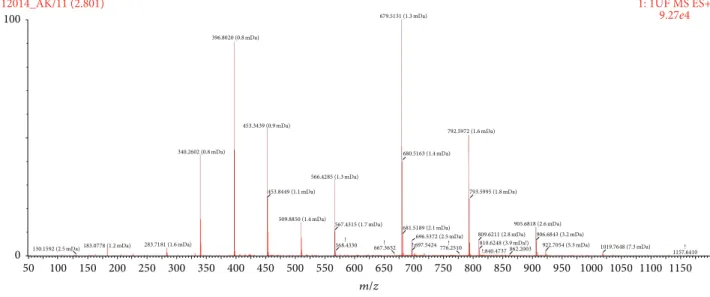
Qualitative/Chemical Analyses of Ankaferd Hemostat and Its Antioxidant Content in Synthetic Gastric Fluids
Tam metin
Şekil
Benzer Belgeler
In conclusion, a surge in capital inflows developing countries increases substantially aggregate expenditure and economic growth on the one hand, and generates
Sağlık Bilimleri Üniversitesi, Sultan Abdülhamid Han Eğitim ve Araştırma Hastanesi, Beyin Cerrahi Anabilim Dalı, İstanbul.. Sinir sisteminin tümörlerle çeşitli
療公益獎」方面,牙科部黃茂栓主任以照護特殊需求者的口腔,獲得「醫療貢獻
In conclusion, purified geraniin exhibited antioxidant activities, SSAO and ACE inhibitory activities, and antihypertensive effects on SHRs.. The results presented here will benefit
The third step of our study was testing the in vivo hemostatic effects of ABS Nanohemostat in comparison with the traditional Ankaferd in a previously established and
Bu yazıda sindesmos yaralanmasının eşlik ettiği distal fibula kırığı nedeni ile internal fiksasyon uyguladığımız bir hastada gelişen ve medikal tedaviye cevap vermeyen
Bu nedenle de tek bir dinin, ideolojinin, sınıfın hâkim olduğu veya tek bir devletin diğerlerini egemenliği altına aldığı Roma İmparatorluğu, Orta Çağ Kilisesi,
By scaling the values of the singular matrix properly these existing SVD based techniques enhances the contrast of image but the contrast in case of the original CT scan image is
