Risk factors for chronic pelvic pain:
hospital-based case–control study
from Turkey
Sule Gokyildiz, Nezihe K Beji, Burcu Avcibay and Fatma T Ozgunen
ABSTRACTChronic pelvic pain (CPP) is a complicated condition that can have a large impact on life. The aetiology of CPP is often unclear and the origin appears to be multifactorial. This study aims to identify risk factors associated with CPP complaint in women. The study is a descriptive case–control study in nature. The study was conducted in one university and one state hospital. Women with CPP (n = 134) composed the case group while those who consulted to the polyclinics with other problems formed the control group (n = 383). The data were collected through a questionnaire which was prepared in light of the related literature and the ‘Pelvic Pain Assessment Form’ developed by the International Pelvic Pain Society. Women in the case and control groups were found to have similar socio-demographical features. This study has detected that CPP is associated with factors such as having a relative with recurrent pelvic pain complaint, having cancer or CPP history, having pain during menstruation, feeling of fullness in the abdominal region and stool consistency, recurrent urinary tract infections, having a diagnosed woman’s disease (ovarian cyst, genital tract infection, prolapsus and menstrual irregularity), having had an abdominal operation, taking vaginal showers after sexual intercourse or for any other reason, falling down from height or having an accident that caused back damage, experiencing a sad event during childhood, being exposed to physical violence or forced to sexual intercourse. In Conclusion, this study has found that reproduction, urinary, gastrointestinal, musculoskeletal systems and psychological factors affect women with chronic pelvic pain.
Key words: Chronic pelvic pain • Gastrointestinal system • Genito-urinary system • Musculoskeletal system • Psychological factors • Risk factors
BACKGROUND
Chronic pelvic pain (CPP) is defined as constant pain in the lower abdomen or pelvis of at least 6 months duration, not associated exclusively with men-struation or sexual intercourse (Kennedy and Moore, 2005).
Authors: S Gokyildiz, PhD, RN, Cukurova University, Adana Health High
School, Balcali Kampusu, Yuregir, Adana, Turkey; NK Beji, PhD, RN, Prof. Dr, Istanbul University, Florence Nightingale Faculty of Nursing, Department of Obstetrics and Gynecology Nursing, Abide-i Hurriyet cad. Sisli, Istanbul, Turkey; B Avcibay, MSc, Midwife, Cukurova University Adana Health High School, Balcali Kampusu, Yuregir, Adana, Turkey; FT Ozgunen, MD, Prof. Dr, Obstetrics and Gynecology Department, Cukurova University Faculty of Medicine, Balcali Kampusu, Yuregir, Adana, Turkey
Address for correspondence: S Gokyildiz, Cukurova University
Adana Health High School, Cukurova Universitesi Adana Saglik Yuksekokulu, Balcali Kampusu, 01330 Yuregir, Adana, Turkey E-mail: [email protected]; [email protected]
CPP prevalence in society-based studies ranges between 14⋅7% (Mathias et al., 1996) and 25⋅4% (Grace and Zondervan, 2004) and it is between 3⋅8% (Zondervan et al., 1999) and 26⋅6% (Muhammad et al., 2011) in women consulting to primary health care cen-tres. Studies show that CPP prevalence is high in women.
CPP is an enigmatic condition that can have a large impact on life. The aetiology of CPP is often unclear and the origin appears to be multifactorial (Gunter, 2003; Kroon and Reginald, 2005). Studies show that CPP is more common at the age of 30s (Mathias et al., 1996; Zondervan et al., 2001; Grace and Zon-dervan, 2004). The history of pelvic pain might be caused by factors such as peripartum pelvic pain syn-drome, delivering an overweight baby, muscle weak-ness and inadequate physical development, (hard) delivery, and delivery with the use of vacuum or for-ceps. Besides, it is common for women with CPP
to have experienced psychological changes, stress, sexual abuse, divorce, and family or violence prob-lems (Koyuncu, 2004; Latthe et al., 2006). Every struc-ture in the abdomen and/or pelvis plays a role in the aetiology of CPP. Evaluations should include reproduc-tion, urinary, gastrointestinal, musculoskeletal, periph-eral and central nervous systems (Gunter, 2003; Kroon and Reginald, 2005).
This study aims to identify the risk factors associated with CPP complaint in women.
MATERIALS AND METHODS Participants
This descriptive, case–control study was conducted in one university and one state hospital with the patients who consulted to Cukurova University Medical Faculty, Department of Obstetrics and Gynaecology and Adana Outpatient Polyclinics of Gynaecology and Obstetrics between the dates of June 2011 and April 2012. During these dates, the departments were visited twice a week (Wednesdays and Thursdays). The women visiting the departments were asked whether they had pain in pubic/lower abdominal or genital region within the past 6 months and/or more. Those who were found to have pain in the mentioned areas within the past 6 months and/or more (n = 134) were included in the case group and those who consulted to the departments because of other complaints (n = 383) formed the control group.
Data collection methods
The data were collected through a questionnaire which was prepared in light of the related literature and the ‘Pelvic Pain Assessment Form’ developed by the International Pelvic Pain Society. The question-naire included questions about socio-demographical features, reproduction, urinary, gastrointestinal and musculoskeletal systems, and psychiatric evaluations and habits. The questionnaire was administered to women while they were waiting for their clinic visit. The form was filled out by researchers during face-to-face interviews.
Ethical considerations
The written ethical approval was obtained from the ethical review board of Cukurova University. The par-ticipants were informed about the aims of the study and their verbal consent was obtained prior to the administration of the questionnaire. The participants were ensured that the information they gave would be kept confidential and that they could withdraw from the study any time if they wanted to do so.
Data analysis
The data obtained were calculated using SPSS (Sta-tistical Programme for Social Science) 13⋅5 for Windows and evaluated through frequency, mean, standard deviation, median, minimum and maximum, 𝜒2 test. Data with respect to CPP risk factors were
evaluated using Backward Stepwise Logistic Regres-sion Analysis. Odds ratios (ORs) and 95% confidence intervals (CIs) were obtained from unconditional mul-tiple logistic regression to evaluate the association between CPP and various risk factors. The partici-pants (n = 517) were divided into two groups as having and not having CPP. CPP was assessed in terms of its relationship with such factors as age, number of pregnancies and term labours, infant weight, urinary tract infection in the family, cancer or CPP history in the family, dysmenorrhea, woman disease, taking vaginal showers, having an operation, having an acci-dent, genital organ infection, bladder/urinary habits, bowel/defaecation habits and psychological factors. Statistical significance level was taken as p< 0⋅05 (Ozdamar, 2003).
RESULTS
This hospital-based study has revealed that 25⋅9% (n = 134) of the participants have CPP. Average age of the participants is 34⋅02 ± 10⋅5 in the case group, 75⋅4% (n = 101) are married, 38⋅8% (n = 52) grad-uated from primary school, 84⋅3% (n = 113) do not work, 42⋅5% (n = 57) have medium income, and 84⋅3% (n = 113) have nuclear families. As for the control group, the participants’ average age is 32⋅72 ± 10⋅82, 82% (n = 314) are married, 33⋅4% (n = 128) graduated from primary school, 83⋅8% (n = 321) do not work, 45⋅7% (n = 175) have medium income and 80⋅7% (n = 309) have nuclear families. No statistically signif-icant differences were found between the case and control groups in terms of their socio-demographical features (Table 1).
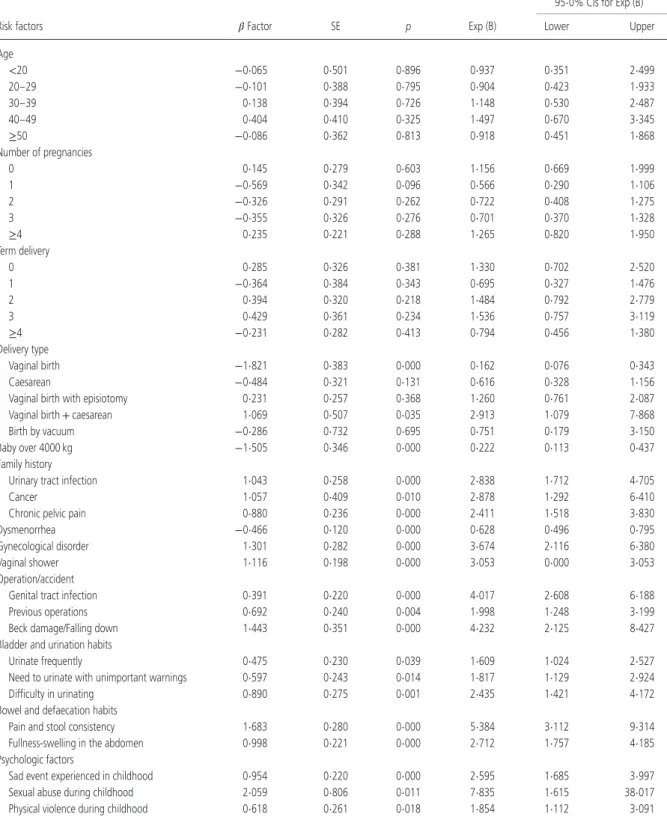
Findings regarding the distribution of risk factors associated with CPP are demonstrated in Table 2. The relationship between the participants’ obstetrics his-tory and CPP shows that delivery type and delivering a baby over 4000 kg was not found to be associated with CPP. However, the risk was found to increase 2⋅9 times more in those who experienced both vagi-nal and caesarean delivery. No statistically significant relationship was found between CPP and the number of pregnancies, but despite not being statistically sig-nificant, having two and three deliveries was found to create a partial risk factor for women.
An evaluation of the relationship of CPP with fibromyalgia, CPP, scleroderma, endometriosis,
Table 1 Socio-demographic characteristics of the participants CPP (n = 134) Control (n = 383) n % n % 𝜒2 p Age∗ <20 10 7⋅5 33 8⋅6 3⋅61 0⋅46 20–29 43 32⋅1 147 38⋅4 30–39 39 29⋅1 105 27⋅4 40–49 31 23⋅1 64 16⋅7 ≥50 11 8⋅2 34 8⋅9 Education Illiterate 21 15⋅7 70 18⋅3 3⋅27 0⋅51 Primary school (5 years) 52 38⋅8 128 33⋅4
Secondary school (8 years) 21 15⋅7 47 12⋅3 High school (12 years) 24 17⋅9 79 20⋅6 University 16 11⋅9 59 15⋅4 Marital status Married 101 75⋅4 314 82 2⋅74 0⋅98 Single 33 24⋅6 69 18 Work Working 21 15⋅7 62 16⋅2 0⋅02 0⋅88 Not working 113 84⋅3 321 83⋅8 Economic status Lower average 62 46⋅3 141 36⋅8 4⋅50 0⋅10 Medium 56 41⋅8 175 45⋅7 Upper average 16 11⋅9 67 17⋅5 Family type Nuclear family 113 84⋅3 309 80⋅7 0⋅88 0⋅34 Extended family 21 15⋅7 74 19⋅3
CPP, chronic pelvic pain.
∗X ± SD = CPP 34⋅02 ± 10⋅58, Control 32⋅72 ± 10⋅82.
lupus, interstitial cystitis, cancer, depression, recurrent urinary tract infection and irritable bowel syndrome in family shows that those who have family members with recurrent urinary tract infection or cancer are 2⋅4–2⋅8 times more at risk of having CPP complaint (Table 2).
Although no differences were found between the case and control groups in term of their age of menar-che, continuation of menstruation and menstruation period (p> 0⋅05), menstrual pain was found to be sta-tistically significant in the case group (p< 0⋅05). Logis-tic regression analysis results indicate a significant relationship between them (Table 2).
An evaluation of the participants’ bladder and uri-nation habits shows that the women in the case group urinate more frequently, need to urinate with unimportant warnings, have difficulty in urinating, and frequently have urinary tract infections (p< 0⋅05). An analysis of the participants’ bowel and defaecation habits indicated a significant relationship between the case group participants’ pain and their defaeca-tion features (p< 0⋅05); the participants in the case group were found to have more defaecation problems
(defaecating less than three times a week, solid-hard defaecation, feeling of insufficient evacuation and feeling of fullness-swelling in the abdomen). The rela-tionship of CPP with micturition and defaecation habits was evaluated and it was found that CPP risk was higher especially in defaecation habits. The feeling of fullness in the abdomen was found to increase the risk 2⋅7 times more. The risk increased in a proportion of 5⋅3 in the relationship of pain and stool consistency (Table 2).
It was found that the proportion of a diagnosed woman disease was much higher in the CPP group and increased the risk of CPP 3⋅6 times more. Of the women in the CPP group, 11⋅9% had ovarian cyst, 7⋅4% had genital tract infection, 2⋅2% had prolapsus and 2⋅2% had menstrual irregularity. Any abdominal operation increases the risk 1⋅9 times more, and any infection in the genital organs increases the risk 4 times more. Falling down from height or having an accident that caused back damage increases CPP risk 4⋅2 times more. Taking a vaginal shower after sexual intercourse or for any other reason increases CPP risk three times more (Table 2).
Having any psychological health problem diagnosed by a doctor, experiencing a sad event in childhood, experiencing sexual abuse in childhood and/or adult, being forced to have sexual intercourse and being exposed to physical violence problems are evaluated in terms of their relationships with CPP; no relation-ships were found except for the findings in relation to childhood period. The proportions of increasing CPP risk were found to be 2⋅5 times more in a sad event experienced during childhood, 7⋅8 times more in being forced to sexual intercourse and 1⋅8 times more in being exposed to physical violence (Table 2).
This study aiming to identify the risk factors associ-ated with CPP has found that urinary, gastrointestinal, and musculoskeletal systems and psychological fac-tors affect women with CPP.
DISCUSSION
In line with the results of the studies (Mathias et al., 1996; Zondervan et al., 1999; Zondervan et al., 2001; Grace and Zondervan, 2004; Muhammad et al., 2011) conducted before CPP has been found to be a common health problem in women.
Studies show that CPP which causes problems with its peeks in the reproduction period is common mostly at the age of 30s. In their study conducted with 5263 women aged between 18 and 50 (CPP n = 773), Math-ias et al. (1996) aimed to identify the effects of CPP on women’s quality of life, performance (work life) and the status of benefitting from the health services and found
Table 2 Backward stepwise logistic regression analysis of risk factors for CPP
95⋅0% CIs for Exp (B) Risk factors 𝛽 Factor SE p Exp (B) Lower Upper Age <20 −0⋅065 0⋅501 0⋅896 0⋅937 0⋅351 2⋅499 20–29 −0⋅101 0⋅388 0⋅795 0⋅904 0⋅423 1⋅933 30–39 0⋅138 0⋅394 0⋅726 1⋅148 0⋅530 2⋅487 40–49 0⋅404 0⋅410 0⋅325 1⋅497 0⋅670 3⋅345 ≥50 −0⋅086 0⋅362 0⋅813 0⋅918 0⋅451 1⋅868 Number of pregnancies 0 0⋅145 0⋅279 0⋅603 1⋅156 0⋅669 1⋅999 1 −0⋅569 0⋅342 0⋅096 0⋅566 0⋅290 1⋅106 2 −0⋅326 0⋅291 0⋅262 0⋅722 0⋅408 1⋅275 3 −0⋅355 0⋅326 0⋅276 0⋅701 0⋅370 1⋅328 ≥4 0⋅235 0⋅221 0⋅288 1⋅265 0⋅820 1⋅950 Term delivery 0 0⋅285 0⋅326 0⋅381 1⋅330 0⋅702 2⋅520 1 −0⋅364 0⋅384 0⋅343 0⋅695 0⋅327 1⋅476 2 0⋅394 0⋅320 0⋅218 1⋅484 0⋅792 2⋅779 3 0⋅429 0⋅361 0⋅234 1⋅536 0⋅757 3⋅119 ≥4 −0⋅231 0⋅282 0⋅413 0⋅794 0⋅456 1⋅380 Delivery type Vaginal birth −1⋅821 0⋅383 0⋅000 0⋅162 0⋅076 0⋅343 Caesarean −0⋅484 0⋅321 0⋅131 0⋅616 0⋅328 1⋅156 Vaginal birth with episiotomy 0⋅231 0⋅257 0⋅368 1⋅260 0⋅761 2⋅087 Vaginal birth + caesarean 1⋅069 0⋅507 0⋅035 2⋅913 1⋅079 7⋅868 Birth by vacuum −0⋅286 0⋅732 0⋅695 0⋅751 0⋅179 3⋅150 Baby over 4000 kg −1⋅505 0⋅346 0⋅000 0⋅222 0⋅113 0⋅437 Family history
Urinary tract infection 1⋅043 0⋅258 0⋅000 2⋅838 1⋅712 4⋅705 Cancer 1⋅057 0⋅409 0⋅010 2⋅878 1⋅292 6⋅410 Chronic pelvic pain 0⋅880 0⋅236 0⋅000 2⋅411 1⋅518 3⋅830 Dysmenorrhea −0⋅466 0⋅120 0⋅000 0⋅628 0⋅496 0⋅795 Gynecological disorder 1⋅301 0⋅282 0⋅000 3⋅674 2⋅116 6⋅380 Vaginal shower 1⋅116 0⋅198 0⋅000 3⋅053 0⋅000 3⋅053 Operation/accident
Genital tract infection 0⋅391 0⋅220 0⋅000 4⋅017 2⋅608 6⋅188 Previous operations 0⋅692 0⋅240 0⋅004 1⋅998 1⋅248 3⋅199 Beck damage/Falling down 1⋅443 0⋅351 0⋅000 4⋅232 2⋅125 8⋅427 Bladder and urination habits
Urinate frequently 0⋅475 0⋅230 0⋅039 1⋅609 1⋅024 2⋅527 Need to urinate with unimportant warnings 0⋅597 0⋅243 0⋅014 1⋅817 1⋅129 2⋅924 Difficulty in urinating 0⋅890 0⋅275 0⋅001 2⋅435 1⋅421 4⋅172 Bowel and defaecation habits
Pain and stool consistency 1⋅683 0⋅280 0⋅000 5⋅384 3⋅112 9⋅314 Fullness-swelling in the abdomen 0⋅998 0⋅221 0⋅000 2⋅712 1⋅757 4⋅185 Psychologic factors
Sad event experienced in childhood 0⋅954 0⋅220 0⋅000 2⋅595 1⋅685 3⋅997 Sexual abuse during childhood 2⋅059 0⋅806 0⋅011 7⋅835 1⋅615 38⋅017 Physical violence during childhood 0⋅618 0⋅261 0⋅018 1⋅854 1⋅112 3⋅091 CPP, chronic pelvic pain; CI, confidence interval.
the average age of women with CPP as 35⋅7 ± 8⋅6 (p> 0⋅05). In their study which included 2016 women aged between 18 and 49 and aimed to identify CPP
prevalence and its effects on women’s life in Eng-land, Zondervan et al. (2001) found that with a propor-tion of 28%, CPP was common mostly among women
aged between 36 and 40 (p< 0⋅05). In a similar vein, Grace and Zondervan (2004) aimed to find out the CPP prevalence, pain severity, diagnosis and the sta-tus of benefitting from health services in 1160 women aged between 18 and 50 (CPP n = 286) and found that CPP prevalence was higher at the age of 30s than it was at the lower and upper age groups (p< 0⋅05). In the master thesis titled ‘CPP Prevalence, Risk Fac-tors and Effects on Quality of Life among Women aged between 15 and 49 in Sakarya’, CPP preva-lence was found to be most common at the ages between 25 and 29 (24⋅7%), secondly between the ages 30 and 34 (15⋅4%). However, the logistic regres-sion analysis results showed that age was not a risk factor for CPP (Ozdemir, 2012). This study has found that despite not being statistically significant, 30–39 and 40–49 age groups are partially at risk in terms of CPP.
The study conducted by Pitts et al. (2008) with 1983 Australian women aged between 16 and 49 aimed to identify the prevalence of three types of pain (dys-menorrhea, dyspareunia and CPP) and the associated factors; no significant relationship was found between pregnancy results and CPP. Ozdemir (2012) found that having a miscarriage, use of vacuum during deliv-ery, and developing vaginal laceration and bleeding after delivery in the obstetric history of women signif-icantly increased CPP prevalence but they were not risk factors for CPP. The relationship with CPP and obstetric history in this study has revealed that only women who experienced both vaginal and caesarean section are in the risk group. Besides, no significant relationships were detected between CPP and the number of pregnancies and number of terms. Despite not being significant, having had two and three deliv-eries were found to create a partial risk for CPP in women.
Ozdemir (2012) found that having dysmenorrhea and dyspareunia significantly increased CPP preva-lence and created an important risk factor for CPP. In line with this finding, this study has also revealed that women with CPP more frequently had dysmenorrhea and the relationship between them was found to be sig-nificant (p< 0⋅05).
Having fibromyalgia, CPP, scleroderma, endo-metriosis, lupus, interstitial cystitis, cancer, depres-sion, recurrent urinary tract infection and irritable bowel syndrome in family creates risk for CPP (Koyuncu, 2004). This study has also found that women who have someone with recurrent urinary tract infection, cancer and CPP in their families are 2⋅4–2⋅8 times more at risk of having CPP complaint (Table 2).
Ozdemir (2012) found that a diagnosed woman disease significantly increased CPP prevalence.
Logistic regression analysis shows that any gynae-cological disease diagnosed by a doctor created a risk factor for CPP. This study has also found that the proportion of a diagnosed woman disease was higher in the CPP group and the woman disease factor increased CPP risk 3⋅6 times more.
CPP is an important result of pelvic inflammatory disease (PID) and recurrent infections are common (Swanton and Reginald, 2004; Haggerty et al., 2005; Kroon and Reginald, 2005). Of the women whose PID was confirmed in laparoscopy, 20% had CPP com-plaint. Besides, CPP prevalence increased in the 67% of the women who had three or more PID attacks (Swanton and Reginald, 2004; Kroon and Reginald, 2005). This study has found that CPP risk increases four times more if there are any infections in the genital organs. Vaginal shower is a common prac-tice in our country (Sen and Mete, 2009; Sunay et al., 2011). Sunay et al. (2011) found that the risk of hav-ing abnormal vaginal discharge increases 3⋅9 times more in those who take vaginal showers. This study has revealed that women taking vaginal showers after sexual intercourse or for any other reason are three times more at risk for having CPP.
Considering an abdominal surgery experienced in the past is of great importance in CPP (Koyuncu, 2004). Ozdemir (2012) found that having an operation in relation to genital organs increased CPP prevalence. This study also has found that an abdominal operation increases CPP risk 1⋅9 times more.
Problems in relation to muscle–skeleton system are important and thus they should be taken into con-sideration both primarily and secondarily. Pain can develop as a result of a trauma happened in the pelvis caused by a traffic accident or pregnancy or degenerations or traumas in the related muscle groups (Swanton and Reginald, 2004). This study has found that falling from height or having an accident that caused back damage increase the risk of CPP 4⋅2 times more.
In their study which aimed to identify the preva-lence of voiding symptoms in women with CPP, Van Os-Bossagh et al. (2003) found that majority of the women with CPP had voiding symptoms and more fre-quently experienced all urinary symptoms than those in the control group. The study which included 60 women with CPP and 31 women without CPP revealed the problems experienced as incontinence for 43%, inad-equate voluntary control of the urethral sphincter for 50%, inability to postpone for 37%, urge for 37% and incomplete voiding for 37%. Similarly, this study has found that CPP is accompanied by urinary complaints. The women in the case group reported to urinate fre-quently, need to urinate with unimportant signs, have
difficulty in urinating and have frequent urinary tract infections (p< 0⋅05).
The most significant symptoms of irritable bowel syndrome which is common among young women and the most common gastrointestinal reason of CPP include stomach ache, feeling of swelling, changeable diarrhoea – constipation periods, pain before bowel movements and relaxation after defaecation (Kroon and Reginald, 2005; Longstreth et al., 2006). Ozdemir (2012) found that CPP prevalence increased with the complaints such as having frequent constipations and blood in stool, pain in bowel movements, anorexia and frequent nausea and vomiting. This study has also found the gastrointestinal complaints to be common and associated with CPP. Feeling of fullness in the abdomen increases the risk 2⋅7 times more, and the risk increases with the relationship between stool con-sistency and pain 5⋅3 times more.
More than 60% of the women with CPP were found to have psychological problems; the most frequently encountered one is depression (25–50%; Slade and Cordle, 2005). Studies show that there is a relation-ship between CPP and sexual/physical abuse (Walling et al., 1994a; Fry et al., 1997; Collett et al., 1998; Lampe et al., 2003; Leserman, 2005; Haugstad et al., 2006). In their study which aimed to compare sexual and physical abuse prevalence during childhood and adulthood in women with and without CPP (chronic headache) and without pain, Walling et al., (1994b) found that sexual abuse was more common in women with CPP. Collett et al. (1998) compared patients with and without CPP and found sexual abuse prevalence higher in CPP group. Meltzer-Brody et al. (2007) found that nearly 50% of the women with CPP had sexual or physical abuse history, and nearly one of three of them reported to have post-traumatic stress disorder. In this study, psychological health problems such as depression, anxiety, hysteria, extroversion, borderline, paranoia, post-traumatic stress, a sad event experi-enced in childhood, sexual abuse during childhood and adulthood, and being forced to sexual relationship or
WHAT IS KNOWN ABOUT THIS TOPIC
• CPP is a common health problem among women at reproductive age and it can have very negative effects on women’s both daily and work life.
WHAT THIS PAPER ADDS
• This case–control study has adopted a holistic approach for women and evaluated risk factors associated with CPP such as reproductive system, urinary system, gastrointestinal system, musculoskeletal system and psychological factors.
exposed to physical violence were evaluated in terms of their relationship with CPP and no relationships were detected except for findings in childhood. A sad event experienced in childhood increases CPP risk 2⋅5 times more, being forced to sexual relationship 7⋅8 times more and being exposed to physical violence increases the risk 1⋅8 times more.
Limitation of this study is that it is a hospital-based one. Society-based studies to be conducted with more participants would shed more light to the issues of CPP prevalence and the associated factors.
CONCLUSION
This study has found that CPP is a common problem in women and is associated with various factors such as gynaecological, urological, gastrointestinal, muscu-loskeletal systems and psychological factors. There-fore, it is important to evaluate women with a holistic and multidisciplinary approach.
IMPLICATIONS FOR PRACTICE
CPP is a common problem affecting the life of many women substantially. CPP requires a multidisciplinary team approach due to its complicated and multifactorial aetiology, and it is essential that nurses take place in this team work with their practitioner, educator, coun-sellor, coordinator and researcher roles.
CONFLICT OF INTEREST
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
ACKNOWLEDGEMENTS
We would like to thank to all the women who volun-teered to participate in the study. This study was not funded by any organization.
REFERENCES
Collett BJ, Cordle CJ, Stewart CR, Jagger C. (1998). A comparative study of women with chronic pelvic pain, chronic nonpelvic pain and those with no history of pain attending general practitioners. British Journal of Obstetrics and Gynaecology; 105: 87–92.
Fry RPW, Crisp AH, Beard RW. (1997). Sociopsychological fac-tors in chronic pelvic pain: a review. Journal of Psychosomatic
Research; 42 (1): 1–15.
Grace VM, Zondervan KT. (2004). Chronic pelvic pain in women in New Zealand: prevalence, pain, severity, diagnoses and use of the health services. Australian and New Zealand Journal of
Public Health; 28 (4): 369–375.
Gunter J. (2003). Chronic pelvic pain: an integrated approach to diagnosis and treatment. Obstetrical and Gynecological Survey;
58(9): 615–623.
Haggerty CL, Peipert JF, Weitzen S, Hendrix SL, Holley RL, Nel-son DB, Randall H, Soper DE, Wiesenfeld HC, Ness RB, PID Evaluation and Clinical Health (PEACH) Study Investigators. (2005). Predictors of chronic pelvic pain in an urban popula-tion of women with symptoms and signs of pelvic inflamma-tory disease. Sexually Transmitted Diseases; 32 (5): 293–299. Haugstad GK, Haugstad TS, Kirste UM, Leganger S, Wojniusz S,
Klemmetsen I, Malt UF. (2006). Posture, movement patterns, and body awareness in women with chronic pelvic pain.
Journal of Psychomatic Research; 61: 637–644.
Kennedy SH, Moore SJ. (2005). The initial management of chronic pelvic pain. Royal College of Obstetricians and Gynaecologist Guideline No: 41.
Koyuncu FM. (2004). Management of chronic pelvic pain.
TJOD-Training and Actual Development After Expertise; 1: 23–31
(In Turkish).
Kroon N, Reginald P. (2005). Medical management of chronic pelvic pain. Current Obstetrics and Gynecology; 15: 285–290. Lampe A, Doering S, Rumpold G, Solder E, Krismer M,
Kanther-Rumplmair W, Schubert C, Söllner W. (2003). Chronic pain syndromes and their relation to childhood abuse and stressful life events. Journal of Psychomatic Research;
54: 361–367.
Latthe P, Mignini L, Gray R, Hills R, Khan K. (2006). Factors pre-disposing women to chronic pelvic pain: systematic review.
British Medical Journal; 332: 749–755.
Leserman J. (2005). Sexual abuse history: prevalence, health effects, mediators, and psychological treatment. Psychosomatic
Medicine; 67: 906–915.
Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. (2006). Functional bowel disorders.
Gastroenterol-ogy; 130: 1480–1491.
Mathias SD, Cupperman M, Liberman RF, Lipschutz RC, Steege JF. (1996). CPP prevalence health related quality of life and economic correlates. Obstetrics and Gynecology; 87: 321–327. Meltzer-Brody S, Leserman J, Zolnoun D, Steege J, Green E,
Teich A. (2007). Trauma and posttraumatic stress disorder in women with chronic pelvic pain. Obstetrics and Gynecology;
109: 902–908.
Muhammad YY, Nossier SA, El-Dawaiaty AA. (2011). Prevalence and characteristics of chronic pelvic pain among women in Alexandria, Egypt. The Journal of the Egyptian Public Health
Association; 86: 33–38.
Ozdamar K. (2003). Biostatistic with SPSS. 5 edn. Eskisehir: Kaan Publication (In Turkish).
Ozdemir K. (2012). Chronic Pelvic Pain Prevalence, Risk Factors, and its Effects on Quality of Life Among Women Aged 15–49 and Lived in Sakarya. Master Thesis (Advisor: Ozerdogan N). Department of Obstetrics and Gynecology Nursing, Institute of Health Science, Eskisehir Osmangazi University, Eskisehir (In Turkish).
Pitts MK, Ferris JA, Smith AMA, Shelley JM, Richters J. (2008). Prevalence and correlates of three types of pelvic pain in nationally representative sample of Australian women. The
Medical Journal of Australia; 189 (3): 138–143.
Sen E, Mete S. (2009). Vaginal Douching Practices of Women in Turkey. Dokuz Eylul University Electronic Journal of Nursing
School; 2 (1): 3–15 (In Turkish).
Slade P, Cordle C. (2005). Psychological aspects of the manage-ment of chronic pelvic pain. Current Obstetrics and Gynaecology;
15: 298–305.
Sunay D, Kaya E, Ergun Y. (2011). Vaginal douching behavior of women and relationship among vaginal douching and vaginal discharge and demographic factors. Journal of Turkish Society of
Obstetrics and Gynecology;; 8 (4): 264–271 (In Turkish).
Swanton A, Reginald P. (2004). Medical management of chronic pelvic pain: the evidence. Reviews in Gynaecological Practice; 4: 65–70.
Van Os-Bossagh P, Pols T, Hop WCJ, Bohnen AM, Vier-hout ME, Drogendijk AC. (2003). Voiding symptoms in chronic pelvic pain (CPP). European Journal of Obstetrics and Gynecology and Reproductive Biology; 107:
185–190.
Walling MK, O’hara MW, Reiter RC, Milburn AK, Lilly G, Vincent SD. (1994a). Abuse history and chronic pain in women: I. Prevalences of sexual abuse physical abuse. Obstetrics and Gynecology; 84 (2): 193–199.
Walling MK, O’hara MW, Reiter RC, Milburn AK, Lilly G, Vincent SD. (1994b). Abuse history and chronic pain in women: II. A multivariate analysis of abuse and psychological morbidity.
Obstetrics and Gynecology; 84 (2): 200–206.
Zondervan KT, Yudkin PL, Vessey MP, Dawes MG, Barlow DH, Kennedy SH. (1999). Prevalence and incidence of chronic pelvic pain in primary care: evidence from national general practice database. British Journal of Obstetrics and Gynaecology;
106: 1149–1155.
Zondervan KT, Yudkin PL, Vessey MP, Jenkinson CP, Dawes MG, Barlow DH, Kennedy SH. (2001). The community preva-lence of chronic pelvic pain in women and associated illness behaviour. British Journal of General Practice; 51: 541–547.