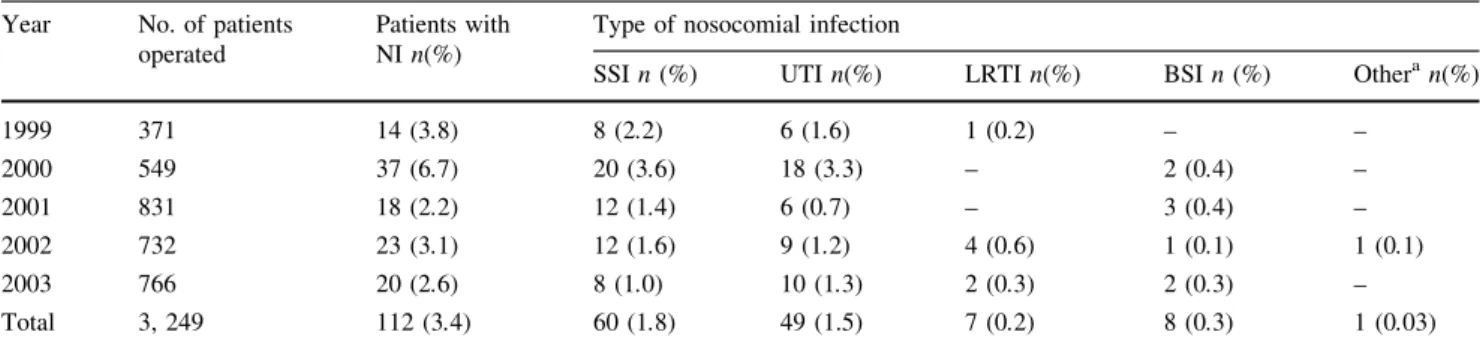
Five-year surveillance of nosocomial infections following orthopedic surgery in a private medical center
Tam metin
Şekil

Benzer Belgeler
Objective: The purpose in this research is to evaluate hand hygiene the attitudes of healthcare staff working in intensive care unit of state hospital of a
The goals of this research are to understand the types of contracting between the hospital and the equipment supplier, to explore whether or not different types of hospitals
Background: We used 4-year nationwide population-based data to explore the volume-outcome relationships for lung cancer resections in Taiwan and to determine whether there is
In addition, the future of medical education will be in the field of scientific research, and the importance of patient safety is discussed while adapting to new technologies
The IV Insertion Site in the Pediatric Patient Evaluation Form: This form developed by researchers includes questions about age, gender, disease diagnosis, total patient days,
As a result, nearly half of the patients were found to not to have an education on “Catheter-Associated Urinary Tract Infections”, not to have adequate knowledge about catheter
Çalışmanın diğer bir sonucuna göre çalışanların cinsiyetlerinin örgütsel iklim ve bağlılık düzeylerinde bir farklılık oluşturup oluşturmadığı
The second reason is that teenagers clash with their peers or teachers because they have conflicting opinions; Third is the diversity of relationships between parents and
