Macroscopic footprint of the glenoid labrum
Tam metin
Şekil
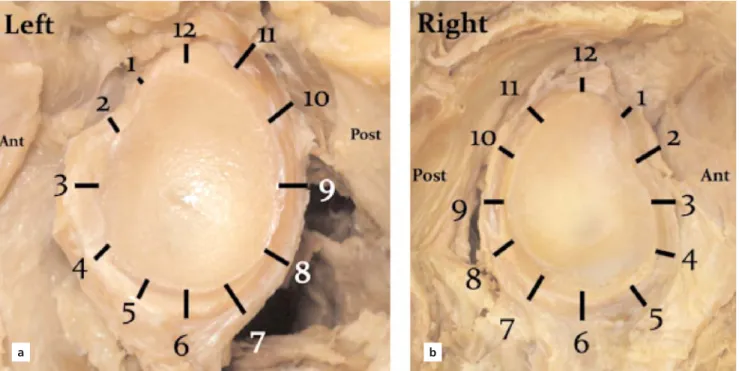
![Figure 1. Dissection of the glenoid, left shoulder. [Color figure can be viewed in the online issue, which is available at www.anatomy.org.tr]](https://thumb-eu.123doks.com/thumbv2/9libnet/4389036.74273/2.918.89.448.810.1058/figure-dissection-glenoid-shoulder-color-figure-available-anatomy.webp)
Benzer Belgeler
2 SBYLJ SEÇMELİ BİYOLOJİ 4 MESUT DEMİR. 3 SFZK SEÇMELİ FİZİK 4
ÇANKAYA BAHÇELİEVLER 100YIL MESLEKİ VE TEKNİK ANADOLU LİSESİ..
Major cellular response pathways to DNA damage including DNA repair, DNA damage checkpoints, apoptosis, and transcriptional reprogramming are gated by the circadian clock....
S.No Ders Dersin Adı Hs Yer Dersin Öğretmenleri..
Match the English sentences with the Turkish meanings.. Geç kaldığım için
[r]
In this study, we aimed to evaluate the ovarian reserve with basal hormone values and clomiphene citrate challenge test in patients with endometrioma, to compare results with
Bu yazıda angulus mandibula kırığına eşlik eden glenoid fossa kırığı bulunan bir olgu sunulmuş olup, ayrıca TME B T incelemesinin glenoid fossa kırıklarındaki
