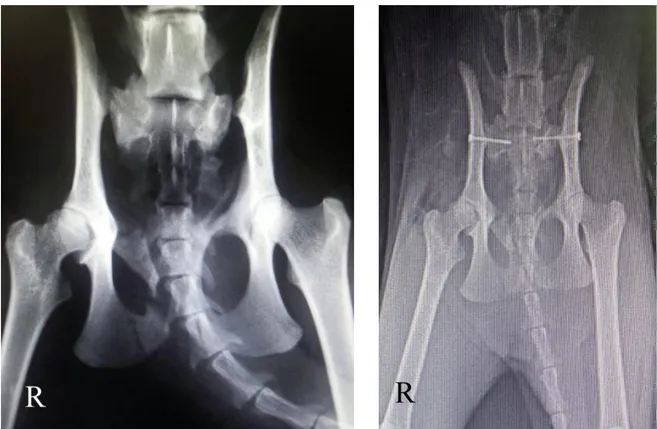
Başlık: Evaluation and surgical treatment of sacroiliac fracture-luxations in 28 cats and 25 dogsYazar(lar):ERGIN, Irem; SENEL, Oytun Okan; OZDEMIR, Ozge; ULUSAN, Sinan; BILGILI, Hasan Cilt: 63 Sayı: 2 Sayfa: 127-136 DOI: 10.1501/Vetfak_0000002720 Yay
Tam metin
Şekil


Benzer Belgeler
The purpose of this study was to evaluate the patients who underwent partial hip replacement surgery for femoral neck fracture by means of their Harris Hip score in order to
Twelve (10.3%) patients were with a history of fractures and 105 (89.7%) were without; 48 (41%) patients were clas- sified as having primary osteoporosis, and the remaining 69
Yozgat ve Çorum illerinde yaşayan bireysel yatırımcılar arasında araştırma bulgularından biri ise her iki gruptaki yatırımcıların yatırım aracı
In the context of psychological portrayal of female characters in novels of Anita Desai, Meena Belliappa observes: “What is new in Anita Desai is the effort to
Different proactive provisioning strategies are utilized in cloud environment and their execution changes with the sort of workload.[10] compared the five
Most other tourists mentioned that they did not consider higher prices to deter them from staying in an AA if the accommodation was able to create an authentic and highly
6818 - Define the effect size means for the experimental studies conducted in the period (2010-2020), addressed the effectiveness of using constructive learning
presented Line Edge Map(LEM) representation [8] in which face contours are extracted and combined in segments and then organized in lines. In this study, they have
