 1.5 Lubrication 0–6 3.3 ± 1.8 Orgasm 0–6 3.1 ± 1.8 Satisfaction 0–6 3.4 ± 1.6 Pain 0–6 3.6 ± 2.0 Total 2–36 18.8 ± 8.7 SQLQ-F 27–106 72.7 ± 13.7
SD: standard deviation; MRS: Menopause Rating Scale; FSFI: Female Sexual Function Index; SQLQ-F: Sexual Qual-ity of Life Questionnaire-Female.
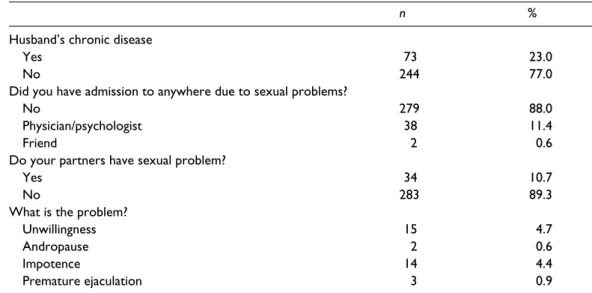
n %
Husband’s chronic disease
Yes 73 23.0
No 244 77.0
Did you have admission to anywhere due to sexual problems?
No 279 88.0
Physician/psychologist 38 11.4
Friend 2 0.6
Do your partners have sexual problem?
Yes 34 10.7
No 283 89.3
What is the problem?
Unwillingness 15 4.7
Andropause 2 0.6
Impotence 14 4.4
Premature ejaculation 3 0.9
BMI: body mass index; SD: standard deviation.
Table 1. (Continued)
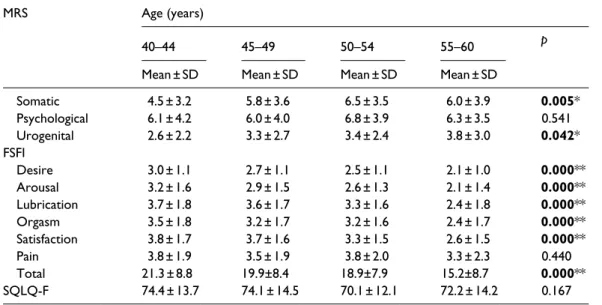
significant difference between the female age groups and all FSFI subdimensions, except for pain (p < 0.05) (Table 4).
However, there was no statistically significant difference between the female age groups and the mean SQLQ-F scores (p > 0.05) (Table 4).
Discussion
In this study, menopausal complaints and sex-ual functions and sexsex-ual qsex-uality of life in women aged between 40 and 60 years were evaluated.
In this study, when contacted with females during the data collection phase, the reason for admission to the outpatient clinic was usually routine examinations (i.e. blood tests, mam-mography, and bone densitometry) which must be done in the menopausal period rather than seeking solutions for menopausal complaints. Biological factors as well as psychological, social, and cultural factors need to be consid-ered for a better understanding of menopause. It has been shown that large differences both between and within cultures are influential in the menopause perception, in terms of the men-opausal behaviors and complaints in this period (Alan et al., 2016).
In addition, there was statistically significant difference between the female age groups and MRS subdimensions, somatic complaints (p = 0.005), and urogenital complaints (p = 0.042) (Table 4). Also, we observed a statistically
In the Turkish society, menopausal period is adversely perceived by women, and since they do not prefer drug treatment in coping with problems, their outpatient clinic controls mostly consist of having routine examinations. On the contrary, it has been reported that Asian, Arabian, and African women perceive menopause more positively and have a more smooth and comfortable period (Huang et al., 2010; Makuwa et al., 2015; Odıarı and Chambers, 2012). In a qualitative study con-ducted by us at the same hospital in Turkey and in similar studies conducted in Turkey, it has been shown that women mostly perceive menopause negatively (Alan et al., 2016; Sahin et al., 2011; Yangın et al., 2010). As a result, when a woman goes through meno-pause, menopause can be regarded as an unfa-vorable period for herself with the negative perceptions such as the end of fertility, the beginning of getting older, and the end of sex-uality. In this study, this characteristic of the Turkish society may be seen as a factor in our study findings.
In this study, we found that somatic and psy-chological complaints were more than the uro-genital complaints. The main somatic and psychological complaints are hot flush, night sweating, palpitation, and mental changes such as malaise and nervousness. In the study of Discigil et al. (2008) in which the perception of menopause was investigated, they found that the women at menopausal period most fre-quently correlated hot flush, night sweating, and nervousness with menopause. In the study of Chedraui et al. (2012), the incidence of depressive mood was 74.6 percent and the inci-dence of hot flush was 65.5 percent. In the study of Çoban et al. (2008), psychological com-plaints were experienced more intensely (Chedraui et al., 2012). Juang et al. (2005) found that the presence of hot flush was corre-lated with high anxiety and depression scores. In similar studies, somatic and psychological complaints were observed more than urogenital complaints (Nisar and Sohoo, 2010; Rahman et al., 2010; Shafie et al., 2011; Uludağ et al., 2014).
Table 3. Correlations between scale scores. Somatic
complaints Psychological complaints Urogenital complaints FSFI Total
Desire r −0.135 −0.018 −0.219 p 0.016* 0.748 0.000** Arousal r −0.108 0.007 −0.171 p 0.054 0.899 0.002* Lubrication r −0.047 0.048 −0.162 p 0.408 0.393 0.004* Orgasm r −0.067 −0.001 −0.146 p 0.232 0.987 0.009* Satisfaction r −0.088 −0.027 −0.198 p 0.120 0.626 0.000** Pain r −0.197 –0.119 −0.198 p 0.000** 0.035* 0.000** FSFI total r −0.125 −0.019 −0.229 p 0.026* 0.741 0.000** SQLQ-F r −0.185 –0.225 −0.181 0.118 p 0.001* 0.000** 0.001* 0.035*
FSFI: Female Sexual Function Index; SQLQ-F: Sexual Quality of Life Questionnaire-Female. Signifant values are marked in bold
In this study, total mean FSFI score was 18.86 ± 8.75 (Table 2). Sexual dysfunction was detected in 82 percent of the women included to the study. Sexual dysfunction is a frequently seen health problem which may reduce female quality of life, self-confidence, which may cause loneliness, and which may affect the interpersonel relationships (Ege et al., 2010). In the literature, FSD can be accepted as prevalent. In the studies in Turkey which were performed according to the FSFI scores, the incidence of FSD was found to be 70.9 percent in the study of Tekin et al. (2014), 68.8 percent in the study of Özerdoğan et al. (2009), and 65 percent in the study of Yangın et al. (2008). The incidence of FSD in similar studies in Turkey varies between 43.4 and 57.5 percent (Aslan et al., 2008; Cayan et al., 2016; Ege et al., 2010; Erbil, 2011; Kömürcü and İşbilen, 2011). When the interna-tional studies were examined, the incidence of FSD in postmenopausal women in Iran was 81.5 percent, the incidence of FSD in women in Equator was 72.4 percent, and it was 67 percent in Brazilian (Cabral et al., 2013; Chedraui et al.,
2012; Jamali et al., 2016). Based on these find-ings, we conclude that the incidence of FSD is high in similar international studies (Ishak et al., 2010; Nazarpour et al., 2016; Perez-Lopez et al., 2012; Rouzi et al., 2015; Safarinejad, 2006). The findings of this study are consistent with the literature data.
In this study, a negative significant correla-tion was found between all subdimension of MRS and total SQLQ-F score (p < 0.05). Furthermore, there was a positive significant correlation between total FSFI score and total SQLQ-F score (p = 0.039) (Table 3). As the menopausal complaints increase, sexual func-tions would disrupt and sexual quality of life in females with impaired sexual function would be negatively affected. In this study, the rela-tionship between menopausal problems experi-enced among women aged 40–60 years and sexual functions, and quality of life were evalu-ated. There are many studies addressing into the relationship between either menopausal lems and quality of life, or menopausal prob-lems and sexual function in the literature. Our
Table 4. Comparison of female age groups and scales.
MRS Age (years)
40–44 45–49 50–54 55–60 p
Mean ± SD Mean ± SD Mean ± SD Mean ± SD
Somatic 4.5 ± 3.2 5.8 ± 3.6 6.5 ± 3.5 6.0 ± 3.9 0.005* Psychological 6.1 ± 4.2 6.0 ± 4.0 6.8 ± 3.9 6.3 ± 3.5 0.541 Urogenital 2.6 ± 2.2 3.3 ± 2.7 3.4 ± 2.4 3.8 ± 3.0 0.042* FSFI Desire 3.0 ± 1.1 2.7 ± 1.1 2.5 ± 1.1 2.1 ± 1.0 0.000** Arousal 3.2 ± 1.6 2.9 ± 1.5 2.6 ± 1.3 2.1 ± 1.4 0.000** Lubrication 3.7 ± 1.8 3.6 ± 1.7 3.3 ± 1.6 2.4 ± 1.8 0.000** Orgasm 3.5 ± 1.8 3.2 ± 1.7 3.2 ± 1.6 2.4 ± 1.7 0.000** Satisfaction 3.8 ± 1.7 3.7 ± 1.6 3.3 ± 1.5 2.6 ± 1.5 0.000** Pain 3.8 ± 1.9 3.5 ± 1.9 3.8 ± 2.0 3.3 ± 2.3 0.440 Total 21.3 ± 8.8 19.9±8.4 18.9±7.9 15.2±8.7 0.000** SQLQ-F 74.4 ± 13.7 74.1 ± 14.5 70.1 ± 12.1 72.2 ± 14.2 0.167
MRS: Menopause Rating Scale; FSFI: Female Sexual Function Index; SQLQ-F: Sexual Quality of Life Questionnaire-Female; SD: standard deviation.
Signifant values are marked in bold One-way ANOVA test *p < 0.05; **p < 0.001.
study is more comprehensive than previous studies in this context.
In climacteric period, quality of life is affected by menopause type, vasomotor, uro-genital, psychosocial symptoms and sexual dysfunction observed during this period (De Lorenzi and Saciloto, 2006). In the study of Nisar and Sohoo (2010), as the menopausal complaints increased, the quality of life was negatively affected. As it was reported in the study of Safarinejad (2006), FSD had a major impact on quality of life and sexual dysfunction might also severely impair woman’s quality of life. In the study of Perez-Lopez et al. (2012) in which the sexual functions were evaluated in middle-aged women in Spain, 23.5 percent of women experienced menopausal symptoms intensely, and quality of life decreased and FSD increased in these women. In the study of Cabral et al. (2013) in which sexual functions in middle-aged women in Brazil were investi-gated, sexual dysfunction was 21.7 times more in women experiencing intense menopausal symptoms and sexual dysfunction was 6.6 times more in women with worse quality of life. The study by De Lorenzi and Saciloto (2006) showed that sexual desire reduced in 60.6 per-cent of the menopausal women (De Lorenzi and Saciloto, 2006). In another study in Iran, sexual activity decreased at a rate of 70.3 percent after menopause (Omidvar et al., 2011). These results indicate that sexual function and sexual quality of life is negatively affected in women during climacteric period.
In this study, there was statistically signifi-cant difference between the female age groups and subdimensions of MRS such as somatic complaints (p = 0.005), urogenital complaints (p = 0.042), and all subdimensions of FSFI except pain (p < 0.05) (Table 4). Similar to this study, Chedraui et al. (2012) found that somatic and urogenital complaints increased with increasing age. In the study of İnceboz et al. (2010) in which the quality of life was investi-gated in climacteric women, total mean MRS score in the women aged between 40 and 47 years was 15.2 ± 8.8 and the mean score increased to 17.6 ± 8.5 in women age >55 years.
In similar studies, the severity of menopausal complaints increased and quality of life decreased with increasing age (Shafie et al., 2011; Uludağ et al., 2014). In the literature, age is reported as the most important determi-nant of FSD (Aslan et al., 2008; Jaafarpour et al., 2013; Jonusiene et al., 2013). Reduced functional capacity in tissue and organs, increased number of births, and hormonal changes together with increasing age may lead development of FSD in advanced age, com-pared to the ones at early age (Özerdoğan et al., 2009). In this study, menopausal com-plaints increased and sexual functions were negatively affected with increasing age. In the study of Jonusiene et al. (2013) in which men-opausal symptoms, mood, and sexual func-tions were investigated in postmenopausal Lithuanian women, sexual function was found to be better in younger women, and there was a significant age-related impairment in sexual function in postmenopausal women. In the study of Aslan et al. (2008) which was con-ducted in 1009 healthy women to identify risk factors and prevalence of sexual function in Turkey, the incidence of reduced sexual func-tion according to age groups was found to be 22 percent for ages 20–29 years, to be 39.7 per-cent for ages 30–39 years, to be 50.2 perper-cent for ages 40–49 years, to be 71.3 percent for ages 50–59 years, to be 82.9 percent for ages 60–64 years, and 87.8 percent for ages 65 years and above. Cabral et al. (2013) reported that women at age 56–65 years have 7.3-fold more probability of sexual dysfunction than the women at age 40–45 years. Another study on the subject, the mean age of women who had FSD was significantly high (Cayan et al., 2004). In the study of Jaafarpour et al. (2013), the prevalence of FSD increased with age, from 22 percent in women aged <20 years to 75.7 percent in women aged 40–50 years (Jaaforpour et al., 2013). The findings in simi-lar studies are consistent (Chedraui et al., 2012; Khoei et al., 2014). In this study, similar to the literature, menopausal complaints and FSD were found to be increased with increas-ing age.
Conclusion
In conclusion, women at age between 40 and 60 years did not experience menopausal symp-toms very intensely; however, 82 percent had FSD and their sexual quality of life was mod-erate. Furthermore, it was found that meno-pausal complaints of women had significant effects on sexual function and sexual quality of life. It was found that menopausal symp-toms and FSFI scale scores were correlated with age and severity of menopausal symp-toms increase and the incidence of FSD increase with increasing age.
According to these results, it is recom-mended to provide appropriate environment for easily expressing sexual problems that they experienced and develop education pro-grammes to improve sexual health and to raise awareness related to sexuality in women at menopausal period in accordance with holistic nursing approach.
Findings of this study support the idea that, planning the trainings, which are to be pro-vided for women, particularly in the pre-men-opausal period is of utmost importance, due to the high rate of sexual dysfunction, increased menopausal symptoms with the advanced age, and increased negative effects related to sex-ual life, and it is also important to raise aware-ness before women start to experience menopausal problems. In addition, it is sug-gested that the trainings should be carried out in the outpatient setting, qualified nurses should be assigned for these services, and the partners should be included in these trainings, if possible.
Acknowledgements
The authors thank all the women who agreed to par-ticipate in the study. Data from this study were pre-sented as an oral presentation at the 24th World Congress on Controversies in Obstetrics, Gynecology & Infertility (COGI), 10–13 November 2016 in Amsterdam, The Netherlands. S.G.S. and S.A. designed the study; E.G. and S.G.S. collected, ana-lyzed data, and drafted the manuscript. E.G., S.G.S., and S.A. participated in the interpretation of the
result, revision, and finalizing the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of inter-est with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/ or publication of this article: This study was supported by research fund from Cukurova University with the project number TSA-2015-4763.
ORCID iD
Ebru Gozuyesil http://orcid.org/0000-0002-9193- 2182
References
Alan S, Gozuyesil E and Gokyildiz S (2016) Effects of menopause on the life of women who experi-ence hot flashes and their health-seeking behav-iours. International Journal of Caring Sciences 9(2): 542–550.
Aslan E, Beji NK, Gungor I, et al. (2008) Prevalence and risk factors for low sexual function in women: A study of 1,009 women in an outpatient clinic of a university hospital in Istanbul. The Journal of Sexual Medicine 6: 2044–2052.
Aygin D and Aslan FE (2005) The Turkısh adaptatıon of the Female Sexual Functıon Index. Turkiye
Klinikleri Journal of Medical Sciences 25:
393–399.
Cabral PU, Canario AC, Spyrides MH, et al. (2013) Determinants of sexual dysfunction among middle-aged women. International Journal
of Gynaecology and Obstetrics: The Official Organ of the International Federation of Gynaecology and Obstetrics 12: 271–274.
Cayan S, Akbay E, Bozlu M, et al. (2004) The preva-lence of female sexual dysfunction and poten-tial risk factors that may impair sexual function in Turkish women. Urologia Internationalis 72(1): 52–57.
Cayan S, Yaman Ö, Orhan İ, et al. (2016) Prevalence of sexual dysfunction and urinary incontinence and associated risk factors in Turkish women.
European Journal of Obstetrics & Gynecology and Reproductive Biology 203: 303–330.
Chedraui P, Perez-Lopez FR, Sanchez H, et al. (2012) Assessment of sexual function of mid aged Ecuadorian women with the 6 item Female Sexual Function Index. Maturitas 71: 407–412.
Çoban A, Nehir S, Demirci H, et al. (2008) Klimakterik dönemdeki evli kadınların eş uyumları ve menopoza ilişkin tutumlarının menopozal yakınmalar üzerine etkisi. F.Ü.
Sağlık Bilimleri Dergisi 22: 343–349.
Da Silva Lara LA, Useche B, Silva JCR, et al. (2009) Sexuality during the climacteric period.
Maturitas 62: 127–130.
De Lorenzi DR and Saciloto B (2006) Factors related to frequency of sexual activity of postmeno-pausal women. Revista da Associação Médica
Brasileira 52: 256–260.
Discigil G, Gemalmaz A, Tekin N, et al. (2008) Perception of menopause in a group of women living in Aydın and Muğla, Turkey. Turkiye
Klinikleri Journal of Medical Sciences 28:
494–499.
Ege E, Akın B, Yaralı Arslan S, et al. (2010) Sağlıklı kadınlarda cinsel fonksiyon bozukluğu sıklığı ve risk faktörleri. TUBAV Bilim Dergisi 3: 137–144.
Erbil N (2011) Prevalence and risk factors for female sexual dysfunction among Turkish women attending a maternity and gynecology outpatient clinic. Sexuality and Disability 29: 377–386. Görgel EB and Çakıroglu FP (2007) Menopozal
Dönemde Kadın. Ankara Üniversitesi Basımevi,
Ankara,Turkey: 1-4.
Gürkan ÖC (2005) Menopoz semptomları değer-lendirme ölçeğinin Türkçe formunun güvenirlik ve geçerliliği. Hemşirelik Forumu Mayıs– Haziran: 30–35.
Heinemann K, Ruebig A, Potthoff P, et al. (2004) The Menopause Rating Scale (MRS) scale: A methodological review. Health and Quality of
Life Outcomes 2: 45.
Huang KE, Xu L and Jaisamram U (2010) The Asian menopause survey: Knowledge, percep-tions hormone treatment and sexual function.
Maturitas 65(3): 276–283.
İnceboz U, Demirci H, Özbaşaran F, et al. (2010) Manisa bölgesinde yaşayan klimakterik dönem kadınlarında yaşam kalitesini etkileyen faktör-ler. Trakya Üniversitesi Tip Fakültesi Dergisi 27: 111–116.
Ishak IH, Low WY and Othman S (2010) Prevalence, risk factors, and predictors of female sexual dysfunction in a primary care setting: A sur-vey finding. The Journal of Sexual Medicine 7: 3080–3087.
Jaafarpour M, Khani A, Khajavikhan J, et al. (2013) Female sexual dysfunction: Prevalence and risk factors. Journal of Clinical and Diagnostic
Research 7: 2877–2880.
Jamali S, Javadpour S, Mosalanejad L, et al. (2016) Attitudes about sexual activity among post-menopausal women in different ethnic groups: A cross-sectional study in Jahrom, Iran. Journal
of Reproduction & Infertility 17: 47–55.
Jonusiene G, Zilaitiene B, Adomaitiene V, et al. (2013) Sexual function, mood and menopause symptoms in Lithuanian postmenopausal women. Clımacterıc 16: 185–193.
Juang KD, Wang SJ, Lu SR, et al. (2005) Hot flashes are associated with psychological symptoms of anxiety and depression in peri and post but not premenopausal women. Maturitas 52: 119–126. Khoei EM, Sheikhan F and Shamsalizadeh N (2014)
Menopause negatively impacts sexual lives of middle-aged Iranian women: A cross-sectional study. Journal of Sex & Marıtal Therapy 40(6): 552–600.
Kömürcü N and İşbilen A (2011) Adaptation of women to sexual life during the postmeno-pausal period. Turkish Journal of Urology 37: 326–330.
Makuwa GN, Rikhotso SR and Mulaudzi FM (2015) The perceptions of African women regarding natural menopause in Mamelodi, Tshwane dis-trict. Curationis 38(2): 1531.
Nazarpour S, Simbar M, Tehrani FR, et al. (2016) Sexual function and exercise in postmenopau-sal women residing in Chalous and Nowshahr, Northern Iran. Iran Red Crescent Medical
Journal 18(5): e30120.
Nehir S, Çoban A, Demirci H, et al. (2009) Menopozal belirtilerin ve evlilik uyumunun yaşam kalitesi üzerine etkisi. Cumhuriyet Tıp
Dergisi 31: 15–21.
Nisar N and Sohoo NA (2010) Severity of menopau-sal symptoms and the quality of life at differ-ent status of menopause: A community based survey from rural Sindh, Pakistan. International
Journal of Collaborative Research on Internal Medicine & Public Health 12: 118–130.
Odıarı E and Chambers AN (2012) Perceptions, attitudes, and self-management of natural
menopausal symptoms in Ghanaian women.
Health Care for Women International 33:
560–574.
Omidvar S, Bakouie F and Amiri FN (2011) Sexual function among married menopausal women in Amol (Iran). Journal of Midlife Health 2: 77–80.
Özerdoğan N, Sayıner FD, Köşgeroğlu N, et al. (2009) The prevalence of sexual dysfunction and depression and other factors associated in women 40 to 65 years old. Maltepe Üniversitesi
Bilim Ve Sanat Dergisi 2: 45–59.
Özkan S (2008) Klimakterium ve menopoz. In: Sirin A and Kavlak O (eds) Kadın Sağlığı. Bedray Basımevi, Istanbul, Turkey, p. 234.
Perez-Lopez FR, Fernandez-Alonso AM, Trabalon-Pastor M, et al.; MenopAuse Risk Assessment (MARIA) Research Group (2012) Assessment of sexual function and related factors in mid-aged sexually active Spanish women with the six-item Female Sex Function Index.
Menopause 19: 1224–1230.
Rahman SA, Zainudin SR and Mun VL (2010) Assessment of menopausal symptoms using modified Menopause Rating Scale (MRS) among middle age women in Kuching, Sarawak, Malaysia. Asia Pacific Family Medicine 9: 5. Rosen R, Brown C, Heiman J, et al. (2000) The
Female Sexual Function Index (FSFI): A mul-tidimensional self-report instrument for the assessment of female sexual function. Journal
of Sex & Marital Therapy 26: 191–208.
Rouzi AA, Sahly N, Sawan D, et al. (2015) The prevalence of sexual dysfunction in the female health care providers in Jeddah, Saudi Arabia.
Scıentıfıc Reports 5: 7905.
Safarinejad MR (2006) Female sexual dysfunction in a population-based study in Iran: Prevalence and associated risk factors. International Journal of
Impotence Research 18: 382–395.
Sahin NH, Bal MD, Boga NM, et al. (2011) Women’s perception of the menopause and hormone treatment: Barriers against hormone therapy.
Clımacterıc 14: 152–156.
Schneider HPG, Heinemann LAJ, Rosemeier HP, et al. (2000) The Menopause Rating Scale (MRS): Reliability of scores of menopausal complaints. Clımacterıc 3: 59–64.
Shafie KE, Farsi YA, Zadjali NA, et al. (2011) Menopausal symptoms among healthy, mid-dle-aged Omani women as assessed with the Menopause Rating Scale. Menopause 18: 1113–1119.
Soules MR, Sherman S, Parrott E, et al. (2001) Executive summary: Stages of Reproductive Aging Workshop (STRAW). Menopause 8(6): 402–407.
Symonds T, Boolell M and Quırk F (2005) Development of questionnaire on sexual qual-ity of life in women. Journal of Sex & Marital
Therapy 31: 385–397.
Tekin YB, Ural UM, Üstüner I, et al. (2014) Evaluation of female sexual function index and associated factors among married women in North Eastern Black Sea region of Turkey.
Turkish Journal of Obstetrics and Gynecology
11(3): 153–158.
Tugut N and Gölbaşı Z (2010) Cinsel Yaşam Kalitesi Ölçeği—Kadın Türkçe versiyonunun geçer-lik ve güvenirgeçer-lik çalışması. Cumhuriyet Tıp
Dergisi 32: 172–180.
Uludağ A, Güngör ANC, Gencer M, et al. (2014) Kadınların hayatındaki başka bir dönem: Menopoz ve menopozun yaşam kalitesine etkisi. Türk Aile Hekimliği Dergisi 18: 25–30. Varma GS, Oguzhanoglu NK, Karadag F, et al.
(2005) The relationship between depression and anxiety levels and sexual satisfaction for natu-ral and surgical menopause. Clinical Psychiatry
Journal 8: 109–115.
Wiegel M, Meston C and Rosen R (2005) The Female Sexual Function Index (FSFI): Cross-validation and development of clinical cutoff scores.
Journal of Sex & Marital Therapy 31: 1–20.
World Health Organization (WHO) (1996) Research
on the menopause in the 1990s. WHO technical
report series no. 866. Geneva: WHO. Available at: http://whqlibdoc.who.int/trs/WHO_TRS_866. pdf (accessed 10 September 2016).
Yangın HB, Kukulu K and Sözer GA (2010) The per-ception of menopause among Turkish women.
Journal of Women & Aging 22: 290–305.
Yangın HB, Sözer GA, Sengün N, et al. (2008) The relationship between depression and sexual function in menopause period. Maturitas 61: 233–237.