Clin Respir J. 2020;14:47–53. wileyonlinelibrary.com/journal/crj © 2019 John Wiley & Sons Ltd
|
47 O R I G I N A L A R T I C L EBone mineral density in emphysema and chronic bronchitis
phenotypes in hospitalized male chronic obstructive pulmonary
disease patients
Burcu Yormaz
1|
Hakan Cebeci
2|
Farise Yılmaz
3|
Mecit Süerdem
11Department of Pulmonology, Selcuk University Faculty of Medicine, Konya, Turkey
2Department of Radiology, Selcuk University Faculty of Medicine, Konya, Turkey
3Department of Nuclear Medicine, Selcuk University Faculty of Medicine, Konya, Turkey
Correspondence
Burcu Yormaz, Department of
Pulmonology, Selcuk University Faculty of Medicine, Selcuklu, Konya 42250, Turkey. Email: [email protected]
Abstract
Introduction: Risk of osteoporosis known to increase in chronic obstructive
pulmo-nary disease (COPD), but is usually overlooked, especially in male patients.
Objectives: The present study compares the bone mineral density (BMD)
measure-ments of male COPD patients with emphysema and the chronic bronchitis pheno-type, and evaluates the association between density of emphysema and osteoporosis.
Methods: Ninety‐four patients with COPD, and with emphysema and the chronic
bron-chitis phenotype, were included in the prospective study. A high‐resolution computed tomography (HRCT) was used for the diagnosis of emphysema, and a dual X‐ray absorp-tiometry was used to measure the BMD of the lumbar vertebrae and neck of the femur.
Results: Emphysema phenotype 45.75% and chronic bronchitis phenotype 54.25%,
based on their clinical findings and a quantitative volumetric analysis by HRCT. Osteoporosis was found 60.47% and 17.65% of patients with emphysema and bron-chitis, while osteopenia was detected 27.91% and 41.18% of patients with emphy-sema and bronchitis, respectively. A negative correlation was found between HRCT emphysema density and the bone densitometer t‐score in patients with osteoporo-sis. Among the patients with osteoporosis, a positive correlation was found between Body Mass Index (BMI) and the bone densitometer t‐score. Only BMI and emphy-sema score were found to be independent risk factors for a low BMD. One unit drop in BMI increased the risk of osteoporosis by 28% (OR = 1.28, 95% CI 1.14‐1.45) (P < 0.001). One unit increase in emphysema score increased the risk of osteoporosis by 6% (OR = 1.06, 95% CI 1.03‐1.09) (P < 0.001).
Conclusion: Especially male patients with emphysema, high dyspnea score, low
BMI and frequent exacerbations should be evaluated for osteoporosis.
K E Y W O R D S
bone densitometer, COPD, emphysema, osteoporosis
1
|
INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is recog-nized as a complex heterogeneous syndrome, having both pulmonary and extrapulmonary features.1 The systemic
consequences of COPD contribute significantly to a decrease in quality of life.2 COPD has different phenotypes, with dif-ferent clinical, radiological and prognostic features,3 with two of the best known phenotypes among the many validated or invalidated phenotypes of the disease being emphysema
and chronic bronchitis.4 The correct determination of the phenotype is important for predicting prognosis and ensuring the best therapy.5
COPD is a disease with many comorbidities, 6 among which osteoporosis is one of the best known. Several studies have shown a high prevalence of osteoporosis and low bone mineral density (BMD) in patients with COPD.7,8 There are still several unanswered questions about the prevalence of osteoporosis and osteopenia in COPD patients varies be-tween 9%‐69% and 27%‐67%, respectively.9 COPD patients have several risk factors for osteoporosis, including hypo-gonadism and poor mobility because of ageing, smoking, poor nutrition, systemic inflammation, low BMI and high doses of inhaled corticosteroids, as well as courses of sys-temic steroids. 10 Various epidemiological studies have been demonstrated the association between airway limitation and osteoporosis, 9,11-13 while other studies have reported that emphysema is the strongest predictor of low BMD in pa-tients with airflow obstruction.14,15 There are still several unanswered questions about the association of decreased mineral bone density, airway disease and emphysema. 15,16
Osteoporosis is a subclinical disease and it is often eval-uated in postmenopausal women. Although osteoporosis is a serious comorbidity in patients with COPD, the evaluation of BMD is generally overlooked in male patients with COPD. The present study compared the BMD measurements of male COPD patients, with emphysema and the chronic bronchitis phenotype, who were hospitalized because of exacerbation. To the best of our knowledge, no study to date has evaluated the difference in BMD in the two phenotypes of COPD. We also determined any independent predictors of decreased BMD.
2
|
MATERIALS AND METHODS
Patients with COPD with emphysema and the bronchitis phe-notype aged 40 years or older, and who were hospitalized because of exacerbation of COPD in the Pulmonary Diseases Clinic of the School of Medicine of University of Selcuk between October 2017 and April 2018, were prospectively included in the study.
In the patient selection, inclusion criteria: all patients were having a definitive diagnosis of COPD through ap-propriate spirometric measurements (post‐bronchodilator FEV1/FVC <0.70), a previous medical history of at least 20 packs of cigarettes/year smoked and being under regular inhaler treatment for more than a year. Exclusion criteria: Patients who have a history of asthma or any chronic pul-monary disorders other than COPD, diseases of the thy-roid and parathythy-roid glands, malignancy, history of bone disease, treatment for osteoporosis or the administration of diuretics were excluded. The patients’ history of cigarette smoking, body mass index (BMI), number of exacerbations
in the past year, arterial blood gases and levels of alpha‐1 antitrypsin (A1AT), parathormone (PTH), calcium (Ca), phosphorus (P), vitamin D and alkaline phosphatase (ALP) levels were recorded. The severity of dyspnea was graded according to the mMRC Dyspnea Scale in the stable period before exacerbation. The BMI was calculated by dividing weight (in kilograms) by the square of the height.
Chronic bronchitis was defined as cough and sputum produc-tion occurring on most days of the month for at least 3 months per year for 2 years prior to the study.1 The emphysema pheno-type of COPD was determined through a density measurement on high‐resolution computed tomography (HRCT). All CT examinations were performed using a 128 multi‐detector CT scanner (Siemens Healthcare, Erlangen, Germany) at a radia-tion exposure of 100 mA. A single chest radiologist evaluated and processed the HRCT images. Images were reconstructed and lung and emphysema volumes were measured through a quantitative volumetric analysis on previously acquired HRCT chest images using the Siemens Syngo‐Via CT Workspace. Percent emphysema was defined as number of lung voxels below −920 HU (Hounsfield Unit), and a level higher than 15% was accepted as a cut off value for discriminating between the emphysema and non‐emphysema groups.17
Bone mineral density was measured at the lumbar spine (L1‐L4) and femoral necks through a dual energy X‐ray ab-sorptiometry (DEXA) (Hologic QDR 2000, Bedford, MA, USA). Osteoporosis was defined as t‐score below −2.5 and osteopenia was defined as t‐score between −1.0 and −2.5, in accordance with the World Health Organization definition.18 Subjects with a t‐score greater than −1 were considered nor-mal. Patients with abnormal t‐score were referred to the en-docrinology clinic.
The normality of the data obtained by the measurements of patient parameters was tested with an Anderson Darling nor-mality test. A One‐Way ANOVA and a student's t test were used for the analysis of the continuous variables with normal distribution, while Kruskal‐Wallis and Mann‐Whitney U tests were used for the analysis of non‐normally distributed vari-ables. In addition, Pearson and Spearman's Rho correlation coefficients were used for the evaluation of associations of the measured parameters. Pair‐wise comparisons of the parame-ters that were found to be significant in the One‐Way ANOVA and the Kruskal‐Wallis tests were performed using a Tukey HSD and Conover‐Iman binary comparison with a Bonferroni correction, respectively. A multiple linear regression analy-sis was used to identify the following independent variables related to BMD: age, BMI, smoking (pack/years), emphy-sema score, biofuel exposure (years), vitamin D and mMRC. Logistic regression analysis was used to evaluate the relation-ship between BMI, emphysema score and osteoporosis.
The general statistical significance and Bonferroni cor-rection levels were set at P < 0.05 and P < 0.016, respec-tively. However, a Chi‐square test was used for the analysis of
categorical variables. Visual presentations of statistical anal-yses were prepared using Box Plot and Scatter Plot, with the obtained P values given in the graphics.
3
|
RESULTS
A total of 94 patients were included in the study. Based on BMD measurements, 35 (37.23%) patients were found to have osteoporosis and 33 (35.10%) were diagnosed to have osteopenia. Bone densitometry was evaluated as normal in 26 (27.65%) patients. A total of 43 patients (45.75%) were as-signed to the emphysematous phenotype group based on an HRCT density measurement, and 51 patients (54.25%) were assigned to the chronic bronchitis phenotype group based on clinical findings. The rates of osteoporosis and osteope-nia according to the phenotypes are presented in Table 1. Osteoporosis was found in 26 (60.47%) and 9 (17.65%) of the patients with the emphysematous and chronic bronchitis phe-notypes, respectively (P < 0.001). Osteopenia was found in 12 (27.91%) and 21 (41.18%) patients among the patients with emphysema and chronic bronchitis, respectively (P < 0.001).
The findings of a comparison of the various parameters in groups with osteoporosis, osteopenia and normal BMD
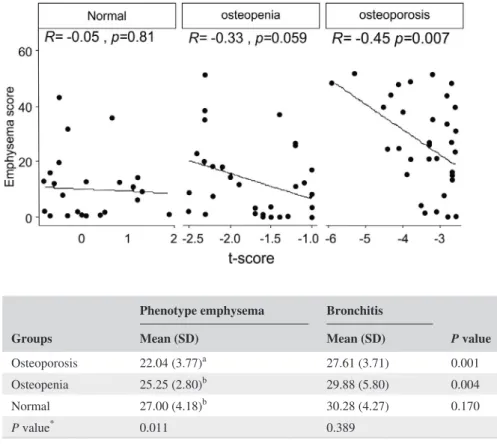
are presented in Table 2. BMI was significantly lower in the group with osteoporosis (P = 0.001). The number of exacerbations over the past year and mMRC dyspnea score were significantly higher in patients with osteoporosis (P = 0.009 and P = 0.005, respectively). No statistically significant difference was found in the mean age, rate of cigarette smoking (pack/year) and levels of Ca, P, PTH, ALP, vitamin D and A1AT. No statistically significant dif-ference was found in the bone densitometer t‐score values between the emphysema and chronic bronchitis phenotypes among the groups with osteoporosis, osteopenia and nor-mal bone densitometer (Table 3). A negative correlation was found between the emphysema score and bone densi-tometer t‐score in patients with osteoporosis (r = −0.45, P = 0.007) (Figure 1).
Among the groups with osteoporosis and osteopenia, the mean BMI values of the patients with emphysema were significantly lower than those patients with chronic bron-chitis (P = 0.001, P = 0.004, respectively) (Table 4). BMI was significantly different in the groups with osteoporosis, osteopenia and normal bone density (P = 0.011), while no significant difference was found in the chronic bronchitis phe-notype COPD (P = 0.389) (Table 4) (Figure 2). Among all
Phenotype Total P value Emphysema Bronchitis Osteoporosis (n, %) 26aA (74.29%) 9bA (25.71%) 35 (100%) <0.001 Osteopenia (n, %) 12 (36.36%) 21B (63.64%) 33 (100%) Normal (n, %) 5aB (19.23%) 21bB (80.77%) 26 (100%) Note: Small letters (a, b) in rows show that statistically significant for rows.
Capital letters (A, B) in column show that statistically significant for columns.
P value: Statistically significant value for Chi‐square test, Fisher's Exact test was performed to multiple
com-parison for rows and columns.
TABLE 1 Osteoporosis and osteopenia distribution by phenotypes
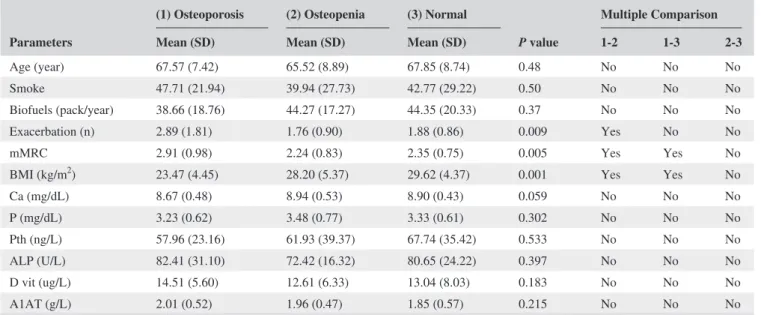
TABLE 2 Comparison of parameters according to groups
Parameters
(1) Osteoporosis (2) Osteopenia (3) Normal
P value
Multiple Comparison Mean (SD) Mean (SD) Mean (SD) 1‐2 1‐3 2‐3
Age (year) 67.57 (7.42) 65.52 (8.89) 67.85 (8.74) 0.48 No No No
Smoke 47.71 (21.94) 39.94 (27.73) 42.77 (29.22) 0.50 No No No
Biofuels (pack/year) 38.66 (18.76) 44.27 (17.27) 44.35 (20.33) 0.37 No No No
Exacerbation (n) 2.89 (1.81) 1.76 (0.90) 1.88 (0.86) 0.009 Yes No No
mMRC 2.91 (0.98) 2.24 (0.83) 2.35 (0.75) 0.005 Yes Yes No
BMI (kg/m2) 23.47 (4.45) 28.20 (5.37) 29.62 (4.37) 0.001 Yes Yes No
Ca (mg/dL) 8.67 (0.48) 8.94 (0.53) 8.90 (0.43) 0.059 No No No P (mg/dL) 3.23 (0.62) 3.48 (0.77) 3.33 (0.61) 0.302 No No No Pth (ng/L) 57.96 (23.16) 61.93 (39.37) 67.74 (35.42) 0.533 No No No ALP (U/L) 82.41 (31.10) 72.42 (16.32) 80.65 (24.22) 0.397 No No No D vit (ug/L) 14.51 (5.60) 12.61 (6.33) 13.04 (8.03) 0.183 No No No A1AT (g/L) 2.01 (0.52) 1.96 (0.47) 1.85 (0.57) 0.215 No No No
Groups
Phenotype emphysema Bronchitis
P value
Total Mean (SD) Mean (SD) Mean (SD)
Osteoporosis −3.48 (0.89) −3.08 (0.44) 0.426 −3.38 (0.81) Osteopenia −1.92 (0.54) −1.62 (0.47) 0.164 −1.73 (0.51) Normal −0.27 (0.53) 0.17 (0.81) 0.361 0.09 (0.78)
Total −2.67 (1.35) −1.14 (1.37) −1.84 (1.56)
TABLE 3 Comparison of t‐score values in emphysema and bronchitis phenotypes
FIGURE 1 The correlation between emphysema score and t‐score
Groups
Phenotype emphysema Bronchitis
P value Mean (SD) Mean (SD) Osteoporosis 22.04 (3.77)a 27.61 (3.71) 0.001 Osteopenia 25.25 (2.80)b 29.88 (5.80) 0.004 Normal 27.00 (4.18)b 30.28 (4.27) 0.170 P value* 0.011 0.389 *Kruskal‐Wallis test.
a, b Diverse icons demonstrate statistically significant difference. Groups which have same icons are related with similar outcomes
TABLE 4 Comparison of BMI values of normal, osteopenia and osteoporosis groups in phenotypes
FIGURE 2 The level of BMI in emphysema and bronchitis phenotypes
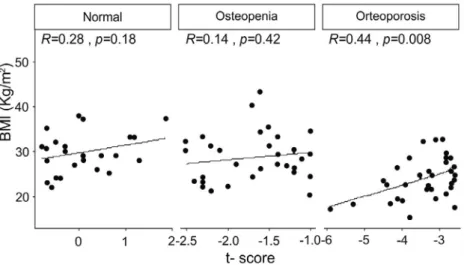
of the patients with osteoporosis, a positive correlation was found between BMI and the bone densitometer t‐score value (r = 0.44, P = 0.008) (Figure 3). A multiple linear regression analysis found that only BMI and the emphysema score were the independent risk factors for low BMD (Table 5).
All patients underwent osteoporosis risk calculations for BMI and emphysema scores without any differentia-tion of emphysema and chronic bronchitis phenotypes. One unit drop in BMI increased the risk of osteoporosis by 28% (OR = 1.28, 95% CI 1.14‐1.45) (P < 0.001). One unit in-crease in emphysema score inin-creased the risk of osteoporosis by 6% (OR = 1.06, 95% CI 1.03‐1.09) (P < 0.001). The risk of developing osteoporosis was 8.33 times higher in patients with emphysema score ≥15% when compared to those with <15% (OR = 8.33, 95% CI 3.16‐21.98) (P < 0.001).
4
|
DISCUSSION
We found a decrease BMD in 72.33% of exacerbated COPD patients who were hospitalized. We also determined osteo-porosis in 37.23% of these patients. Osteoosteo-porosis was found
to be three times more frequent in the emphysema pheno-type than in the chronic bronchitis phenopheno-type (60.47% vs 17.65%, respectively). There was a significant negative correlation between radiological emphysema density and t‐ score of BMD. A multiple linear regression analysis showed that only BMI and emphysema score were independent risk factors for a low BMD. The risk of osteoporosis increased 28% for each unit drop in BMI, and 6% for each unit in-crease in emphysema score. The risk of developing osteo-porosis was 8.33 times higher in patients with emphysema score ≥15% when compared to those with <15%.
Osteoporosis and osteopenia were reported in 36%‐60% and 35%‐72%, respectively, in patients with COPD in a re-view.8 A meta‐analysis of 13 studies including a total of 775 patients with COPD revealed that the prevalence of osteopo-rosis and osteopenia in COPD patients varied from 9%‐69% and from 27%‐67%, respectively.19 The mean rate of oste-oporosis was reported to be 35% in a study. The TORCH (TOwards a Revolution in COPD Health) study of 658 COPD patients revealed the presence of osteoporosis and osteopenia in 23% and 43% of the patients, respectively, at the hip or the lumbar spine on DEXA scan.12 Osteoporosis and osteopenia were observed in 30% and 50% of COPD patients among the Egyptian population.20 Osteoporosis and osteopenia were detected in 68 (66.6%) and 20 (19.6%) of 102 patients with COPD in a study, in which the frequency of osteoporosis was evaluated in COPD among the Indian population.21 The major reasons for the discrepancies in the prevalence of oste-oporosis among the studies may be attributed to the varying sociocultural structures of the patient populations and the dif-ferent diagnostic methods used.
Different studies have reported emphysema to be an in-dependent risk factor for osteoporosis, based on the ‘holes in the lungs, holes in the bones’ theory.16 It has been sug-gested in a study detailing the systemic effects of COPD that oxidative stress, inflammatory cells and proinflamma-tory cytokines, all of which are involved in the pathogenesis FIGURE 3 The correlation between
BMI and t‐score
TABLE 5 Multiple linear regression analysis for bone mass density Variable β t P 95% CI for β Age −0.051 −0.533 0.595 −0.240 to 0.139 BMI 0.324 2.653 0.010* 0.081 to 0.567 Smoke −0.021 −0.236 0.814 −0.198 to 0.156 Biofuel 0.128 1.358 0.178 −0.059 to 0.316 Vitamin D −0.061 −0.651 0.517 −0.248 to 0.126 mMRC −0.107 −1.143 0.256 −0.292 to 0.079 Emphysema score (pe) −0.298 −2.355 0.021 * −0.550 to −0.046
Abbreviations: BMI, body mass index; CI, confidence interval. *P < 0.05 was considered statistically significant.
of COPD and cause damage, might cause injury to both lung parenchyma and bone tissue.22 Bon et al found that the degree of emphysema in COPD patients is the most important factor for osteoporosis, independent of other pre-dictors such as age, gender, tobacco smoking and BMI.15 However, only the visual emphysema score was used in that study. In a study investigating the prevalence of osteo-porosis and the parameters associated with osteoosteo-porosis in the emphysema phenotype, only reduced BMI, FEV1 and PaO2 levels were found to be independent risk factors for low BMD.23 Emphysema score was not found to be a risk factor for low BMD in the present study, although a mul-tiple regression analysis rather than a multivariate analysis statistical method should have been used.
One important result of this present study was the finding of a significantly low BMI among patients with osteoporosis and determination of a significant negative correlation between BMD and BMI. Osteoporosis in COPD was found to be correlated with a decrease in BMI and lean BMI.24-26 Graat‐Verboom et al reported an osteoporosis and osteopenia frequency of 21% and 41%, respectively, among 554 patients with COPD, concluding that cachexia was an independent risk factor for osteoporosis, and obe-sity and excess weight as preventive factors.9 They further demonstrated that the lean BMI, as a measure of muscle wasting, decreased as the level of emphysema increased in participants with COPD.27
Osteoporosis and osteopenia were detected in 40 patients each, in a study with the same number of patients as the pres-ent study,28 and the authors found a significant positive cor-relation between femoral neck t‐score and lumber t‐score and FEV1 and FVC levels. Similarly, in another study, a signif-icant decrease was noted in BMD with a decrease in FEV1 in patients with COPD.13 In contrast, no association was found in an age‐ and gender‐matched study between FEV1 and BMD.12 No comparison of the spirometry results was made in the present study, given the inclusion of patients with COPD with exacerbation.
This cross‐sectional study has some limitations, being performed in a single centre. In addition, data on previ-ous corticosteroid treatment, exposure to sunlight, phys-ical activity and nutrition habits were unavailable in the medical histories of the patients. The results of this study demonstrate that osteoporosis risk is associated with the t‐score in the male emphysema phenotype, in spite of these limitations.
In conclusion, we identified a high prevalence of osteo-porosis and osteopenia in hospitalized male COPD patients, with the frequency of osteoporosis being found to be signifi-cantly high in the emphysema phenotype when compared to the bronchitis phenotype. BMI was found to be signifi-cantly low and the number of exacerbations and mMRC score were significantly high in patients with osteoporosis.
In addition, significant correlations were found between BMD and emphysema score, and BMI. Only BMI and em-physema score were found to be independent risk factors for low BMD. In conclusion, routine BMD measurements should be made especially in emphysema phenotype COPD patients with a high dyspnea score, low BMI and frequent exacerbations.
ACKNOWLEDGMENTS
Thanks to the Assistant Prof. Neriman Akdam (Department of Biostatistics, Faculty of Medicine, Selcuk University) and M. Kazım Korez (Department of Statistics, Faculty of Science, Selcuk University) excavation for their statistical evaluation.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest with the contents of the article.
AUTHOR CONTRIBUTIONS
MS designed the experiments. BY and MS performed experi-ments. HC interpreted thorax tomography. FY commented on bone densitometry results. BY drafted the manuscript. The final version of the manuscript has been read and approved by all authors, and each author believes that the manuscript represents honest work.
ETHICS
The study protocol was approved by the Ethics Committee of the Selcuk University Medical School as a prospective descriptive study, and all subjects gave written informed consent
ORCID
Burcu Yormaz https://orcid.org/0000-0001-6563-8337
REFERENCES
1. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir
Crit Care Med. 2017;195:557‐582.
2. Decramer M, Rennard S, Troosters T, et al. COPD as a lung disease with systemic consequences–clinical impact, mechanisms, and po-tential for early intervention. COPD. 2008;5:235‐256.
3. Han MK, Agusti A, Calverley PM, et al. Chronic obstructive pul-monary disease phenotypes: the future of COPD. Am J Respir Crit
4. Vestbo J, Agusti A, Wouters EF, et al. Should we view chronic obstructive pulmonary disease differently after ECLIPSE?. A clin-ical perspective from the study team. Am J Respir Crit Care Med. 2014;189:1022‐1030.
5. Miravitlles M, Calle M, Soler‐Cataluna JJ. Clinical phenotypes of COPD: identification, definition and implications for guidelines.
Arch Bronconeumol (Eng Ed). 2012;48:86‐98.
6. Barnes P, Celli B. Systemic manifestations and comorbidities of COPD. Eur Respir J. 2009;33:1165‐1185.
7. Jørgensen NR, Schwarz P. Osteoporosis in chronic obstructive pulmonary disease patients. Curr Opin Pulm Med. 2008;14: 122‐127.
8. Biskobing DM. COPD and osteoporosis. Chest. 2002;121:609‐620. 9. Graat‐Verboom L, Wouters E, Smeenk F, Van Den Borne B, Lunde
R, Spruit M. Current status of research on osteoporosis in COPD: a systematic review. Eur Respir J. 2009;34:209‐218.
10. Ionescu A, Schoon E. Osteoporosis in chronic obstructive pulmo-nary disease. Eur Respir J. 2003;22:64‐75.
11. Sin DD, Man JP, Man SP. The risk of osteoporosis in Caucasian men and women with obstructive airways disease. Am J Med. 2003;114:10‐14.
12. Ferguson GT, Calverley PM, Anderson JA, et al. Prevalence and progression of osteoporosis in patients with COPD: results from the TOwards a Revolution in COPD Health study. Chest. 2009;136:1456‐1465.
13. De Vries F, Van Staa T, Bracke M, Cooper C, Leufkens H, Lammers JJ. Severity of obstructive airway disease and risk of osteoporotic fracture. Eur Respir J. 2005;25:879‐884.
14. Ohara T, Hirai T, Muro S, et al. Relationship between pulmonary emphysema and osteoporosis assessed by CT in patients with COPD. Chest. 2008;134:1244‐1249.
15. Bon J, Fuhrman CR, Weissfeld JL, et al. Radiographic emphysema predicts low bone mineral density in a tobacco‐exposed cohort. Am
J Respir Crit Care Med. 2011;183:885‐890.
16. Cooper CB. Do holes in the lungs beget holes in the bones? Am J
Respir Crit Care Med. 2011;183:835‐837.
17. Hersh CP, Jacobson FL, Gill R, Silverman EK. Computed tomog-raphy phenotypes in severe, early‐onset chronic obstructive pulmo-nary disease. COPD. 2007;4:331‐337.
18. Maślińska M. World Congress on Osteoporosis, Osteoarthritis and Musculoskeletal Diseases–the “Wco‐iof‐esceo Congress”: The
18th edition of the WCO‐IOF‐ESCEO Congress‐Krakow 2018.
Reumatologia. 2018;56:199.
19. Graat‐Verboom L, Spruit MA, van den Borne BE, et al. Correlates of osteoporosis in chronic obstructive pulmonary disease: an under-estimated systemic component. Respir Med. 2009;103:1143‐1151. 20. Abbasi M, Zohal M, Atapour B, Yazdi Z. Prevalence of osteoporo-sis and its risk factors in men with COPD in Qazvin. Int J Chronic
Dis. 2016;2016:1–6.
21. Hattiholi J, Gaude GS. Prevalence and correlates of osteoporosis in chronic obstructive pulmonary disease patients in India. Lung
India. 2014;31:221–225.
22. Agusti A, Noguera A, Sauleda J, Sala E, Pons J, Busquets X. Systemic effects of chronic obstructive pulmonary disease. Eur
Respir J. 2003;21:347‐360.
23. Fouda A‐M, Youssef AR. Antiosteoporotic activity of Salvadora persica sticks extract in an estrogen deficient model of osteoporo-sis. Osteoporos Sarcopenia. 2017;3:132‐137.
24. Smith MC, Wrobel JP. Epidemiology and clinical impact of major comorbidities in patients with COPD. Int J Chron Obstruct Pulmon
Dis. 2014;9:871–874.
25. Hillas G, Perlikos F, Tsiligianni I, Tzanakis N. Managing comorbid-ities in COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:95–99. 26. Dursunoğlu N, Köktürk N, Baha A, et al. Comorbidities and their
impact on chronic obstructive pulmonary disease. Tuberk Toraks. 2016;64:289‐298.
27. Rutten E, Grydeland TB, Pillai SG, et al. Quantitative CT: associa-tions between emphysema, airway wall thickness and body compo-sition in COPD. Pulm Med. 2011;2011:1‐6.
28. van Dort MJ, Geusens P, Driessen JH, et al. High imminent verte-bral fracture risk in subjects with COPD with a prevalent or inci-dent vertebral fracture. J Bone Miner Res. 2018;33:1233‐1241. How to cite this article: Yormaz B, Cebeci H,
Yılmaz F, Süerdem M. Bone mineral density in emphysema and chronic bronchitis phenotypes in hospitalized male chronic obstructive pulmonary disease patients. Clin Respir J. 2020;14:47–53.