ORIGINAL ARTICLE
Do C-reactive protein level, white blood cell count, and pain
location guide the selection of patients for computed tomography
imaging in non-traumatic acute abdomen?
E. Ozan1&G.K. Atac1&T. Evrin2&K. Alisar1&L.O. Sonmez2&A. Alhan3
Received: 1 July 2016 / Accepted: 26 August 2016 / Published online: 2 September 2016 # American Society of Emergency Radiology 2016
Abstract The value of abdominal computed tomography in non-traumatic abdominal pain has been well established. On the other hand, to manage computed tomography, appropri-ateness has become more of an issue as a result of the con-comitant increase in patient radiation exposure with increased computed tomography use. The purpose of this study was to investigate whether C-reactive protein, white blood cell count, and pain location may guide the selection of patients for com-puted tomography in non-traumatic acute abdomen. Patients presenting with acute abdomen to the emergency department over a 12-month period and who subsequently underwent computed tomography were retrospectively reviewed. Those with serum C-reactive protein and white blood cell count mea-sured on admission or within 24 h of the computed tomogra-phy were selected. Computed tomogratomogra-phy examinations were retrospectively reviewed, and final diagnoses were designated either positive or negative for pathology relating to presenta-tion with acute abdomen. White blood cell counts, C-reactive protein levels, and pain locations were analyzed to determine whether they increased or decreased the likelihood of produc-ing a diagnostic computed tomography. The likelihood ratio for computed tomography positivity with a C-reactive protein level above 5 mg/L was 1.71, while this increased to 7.71 in patients with combined elevated C-reactive protein level and
white blood cell count and right lower quadrant pain. Combined elevated C-reactive protein level and white blood cell count in patients with right lower quadrant pain may represent a potential factor that could guide the decision to perform computed tomography in non-trau-matic acute abdomen.
Keywords Acute abdomen . Computed tomography . C-reactive protein . White blood cell count . Pain location
Introduction
Acute abdominal pain represents approximately 10 % of emergency department admissions worldwide [6]. Signs and symptoms, clinical examination, and laboratory findings are often insufficient to correctly diagnose the underlying cause but may help to narrow the differential diagnosis. Imaging plays an important role in the evaluation of patients with acute abdominal pain. Computed tomography (CT) is a useful tool in this scenario with high diagnostic accuracy [17,20]. It has high sensitivity and specificity for evaluating most common emergent conditions such as acute appendicitis and diverticu-litis. However, due to concerns about CT radiation and the emerging requirement for more economically effective utili-zation of CT, strategies to manage CT appropriateness have become more of an issue.
Recent studies have demonstrated substantial increases in CT utilization in various institutions and countries worldwide [12,15,18]. Furthermore, numerous studies have pointed out the increasing use of CT at a higher rate in the emergency department (ED) than in other settings and at a rate far exceed-ing the increase in ED patient volume [3,11].
Justification represents one of the three fundamental prin-ciples of radiation protection [8]. In a recent study that * E. Ozan
1
Department of Radiology, Ufuk University School of Medicine, Balgat, Ankara, Turkey
2
Department of Emergency Medicine, Ufuk University Faculty of Medicine, Ankara, Turkey
3 Department of Statistics, Ufuk University Faculty of Arts and
investigated the rate of unjustified CT scans, it was reported that 37 % of abdominal CT scans were unjustified and could be replaced by non-ionizing imaging modalities such as ultra-sound (US) and magnetic resonance imaging (MRI) [14].
When the rising concerns about the radiation administered during CT examination and the increase in CT utilization in the ED are considered, it is obvious that the benefit to risk ratio for any patient will be driven by the appropriateness of the CT examination. Thus, it is essential to correctly identify the pa-tients in whom abdominal CT will be most beneficial in the clinical setting of non-traumatic acute abdomen (NTAA). Therefore, the purpose of our study was to evaluate whether C-reactive protein (CRP), white blood cell (WBC) count, and pain location may serve as a guide for the selection of patients for computed tomography (CT) imaging in this clinical setting.
Material and methods
This single-center retrospective study was conducted in the Radiology and Emergency Medicine Departments of our in-stitution. The study protocol was approved by the institutional ethical committee, and informed consent was obtained from all individual participants included in the study by either phone calls or patient visits.
Patients
Patients presenting to the ED with symptoms of acute abdom-inal pain over a 12-month period and who subsequently underwent abdominal CT were retrospectively reviewed. A total of 231 patients were admitted with a diagnosis ofBacute abdomen^ related to abdominal trauma or other causes. Patients with a history of trauma (n = 79), recent surgery (n = 26), inflammatory bowel disease (n = 9), and known malignancy (n = 10) were excluded. Hospital laboratory in-formation system (LIS) records were then reviewed, and pa-tients with serum CRP level and WBC count measured on admission or within 24 h of the abdominal CT were subselected yielding a final cohort of 101 patients. Pain loca-tions were noted by reviewing ED charts and/or hospital med-ical records. CRP levels, WBC counts, and pain locations were analyzed to determine whether they increased or de-creased the likelihood of producing a diagnostic CT.
Imaging technique and image analysis
All CT exams were performed on a 16-row multi-detector CT scanner (Lightspeed 16, General Electric, Milwaukee, USA). All the CT scans were interpreted retrospectively, based on the consensus of two national board-certified radiologists, who knew the patients all had NTAA; however, they were blinded
to the original CT reports and clinical and laboratory findings. Each study was recruited from our Picture Archiving and Communication System (Centricity PACS, GE Healthcare, General Electric, Milwaukee, USA) and loaded to a dedicated workstation with three 3-MP monitors (BARCO, Brussels). Final CT diagnoses were designated either positive or nega-tive based on CT findings for pathology relating to presenta-tion with acute abdomen. After complepresenta-tion of the image anal-ysis procedure, ED charts and/or hospital computerized med-ical records of all patients were retrospectively reviewed in order to ensure that CT diagnoses were in compliance with final diagnoses.
Laboratory analysis
Hospital LIS records were reviewed. WBC count (103/μL) obtained on complete blood count (CBC) analyses and CRP levels (mg/L) were noted. Laboratory analyses were per-formed using an Abbott ARCHITECT c8000 Clinical Chemistry Analyzer for all patients. Threshold values of WBC count and CRP level were 10.2 × 103/μL and 5 mg/L, respectively.
Statistical analysis
SPSS (IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp.) was used for statistical analysis. Baseline characteristics were analyzed using descriptive sta-tistics. Normality of data for continuous variables was ana-lyzed using Kolmogorov-Smirnov test. Data were described using mean and standard deviation for continuous normal dis-tributions; median, min, and max for non-normal distribu-tions; and frequency for categorical variables. Comparisons between groups were performed using Student’s t test for con-tinuous normally distributed data, Mann–Whitney test, or Kruskal–Wallis test for nonparametric variables with two or more than two groups, respectively. Pearson’s chi-square test was employed to compare categorical variables between sub-groups. The criterion for statistical significance wasp < 0.05. A CRP level of >5 mg/L and a WBC count of >10.20 × 103/ μL were considered elevated above the reference standard. Pain locations were determined as eight main groups being right lower quadrant (RLQ), right upper quadrant (RUQ), left lower quadrant (LLQ), left upper quadrant (LUQ), flank (right or left), epigastric, pelvic, and diffuse abdominal pain, respectively.
Results
One hundred one patients [56 (55.4 %) women; mean age 42.8 ± 19.8] were included in this study. Sixty percent of patients (61/101) had a CT scan with both oral and intravenous
(IV) contrast material, 36 % (36/101) had IV contrast material only, and 4 % (4/101) had neither oral nor IV contrast material.
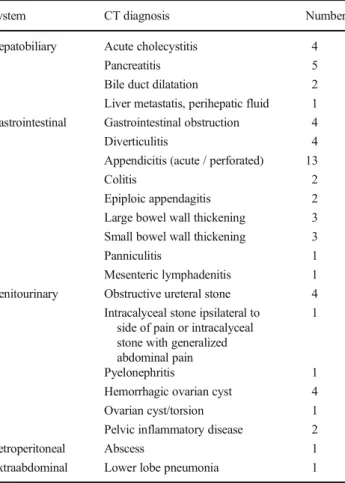
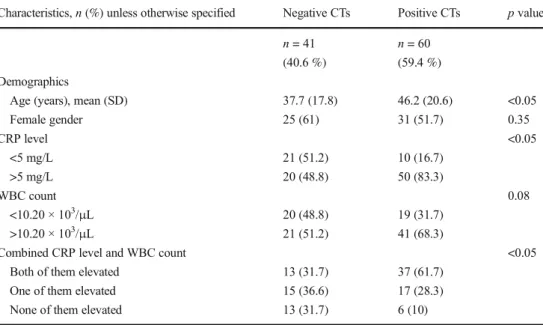
Of the study population, 60 (59.4 %) had positive CTs. Diagnoses found on CT are listed in Table 1. Thirty-one (54.4 %) women and 29 (64.4 %) men had positive CTs. No statistically significant difference was found between women and men in terms of positive and negative CT diagnoses (p = 0.417). Mean age was 46.2 ± 20.6 (minimum–maximum 17–88) and 37.7 ± 17.8 (minimum-maximum 16–78) in pos-itive and negative CT groups, respectively. Age was found to be significantly different between positive and negative CT groups (p < 0.05). When CRP levels and WBC counts were considered as elevated or normal, a significant difference was found between positive and negative CT groups in terms of CRP level (p < 0.05), while in terms of WBC count, no sig-nificant difference was found between groups (p = 0.83). When the patients were grouped considering combined CRP levels and WBC counts, a significant difference was found between positive and negative CT groups (p < 0.05). Cohort characteristics classified by CT diagnoses are listed in Table2. In the total study cohort, an elevated WBC count resulted in a sensitivity of 68 % (95 % CI 55–78) and a specificity of
48 % (95 % CI 34–63), an elevated CRP level resulted in a sensitivity of 83 % (95 % CI 71–90) and a specificity of 51 % (95 % CI 36–65), and combined elevated CRP level and WBC count resulted in a sensitivity of 86 % (95 % CI 72–93) and a specificity of 50 % (95 % CI 32–67) for the positive CT findings relating to presentation with acute abdomen. The likelihood ratios for CT positivity were found to be 1.33, 1.71, and 1.72, with an elevated WBC count, an elevated CRP level, and combined elevated CRP level and WBC count, respectively.
The most common pain location was RLQ pain, while LUQ pain was the least common. When the patients were grouped by pain location, the difference between positive and negative CTs was found to be significantly different (p < 0.05). Of the eight pain locations, RLQ and LLQ pain produced the highest number of positive CTs, while pelvic pain produced the lowest number of positive CTs (Table3).
In patients with RLQ pain, CRP levels were found to be significantly different between positive and negative CT groups (p < 0.05), while in patients with other pain locations, no significant difference was found between groups (as all patients had positive CTs, statistical analysis could not be performed for flank pain) (Table 4). In patients with RLQ pain, an elevated CRP level resulted in a sensitivity of 86 % (95 % CI 67–95) and a specificity of 78 % (95 % CI 52–92) and combined elevated CRP level and WBC count resulted in a sensitivity of 85 % (95 % CI 60–95) and a specificity of 88 % (95 % CI 56–98) for the positive CT findings relating to presentation with acute abdomen. The likelihood ratio for CT positivity in patients with RLQ pain and an elevated CRP level was found to be 4.06, while this increased to 7.71 with a combined elevated CRP level and WBC count.
Discussion
In recent years, CT utilization in the ED has increased greatly [1,3]. It was reported that patients presenting to an ED with abdominal or flank pain were nearly ten times more likely to have CT imaging in 2007 than in 1996 [10]. Although the value of abdominal CT in the ED for patients with non-traumatic abdominal pain has been well established, to man-age CT appropriateness has become more of an issue as a result of the concomitant increase in patient radiation expo-sure with increased CT use. Identification of the appropriate setting to perform CT in patients with acute abdominal pain, thus reducing unnecessary radiation exposure and maximizing the benefit to the patient, is essential. This study sought to investigate whether CRP level, WBC count, and pain location increased or decreased the likelihood of producing a diagnos-tic CT and thus guide the selection of patients for CT imaging in the clinical setting of NTAA.
Table 1 Distribution of CT diagnoses depending on abdominal anatomical location and systems
System CT diagnosis Number
Hepatobiliary Acute cholecystitis 4
Pancreatitis 5
Bile duct dilatation 2 Liver metastatis, perihepatic fluid 1 Gastrointestinal Gastrointestinal obstruction 4
Diverticulitis 4
Appendicitis (acute / perforated) 13
Colitis 2
Epiploic appendagitis 2 Large bowel wall thickening 3 Small bowel wall thickening 3
Panniculitis 1
Mesenteric lymphadenitis 1 Genitourinary Obstructive ureteral stone 4
Intracalyceal stone ipsilateral to side of pain or intracalyceal stone with generalized abdominal pain
1
Pyelonephritis 1
Hemorrhagic ovarian cyst 4 Ovarian cyst/torsion 1 Pelvic inflammatory disease 2
Retroperitoneal Abscess 1
Pain location may provide an additional clue in the diag-nostic workup of patients presenting with acute abdominal pain. It was reported that a significant diagnostic correlation exists between pain locations in the right upper and lower quadrant with a diagnosis of cholecystitis and acute appendi-citis, respectively [13].
Although the lack of specificity and low diagnostic accu-racies are well known [5,21], the inflammatory markers, CRP level and WBC count, are routinely encountered in this clin-ical scenario. A recent study investigated the predictive role of CRP for abdominopelvic CT findings in patients with acute abdomen [4]. The authors divided CRP levels into quartile thresholds in order to facilitate statistical evaluation and con-sidered all CRP values less than 5 to be negative. In contrast, we did not consider quartile thresholds in order to avoid a bias by interrupting the continuous nature of the variable, as was also stated by the authors of the study. It was suggested that increasing levels of CRP predict positive findings on CT with
increasing likelihood. A CRP level in the range of 27.2– 130 mg/L had a sensitivity and specificity of 31.4 and 90.9 % with a likelihood ratio of 3.45, respectively. Our study also investigated WBC count and pain location. In our study, elevated CRP levels in patients with RLQ pain had a sensitiv-ity and specificsensitiv-ity of 86 and 78 % with a likelihood ratio of 4.06, while these increased to 85 and 88 % with a likelihood ratio of 7.71 in patients with a combined elevated CRP level and WBC count and RLQ pain. With regard to the approxi-mately equal numbers of positive and negative CTs in patients with normal CRP levels, the authors considered that a nega-tive CRP level does not rule out posinega-tive findings on CT. In our study cohort, 10 (32.3 %) and 21 (67.7 %) patients in whom the CRP levels were within normal limits had positive and negative CTs, respectively. Thus, our results were in line with their study in terms of analysis of CRP levels; however, we may also assume that combined elevated CRP level and WBC count result in higher sensitivity and specificity with Table 2 Cohort characteristics
classified by CT diagnoses Characteristics,n (%) unless otherwise specified Negative CTs Positive CTs p value n = 41 n = 60
(40.6 %) (59.4 %) Demographics
Age (years), mean (SD) 37.7 (17.8) 46.2 (20.6) <0.05
Female gender 25 (61) 31 (51.7) 0.35 CRP level <0.05 <5 mg/L 21 (51.2) 10 (16.7) >5 mg/L 20 (48.8) 50 (83.3) WBC count 0.08 <10.20 × 103/μL 20 (48.8) 19 (31.7) >10.20 × 103/μL 21 (51.2) 41 (68.3)
Combined CRP level and WBC count <0.05
Both of them elevated 13 (31.7) 37 (61.7) One of them elevated 15 (36.6) 17 (28.3) None of them elevated 13 (31.7) 6 (10) CRP C-reactive protein, WBC white blood cell
Table 3 Range of positive and negative CT diagnoses by pain location
Pain location Negative CTs Positive CTs Total p value (chi-square)
n (%) n (%) n (%)
Right lower quadrant 14 (34.1 %) 23 (38.3 %) 37 (36.6 %) <0.05 Right upper quadrant 1 (2.4 %) 8 (13.3 %) 9 (8.9 %)
Left lower quadrant 2 (4.9 %) 10 (16.7 %) 12 (11.9 %) Left upper quadrant 2 (4.9 %) 1 (1.7 %) 3 (3 %)
Flank 0(0 %) 4 (6.7 %) 4 (4 %)
Epigastric 3(7.3 %) 4 (6.7 %) 7 (6.9 %)
Pelvic 7 (17.1 %) 1 (1.7 %) 8 (7.9 %)
increasing likelihood for determining a positive CT, particu-larly in patients with RLQ pain.
Another study assessed the value of CRP levels and WBC count in differentiating urgent conditions that require imme-diate imaging [7]. Combined elevated CRP level (>10 mg/L) and WBC count (>10 × 109/L) yielded a sensitivity and spec-ificity of 58.0 and 76.7 %, respectively. Although pain local-ization and imaging results were not considered in their study, CRP level and WBC count were declared as insufficient markers in the selection of patients for diagnostic imaging, given the low sensitivity and specificity of these markers to rule out an urgent condition. The authors also stated that CRP level (>50 mg/L) combined with WBC count (>15 × 109/L) achieves the highest positive predictive value (PPV) (85.5 %), and imaging is justified in these patients. However, they did not state the imaging modality, as well as the imaging results, in contrast to our study where CT results were considered. Additionally, according to our study results, higher PPVs (86 and 92 %) are achieved only when elevated CRP level or combined elevated CRP level and WBC count are consid-ered in patients with RLQ pain.
In order to include a clinical predictor, we examined the value of pain location in making a decision to perform CT in patients with NTAA. To our knowledge, this study is the first to assess whether pain location aids in the selection of patients for CT imaging in the clinical setting of NTAA. Right lower and LLQ pain yielded the highest number of positive CTs. Numbers of positive CTs in patients with flank pain and in patients with RUQ pain were also high; however, their pro-portions in the study cohort were small. Of the four patients presenting with flank pain, all had positive CTs with findings of pyelonephritis in one, ureteral stone in two, and intracalyceal stone with dilatation in one. All of these patients were male, and the youngest of them was 31 years old.
Presently, unenhanced CT is commonly used in the evaluation of patients with suspected renal colic with reported high ac-curacy. However, emphasis on the deterministic effects of ra-diation exposure in children and young adults and efforts to reduce medical radiation in this particular group have been well established [2,16]. To avoid radiation exposure, in pa-tients with known urolithiasis and/or a presentation classic for renal colic, US may be preferred as a first-line modality, par-ticularly in children and young females. MRI also can be considered as an alternative to CT in certain conditions, such as pregnancy and young patient age. Nevertheless, relatively restricted availability and less accuracy in directly visualizing stones as compared to CT may be limiting factors in the utility of MRI in EDs [9,19].
In our study, pelvic pain resulted in the lowest number of positive CTs. Of the eight patients with pelvic pain, four had combined elevated CRP level and WBC count and only one patient had positive CT with a final diagnosis of pelvic inflam-matory disease. Additionally, of these patients with pelvic pain, five were women with a mean age of 36 and the youn-gest one was 26 years old. According to the present study results, it may be assumed that CT provides the lowest benefit in patients with pelvic pain in the clinical setting of NTAA.
Our study has several limitations. The study design was single center and retrospective. We did not evaluate whether the patients had US examination prior to CT and the results of US examinations. However, considering that pelvic pain yielded the lowest number of positive CTs in our study cohort, it may be assumed that US may be preferred as a first-line modality, particularly in young females presenting with pelvic pain. Another remarkable point is that although CTs were positive in most of the patients with RUQ pain, we believe that they had diagnoses that may have theoretically been di-agnosed by US. We did not consider any clinical data obtained Table 4 CRP levels in positive
and negative CT groups regarding pain locations
Pain location CRP level Negative CTs Positive CTs Total p value
n (%) n (%) n (%)
Right lower quadrant Normal 11 (78.6 %) 3 (13 %) 14 (37.8 %) <0.05 Elevated 3 (21.4 %) 20 (87 %) 23 (62.2 %)
Right upper quadrant Normal 0 (0 %) 1 (12.5 %) 1 (11.1 %) = 0.708 Elevated 1 (100 %) 7 (87.5 %) 8 (88.9 %)
Left lower quadrant Normal 0 (0 %) 2 (20 %) 2 (16.7 %) = 0.488 Elevated 2 (100 %) 8 (80 %) 10 (83.3 %)
Left upper quadrant Normal 1 (50 %) 0 (0 %) 1 (33.3 %) = 0.386 Elevated 1 (50 %) 1 (100 %) 2 (66.7 %)
Epigastric Normal 1 (33.3 %) 0 (0 %) 1 (14.3 %) = 0.212 Elevated 2 (66.7 %) 4 (100 %) 6 (85.7 %)
Pelvic Normal 3 (42.9 %) 0 (0 %) 3 (37.5 %) = 0.408 Elevated 4 (57.1 %) 1 (100 %) 5 (62.5 %)
Diffuse abdominal Normal 5 (41.7 %) 1 (11.1 %) 6 (28.6 %) = 0.125 Elevated 7 (58.3 %) 8 (88.9 %) 15 (71.4 %)
by an ED physician except for pain location. Other clinical data such as fever, patient complaints other than pain, and physical examination findings to necessitate an abdominal CT were not analyzed. Absolute levels of CRP and WBC counts may have been confounded by other acute inflamma-tory and infectious diseases, chronic conditions such as rheu-matoid arthritis and systemic lupus erythematosus, and certain medications such as non-steroidal anti-inflammatory drugs. No significant difference was found between positive and negative CT groups in terms of CRP levels in patients with pain locations other than RLQ. However, considering the high number of positive CTs in patients with LLQ pain, flank pain, and RUQ pain, we may assume that a significant difference may be found with larger proportions of these groups. Our results in this retrospective study may serve as a starting point for conducting a prospective study involving a larger patient cohort where clinical and laboratory variables could be con-trolled in order to draw useful conclusions.
In conclusion, CRP levels and WBC counts combined with pain location may serve as a guide for the selection of patients for CT imaging in the clinical setting of NTAA. Abdominal CT seems to be clinically justified in patients with RLQ pain and combined elevated CRP level and WBC count, for whom CT imaging would be most beneficial.
Compliance with ethical standards This retrospective study was ap-proved by our institutional review board.
Conflict of interest The authors declare that they have no conflict of interest.
Disclosure No financial disclosures or conflict of interest on behalf of the authors. There was no commercial funding for this study.
References
1. Boone JM, Brunberg JA (2008) Computed tomography use in a tertiary care university hospital. J Am Coll Radiol 5:132–138. doi:10.1016/j.jacr.2007.07.008
2. Brenner DJ, Hall EJ (2012) Cancer risks from CT scans: now we have data, what next? Radiology 265:330–331. doi:10.1148/radiol.12121248
3. Chang JC, Lin YY, Hsu TF, Chen YC, How CK, Huang MS (2016) Trends in computed tomography utilisation in the emer-gency department: a 5 year experience in an urban medical Centre in northern Taiwan. Emerg Med Australas 28:153–158. doi:10.1111/1742-6723.12557
4. Coyle JP, Brennan CR, Parfrey SF, et al. (2012) Is serum C-reactive protein a reliable predictor of abdomino-pelvic CT findings in the clinical setting of the non-traumatic acute abdomen? Emerg Radiol 19:455–462. doi:10.1007/s10140-012-1041-4
5. Gans SL, Atema JJ, Stoker J, Toorenvliet BR, Laurell H, Boermeester MA (2015) C-reactive protein and white blood cell count as triage test between urgent and nonurgent conditions in 2961 patients with acute abdominal pain. Medicine (Baltimore) 94:e569. doi:10.1097/MD.0000000000000569
6. Hastings RS, Powers RD (2011) Abdominal pain in the ED: a 35 year retrospective. Am J Emerg Med 29:711–716. doi:10.1016/j.ajem.2010.01.045
7. Hyams ES, Korley FK, Pham JC, Matlaga BR (2011) Trends in imaging use during the emergency department evaluation of flank pain. J Urol 186:2270–2274
8. ICRP Publication 105 (2007) Radiation protection in medicine. Ann ICRP 37:1–63. doi:10.1016/j.icrp.2008.08.001
9. Kalb B, Sharma P, Salman K, Ogan K, Pattaras JG, Martin DR (2010) Acute abdominal pain: is there a potential role for MRI in the setting of the emergency department in a patient with renal calculi? J Magn Reson Imaging 32:1012–1023
10. Kocher KE, Meurer WJ, Fazel R, Scott PA, Krumholz HM, Nallamothu BK (2011) National trends in use of computed tomog-raphy in the emergency department. Ann Emerg Med 58:452– 462.e3. doi:10.1016/j.annemergmed.2011.05.020
11. Larson DB, Johnson LW, Schnell BM, Salisbury SR, Forman HP (2011) National trends in CT use in the emergency department: 1995-2007. Radiology 258:164–173. doi:10.1148/radiol.10100640
12. Mettler FA Jr, Bhargavan M, Faulkner K, et al. (2009) Radiologic and nuclear medicine studies in the United States and worldwide: frequency, radiation dose, and comparison with other radiation sources—1950-2007. Radiology 253:520–531. doi:10.1148/radiol.2532082010
13. Navarro Fernández JA, Tárraga López PJ, Rodríguez Montes JA, López Cara MA (2009) Validity of tests performed to diagnose acute abdominal pain in patients admitted at an emergency depart-ment. Rev Esp Enferm Dig 101:610–618
14. Oikarinen H, Meriläinen S, Pääkkö E, Karttunen A, Nieminen MT, Tervonen O (2009) Unjustified CT examinations in young patients. Eur Radiol 19:1161–1165. doi:10.1007/s00330-008-1256-7
15. Pearce MS, Salotti JA, McHugh K, et al. (2011) CT scans in young people in northern England: trends and patterns 1993-2002. Pediatr Radiol 41:832–838
16. Pearce MS, Salotti JA, Little MP, et al. (2012) Radiation expo-sure from CT scans in childhood and subsequent risk of leukae-mia and brain tumours: a retrospective cohort study. Lancet 380: 499–505
17. Rosen MP, Siewert B, Sands DZ, Bromberg R, Edlow J, Raptopoulos V (2003) Value of abdominal CT in the emer-gency department for patients with abdominal pain. Eur Radiol 13:418–424
18. Scanff P, Donadieu J, Pirard P, Aubert B (2008) Population expo-sure to ionizing radiation from medical examinations in France. Br J Radiol 81:204–213. doi:10.1259/bjr/24344062
19. Semins MJ, Feng Z, Trock B, Bohlman M, Hosek W, Matlaga BR (2013) Evaluation of acute renal colic: a comparison of non-contrast CT versus 3-T non-contrast HASTE MR urography. Urolithiasis 41:43–46
20. Strömberg C, Johansson G, Adolfsson A (2007) Acute abdominal pain: diagnostic impact of immediate CT scanning. World J Surg 31:2347–2354
21. Wong K, Shahab Y, Gill PG (2012) Diagnostic value of an initial C-reactive protein level in acute surgical patients. ANZ J Surg 82:52–55