Feelings of burden among family caregivers of people with spinal cord injury in Turkey
Tam metin
Şekil
Benzer Belgeler
Bu kurala uygun olarak görselleri kesip bulmacaya yapıştırın..
30 DP’nin CHP iktidarı karşısındaki konumunu güçlendirmek ve siyasal varlığını meşru hale getir- mek amacıyla bir çare olarak kullandığı sine-i millete dönme
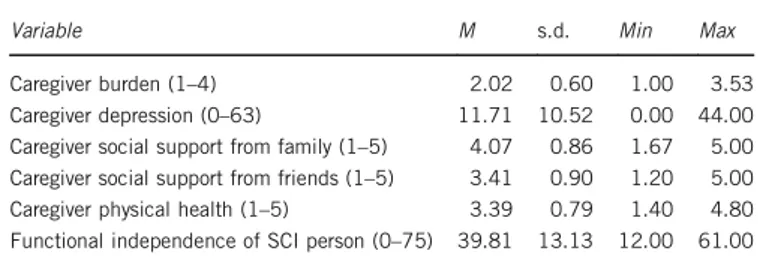
konusu tablo incelendiğinde, geven bitkisinin ham Geven bitkisinin Tablo 1'de verilen ADF ve NDF protein değerleri, KMSD, OMSD'leri yonca kuru değerleri göz önüne
臺北醫學大學 生物統計研究中心 2 在能力評量上,有兩種型式可供選擇: “自我挑戰” 及 “接受測驗”。 “自 我挑戰”
Resim mobilya olarak da kullanılabiliyor, roman vakit öldürmek için de okunabiliyor; şiir ise kendi a- kışı dışında yararlanılabilecek bir nitelik taşı mayan
[r]
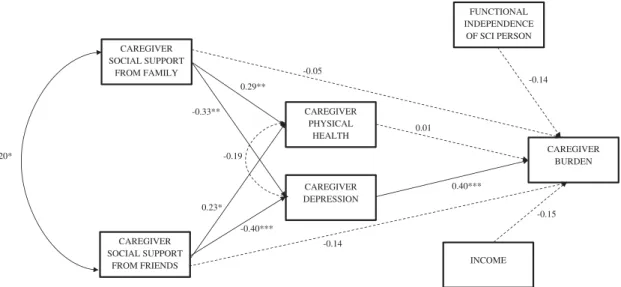
Bakım yükü, yaşam kalitesi ve algılanan sosyal desteğin birbirini etki- lediği, bakım yükü puan ortalaması arttıkça ebeveynlerin algıladıkları sosyal destek ve
SED assistance, a tool developed by the state to combat child poverty, is a form of economic support for children who are unable to access education, health
