Original
Article
Is
there
any
improvement
in
clinical
staging
with
18
F-FDG
PET/CT
compared
to
surgical
staging
in
cases
of
lung
cancer?
夽
Gonca
Kara
Gedik
∗,
Farise
Yilmaz
SelcukUniversity,FacultyofMedicine,DepartmentofNuclearMedicine,Konya,Turkey
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received15January2019 Accepted13May2019 Availableonline25June2019 Keywords: Clinical FDGPET/CT Lungcarcinoma Quantification Staging
a
b
s
t
r
a
c
t
Objective:18F-Fluorinefluorodeoxyglucosepositronemissiontomography/computedtomography(18
F-FDGPET/CT)imagingisconsideredthestandardimagingmodalityforpatientswithnon-smallcelllung carcinoma.Theaimofthisstudywastocompareclinicalstaging(cTNM)performedwith18F-FDGPET/CT
andsurgicalstaging(sTNM)inpatientswithnon-smallcellcarcinomatreatedwithsurgery.
Materialsandmethods:Weperformedaretrospectiveanalysisof99surgicalpatientswithnon-small cellcarcinomawhounderwent18F-FDGPET/CTexamination.Semiquantitativemeasureswere
calcu-latedfromtheprimarylesionsandmediastinallymphnodes.FindingsofcTNMwerecomparedwith finalsurgical–pathologicalevaluation.Subjectsweredividedintotwogroups aspostsurgicalcTNM changedandcTNMunchanged.PatientsinthecTNMchangedgroupwerefurtherclassifiedas postsurgi-calupstaged(US)anddownstaged(DS).ResultsoftheUSpatientswerecomparedwiththeresultsofthe remainingpatientsconsistingofcTNMunchangedandDStoevaluatethepredictablerolesof semiquan-titativeparametersforpostsurgicalupstaging.Todeterminemediastinaltumoralinvolvement,cut-off valueswereobtainedfromcalculatedsemiquantitativeresultsofFDGuptakesinlymphnodes.Apvalue <.05wasconsideredstatisticallysignificant.
Results:Subjectswereaged40–82yearswithameanageof64.78±8.70years.Classificationagreement wasobservedin43patients(43%)andin57%,postsurgicalstagemigrationwasseen.Concurrenceof cTNMandsTNMwasmorepronouncedintheT1andN0subsetswhichwere84%and74%,respectively. ThelowestconcurrencewasobservedinN1classificationfollowedbyT4andN2(1%,50%and58%, respectively).ChangeinTstagingoccurredin20of56(36%),inNstaging22of56(39%)andchangeinT andNin14patients(25%).DistributionofUSandDSpatientsinthecTNMchangedgroupwas,43%(24 of56)and57%(32of56),respectively.Resultsofsemiquantitativemeasuresweresignificantlyhigherin USpatientsthantheresultsofthegroupconsistingofDSpatientsandcTNMunchangedpatients,forall parameters.Cut-offvaluecalculatedfrommediastinaluptakeswasmostspecificformetastasesinMTV (metabolictumorvolume)withanacceptablesensitivity(90%and67%,respectively).
Conclusions: TheconcordancebetweencTNMandsTNMwasbetterinstagingTcategorycompared toNstations.Semiquantitativemeasuresofprimarytumormayplayaroleinpredictingpostsurgical upstaging.TakingMTVintoconsiderationinthemediastinalregionmaybemorevaluablethanother parametersintheassessmentofnodalinvolvement.
©2019Sociedad Espa ˜noladeMedicinaNucleareImagenMolecular.PublishedbyElsevierEspa ˜na,S.L.U.Allrightsreserved.
¿Hay
alguna
mejora
en
la
estadificación
clínica
con
PET/TC
con
18F-FDG
en
comparación
con
la
estadificación
quirúrgica
en
el
cáncer
de
pulmón?
Palabrasclave: Clínico FDGPET/TC Carcinomadepulmón Cuantificación Estadificación
r
e
s
u
m
e
n
Objetivo: La imagen detomografíapor emisión depositrones/tomografía computarizada con 18
F-fluordesoxiglucosa(18F-FDGPET/TC)seconsideraunamodalidaddeimagenestándarenpacientescon
carcinomadepulmóndecélulasnopeque ˜nas.Elobjetivodeesteestudiofuecompararlaestadificación clínica(cTNM)realizadacon18F-FDGPET/TCylaestadificaciónquirúrgica(qTNM)enpacientescon
carcinomadecélulasnopeque ˜nastratadosconcirugía.
Materialymétodos:Realizamosunanálisisretrospectivode99pacientesconcarcinomadecélulasno peque ˜nasintervenidosquirúrgicamentealosqueserealizóunestudio18F-FDGPET/TC.Serealizaron
medidassemicuantitativasenlaslesionesprimariasylosganglioslinfáticosmediastínicos.Loshallazgos decTNMsecompararonconlaevaluaciónquirúrgica-patológicafinal.Lospacientessedividieronendos grupos,qTNMposquirúrgicomodificadoyqTNMnomodificado.Lospacientesenelgrupoconcambio deqTNMseclasificaronadicionalmentecomoupstaged(US)ydownstaged(DS)postquirúrgicos.Los
夽 Pleasecitethisarticleas:GedikGK,YilmazF.¿HayalgunamejoraenlaestadificaciónclínicaconPET/TCcon18F-FDGencomparaciónconlaestadificaciónquirúrgicaen elcáncerdepulmón?RevEspMedNuclImagenMol.2019;38:348–354.
∗ Correspondingauthor.
E-mailaddress:[email protected](G.K.Gedik).
resultadosdelospacientesUSsecompararonconlosresultadosdelospacientesrestantes,queconsistían enqTNMsincambiosyDS,paraevaluarelposiblepapelpredictivodelosparámetrossemicuantitativos enlaestadificaciónpostoperatoria.Paradeterminarlaafectaciónmediastínicatumoral,seobtuvieron valoresdecortedelosresultadossemicuantitativosdecaptacióndeFDGenlosganglioslinfáticos.Un valorp<0,05fueconsideradoestadísticamentesignificativo.
Resultados:Lospacientesteníanentre40y82a ˜nos,conunaedadmediade64,78±8,7a ˜nos.Seobservó unacuerdodeclasificaciónen43pacientes(43%),yen57%seobservómodificaciónenlaestadificación posquirúrgica.LaconcurrenciadecTNMyqTNMfuemásdestacadaenlaclasificaciónT1yN0,convalores de84%y74%,respectivamente.LaconcurrenciamásbajaseobservóenlaclasificaciónN1seguidadeT4 yN2(1%,50%y58%,respectivamente).ElcambioenlaestadificaciónTocurrióen20de56pacientes (36%);elcambioenlaestadificaciónN,en22de56(39%);yelcambioenTyN,en14pacientes(25%).La distribucióndepacientesdeUSyDSenelgrupoconcambiodecTNMfuede43%(24de56)y57%(32 de56),respectivamente.Losresultadosdelasmedidassemicuantitativasfueronsignificativamentemás altosenlospacientesdeUSquelosresultadosdelgrupocompuestoporpacientesconDSyqTNMsin cambios,paratodoslosparámetros.Elvalordecortecalculadoapartirdelascaptacionesmediastínicasfue másespecíficoparametástasisenelMTV(volumenmetabólicotumoral)conunasensibilidadaceptable (90%y67%,respectivamente).
Conclusiones: LaconcordanciaentreTNMyqTNMesmejorenlaclasificacióndelacategoríaTen com-paraciónconlacategoríaN.Lasmedidassemicuantitativasenlostumoresprimariospuedenjugarun papelenlaprediccióndelUSposquirúrgico.ElMTVenlaregiónmediastínicapuedetenerunmayorvalor queotrosparámetrosenlaevaluacióndelaafectaciónganglionar.
©2019SociedadEspa ˜nolade MedicinaNucleareImagenMolecular.PublicadoporElsevierEspa ˜na,S.L.U.Todoslosderechosreservados.
Introduction
Lungcarcinomaistheleadingandthesecondmostcommon causeofcancerdeathamongmenand women.1 Accurate stag-ing, which includes delineation of the extent of disease, both loco-regionallyandatdistantsites,isimportantforselectingthe appropriatetherapeuticregimen.Moreover,staging,whichisbased onprimarytumor(T),regionallymphnodesand(N)andmetastases (M)system,isthesinglemostimportantprognosticfactorfor pre-dictingtheoutcomesofbothsurgicalandnonsurgicalpatientswith lungcarcinoma.2
Currently, two primary lung cancer staging procedures are available: clinical staging, which is provided by noninvasive imaging procedures, or minimally invasive approaches, such as mediastinoscopy.3 For the pathologic staging, information is obtainedfrominvasivesurgeryandthepathologicevaluationofthe excisedtumor.Clinicalstagingcandonewithpreoperative imag-ingtechniquesincludingcomputedtomography(CT)andpositron emissiontomography/computedtomography(PET/CT)performed with18Fluorinefluorodeoxyglucose(18F-FDG).Withthesizebased criteriaformalignancy,CThasalimitedsensitivityandspecificity, especially in nodal staging of mediastinum.4 Mediastinoscopy, whichisconsideredtobegoldstandardformediastinallymphnode staging,isunreliablein<10%ofcasesforlymphnodesmeasuring <1cm.5Surgicalstaging,ontheotherhand,makesavailablegreater certaintyaboutprognosisandisusefulinmakingdecisionsabout adjuvanttherapyaftersurgery.6AstudycomparingimagingTNM andpathologicalTNMinstaginglungcarcinomawithCTpointed outthelowdiagnosticaccuracyofclinicalstagingascomparedwith pathologicalstaging.6,7
18F-FDGPET/CTisincreasinglybeingusedfordiagnosis,staging andforevaluationoftherapyresponseinvarioustumorsincluding lungcarcinoma.Improvementinstagingofpatientswithlung car-cinomahasbeenshownwithintegrated18F-FDGPET/CTsystems comparedtoPETsystemsalone.8,9Besideshavingtheabilityof ana-lyzingcellmetabolism,18F-FDGPET/CTalsoofferssemiquantitative metabolicparametersofthetumorwhichgiveinformationabout metastaticpotentialandriskofrecurrence.Althoughmaximum standarduptakevalue(SUVmax)isthemostcommonlyusedone inclinicalpractice,theroleofmetabolictumorburdenasmeasured withmetabolictumorvolume(MTV)ortotallesionglycolysis(TLG)
hasbeenintroducedandhavebeensuggestedasyielding prognos-ticinformationonsurvivalandgivingbetterprognosticmeasures thanSUVmaxinpatientswithnonsmallcelllungcancer.2,10–12
Theaimofthisstudywastocompareclinicalstagingperformed with18F-FDGPET/CTandsurgicalstaginginpatientswithlung car-cinomatreatedsurgically.Theroleofsemiquantitativeparameters derivedfromprimarytumorandmediastinallymphnodes,as pre-dictorsofpostoperativeupstagingandmediastinalinvolvement, havealsobeenevaluated.
Materialsandmethods
Patients
Thefilesof691patientswithlungcarcinoma,whounderwent 18F-FDGPET/CTbetweenSeptember2012andDecember2018in SelcukUniversityMedicalFacultyDepartmentofNuclearMedicine, wereretrospectivelyreviewed.Patientswithhistologicallyproven lung cancer, who had undergone an 18F-FDG PET/CT scanning for stagingand had beensurgicallytreated afterimaging, were selected.Patientswithsmallcellcarcinoma,patientswhose patho-logicaldataofthesurgicalspecimencouldnotbetherecovered andcasesinwhominductiontherapywasdeliveredafter18F-FDG PET/CT,wereexcludedfromthestudy.Thisstudywasapprovedby thelocalethicscommitteeofourfaculty(meetingdate:24.10.2018, decisionnumber:2018/366)andwritteninformedconsentform wasobtainedinallpatients.
18F-FDGPET/CTscanning
18F-FDG PET/CTimaging wascarried outwith anintegrated scanner(BiographmCT,Siemens,Germany)in8or9bedpositions withanacquisitiontimeof2minperbedpositionfromskullbase tothemidthigh.Allpatientswereaskedtofastatleast6hbefore theexaminationandbloodsugarlevelswereconfirmedtobeless than200mg/dLbeforetheinjectionof370MBqof18F-FDG.Sixty minutesaftertheadministrationoftheradiopharmaceutical,alow doseunenhancedCTusingthe16sliceCTwithacquisition parame-tersof190mA,5mmslicethicknessand140kVwasperformedfor attenuationcorrection,whichwasfollowedbythePETacquisition.
Imageinterpretationandsemiquantification
18F-FDGPET/CTimageswereinterpretedandsemiquantitative analysisof18F-FDGuptakewascalculatedonaSiemensSyngo.via PET/CTworkstation.Ineachpatient,a1.0cmdiameterregionof interest(ROI)wasmanuallyplacedovertheprimarylunglesion andsuspiciouslymphnodestationsontheattenuationcorrected 18F-FDGPETimagesontheslicewiththehighest18F-FDGuptake. Theactivity concentrationwithin theROI was determined and expressedasSUVwhichwascalculatedusingtheformulabelow: activityintheregionofinterest(MBq/mL)/(injectedactivity/body size).From these ROIs,SUVmax and peak standardized uptake value(SUVpeak)werecalculated,bothofwhichwerenormalized tobodyweight.Fordeterminingmediastinalandhilarlymphnode status,werandomlyselected50patients,drewa1.0cmdiameter ROIinthecenterofsuperiorvenacavaandcalculatedthemeanof theirSUVmaxtorepresentbloodpoolSUV,whichwascalculatedas 3.30.ForMTVandTLGcalculation,40%oftheSUVmaxwasadopted asthethresholdtodelineatethetumor;MTVandTLGoftheprimary tumorandmediastinallymphnodewereautomaticallymeasured bythesoftware.
Dataanalysis
Ineachpatientsizeoftheprimarytumor,presenceof medi-astinal and/or hilar lymph nodes and distant metastases were evaluatedandpatientswereclinicallystaged(cTNM)accordingto theeightheditionofTNMclassificationforlungcancer,takingthe findingsofthe18F-FDGPET/CTexaminationintoconsideration.1 Patientsinwhomnolymphnodesinthemediastinalregionwere observedortheoneswithnodaluptakeofSUVmaxbelow3.30; werestagedasN0.Anynodaluptakeoverthevalueof3.30was recordedandconsideredaspositive fortumoralinvolvementof mediastinaland/orhilarlymphnodes.Incasesofmultiplelymph nodeshaving18F-FDGuptakeaboveourthresholdinN2stations, theresultofthehighest18F-FDGuptakewasusedinanalysis. Semi-quantitativemeasurementsoflunglesionsandnodaluptakeswere noted.
Pathologicandsurgicaldataforallpatientswereobtainedfrom theelectronicmedicalrecordsystemofourhospital.Forsurgical staging(sTNM),thesameclassificationsystemwasused. Compar-isonofcTNMandsTNM wasperformedregarding sTNMasthe goldstandard.AftercomparingthecTNMandsTNM,subjectswere dividedinto2groups:cTNMchangedandcTNMunchanged post-operatively.PatientsofcTNMchangedpostoperativelygroup,were furtherclassifiedinto2groupsasupstaged(US)anddownstaged (DS).Besideschangesbetweendifferentstages,changeswithinthe samestage(e.g.:changefromstageIA3toIA2orfromstageIIA toIIB)wasalsotakenintoaccountandregardedasdownstaged orupstaged,respectively.Inordertoevaluatethepredictiveroleof semiquantitativeparameteresforpostsurgicalupstaging;resultsof patientsinUSgroupwascomparedwiththeresultsofthe remain-ingpatientsconsistingofcTNMunchangedandDS.
Statisticalanalysis
ThesoftwarepackageSPSSv16.0wasusedtocarryoutthe sta-tisticalanalysis.ResultsofSUVmax,SUVpeak,MTVandTLGwere expressedasmean±SDormedian.Mann–WhitneyUtestwasused tocomparetheresultsofsemiquantitativeanalysisoftheprimary tumorindifferenthistologicaltypesandalsotocomparetheresults ofpatientsinUSandtheresultsofthegroupofpatients contain-ingcTNMunchangedandDS.ResultsofUSandDSpatientswere alsocomparedbyMann–WhitneyUtest.Fromsemiquantitative measuresobtainedfrommediastinallymphnodes,cut-offvalues werecalculatedfortheirabilitytopredictnodalmalignancy,by
ROCcurveanalysis.Thep-valueswereconsideredstatistically sig-nificantif<0.05.
Results
Our retrospective study included 99 patients (83 male, 16 female, age range: 40–82 years, mean age: 64.78±8.70). All patientsweretreatedsurgically.Systematiclymphnodedissection wascarriedoutinstations2,4,7,8,9,10inrightsidedtumorsand in5,6,7,8,9,10forleftsidedtumors.RemainingN1nodeswere resectedaspartofthesurgicalspecimen.Histologicalanalysisof theprimarytumorrevealedadenocarcinomain44patients, squa-mouscellcarcinoma(SCC)in46,largecellneuroendocrinetumor in6,carcinoidtumorin2andlargecellcarcinomain1patient.
Inallpatients,SUVmaxoftheprimarytumorwasdetermined.In 12patients,inwhichthe18F-FDGPET/CTstudieswerenotavailable, thevaluesofSUVmaxofprimarytumorsandmediastinallymph nodeswererecordedfromthereportsofthepatients;theseresults wereincludedin thereview.However,SUVpeak, TLGandMTV oftheprimarytumorandmediastinallymphnodescouldnotbe calculated.ThemeanandmedianSUVmaxvalueswerehigherin patientswithSCCthanintheoneswithadenocarcinoma,which werecalculated as16.43±10.54and 14.62and 10.19±7.4 and 8.43, respectively(p=0.0001).Among the87 patientsinwhom allsemiquantitativeparameterscouldbecalculated(39patients withadenocarcinoma,39withSCC,9withotherhistologicaltypes), meanandmedianSUVpeak,TLGandMTVvalueswereallhigher inpatientswithSCCthaninpatientswithadenocarcinomaand thedifferenceswerestatisticallysignificant(p<0.05).Theresults ofsemiquantitativemeasurementsofprimarytumorsofdifferent histopathologictypesaredepictedinTable1.
Outof99patients,cTNMrevealedthat1patientwasinstageIA1, 10wereinIA2,20wereinIA3.Therewere20patientsincIB,7in cIIA,19incIIBandfinally15incIIIA,7incIIIB.Noneofthepatients werenotedtohavedistantmetastases.cTNMchanged postoper-ativelyin56patients(57%)andunchangedintheremaining43 (43%,Fig.1).sTNMdemonstratedthat,7patientswereinstageIA1, 13instageinIA2and16wereinsIA3.Therewere20patientsin sIBgroup,8insIIAand19insIIBcategory.SurgicalIIIAandIIIB classesincluded13and 3patients,respectively.Change in sub-stageoccurredin19of56patients(34%),whereasin37patients (66%)achangeofcTNMwasobservedbetweenstages.Comparison ofcTNMandsTNMissummarizedinTable2.
DiagnosticaccuracyincTstagingwashigherthanofcNstaging whichwerecalculatedas72%and62%,respectively.Concurrence ofcTNMandsTNMwasmorepronouncedinT1andN0subsets whichwere84%and74%,respectively.Thelowestconcurrencewas observedinN1classificationfollowedbyT4andN2(1%,50%and 58%,respectively).ChangeinTstagingoccurredin20of56(36%), inNstaging22of56(39%)andchangeinTandNin14ofthem (25%).Among56patientswhosecTNMwerechanged,upstaging wasobservedin24of56(43%,Fig.2)anddownstagingin32(57%,
Fig.3).InpatientsofUSgroup,Tupstagingwasobservedin10of 24(42%),Nupstagingin10of24(42%)andTandNupstagingin 4ofthem(16%).InpatientsofDSgroup,downstageinTstagewas presentin10of32(31%),downstaginginNstageoccuredin12of 32(38%)andTandNdownstagingwasobservedin10of32patients (31%).ComparisonsofcTNMandsTNMinTandNcategoriesare outlinedinTables3and4.
Theanalyses which werecarried out toinvestigatethe role ofsemiquantitativemeasuresinpredictingpostsurgical upstag-ing revealed that all parameteres were significantly higher in US patientsthan theresults ofthe groupconsisting of DS and cTNMunchangedpatients(p<0.05).Themeanandmedian val-uesofSUVmaxoftheprimarytumorinUSandDSgroupswere
Table1
SemiquantitativeresultsofprimarytumorsinofdifferenthistopathologicaltypesofNSCLC.
SUVmax SUVpeak TLG* MTV*
Adenocarcinoma(mean/median) 10.19±7.4/8.43 7.71±6.43/5.98 21.85 5.72
SCC(mean/median) 16.43±10.54/14.62 12.43±8.71/11.58 74.30 8.76
pValue 0.0001 0.001 0.001 0.0039
NSCLC:non-smallcelllungcarcinoma,SCC:squamouscellcarcinoma.
*Onlymedianvaluesareexpressedbecauseofhighlevelsofstandarddeviationinmeanvalues.
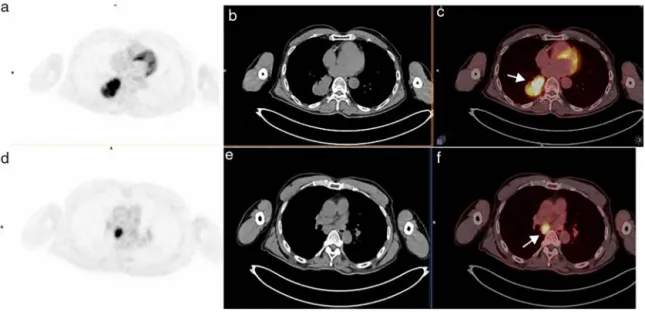
Fig.1.TransaxialPET(a),CT(b),andfused(c)imagesof68yearoldmalepatientshowedaprimarytumorinthelowerlobeoftherightlungwithalongestdiameterof 61mm,whichwasdiagnosedassquamouscellcarcinoma(arrow,c)InthetransaxialPET(d),CT(e),andfused(f)imagesofthesamepatient,subcarinallymphnodeswitha SUVmaxof16.47wereobserved,whichwerefinallyconfirmedasmetastatic(arrow,f).Calculatedsemiquantitativevaluesforlymphnodeswereallabovethecut-oflevels determinedforthem,includingMTV.ThispatientwasclinicallyandsurgicallystagedasT3N2.
Table2
Comparisonofclinicalandsurgicalstaginginwholepatients.
cTNM sIA1 sIA2 sIA3 sIB sIIA sIIB sIIIA sIIIB Total
IA1 1 1 IA2 3 6 1 10 IA3 3 9 5 3 20 IB 2 11 6 1 20 IIA 4 2 1 7 IIB 1 2 3 2 1 6 4 19 IIIA 2 2 2 1 3 4 1 15 IIIB 1 1 3 2 7 Total 7 13 16 20 8 19 13 3 99 Agreement(c/p) 14% 46% 56% 55% 50% 32% 31% 67% 43%
Fig.2. IntransaxialPET(a),CT(b),andfused(c)imagesofa68yearmalepatientwhowasclinicallystagedasT2aN0,aprimarytumorlocatedintheupperlobeofleftthe lungwasobserved(arrow,c).Inthehistopathologicalanalysis,besidesmaintumor,asatellitenoduleinthesamelobeconsistentwithadenocarcinomawasalsoreported. ThepatientwasfinallystagedassT3N0.
calculatedas14.52±6.02and13.91intheUSgroupcomparedto 13.05±11.92and9.47intheDSgroup,respectivelyandthe dif-ferencebetweenthemwasnotstatisticallysignificant(p=0.061). InthecTNMchanged group;SUVpeak, TLGandMTV couldbe calculatedin47patients,22wereUSand25wereDS.Meanand
medianvaluesofSUVpeakwere11.49±5.32and10.51inUSgroup and10.13±10.56and7.05inDSgroup,respectively.LikeSUVmax, thedifferenceofmedianvaluesbetweenUSandDSgroupswas notfoundasstatisticallysignificant(p=0.105).However,whenwe lookedattheTLGandMTVvaluesofprimarytumorsinUSandDS
Table3
Comparisonofclinicalandsurgicaltumorstaging.
cTNM sT1 sT2 sT3 sT4 Total T1 38 8 – – 46 T2 7 25 5 – 37 T3 – 2 8 3 13 T4 – – – 3 3 Total 45 35 13 6 99 Agreement(c/p) 84% 71% 62% 50% 72% Table4
Comparisonofclinicalandsurgicalnodalstaging.
cTNM sN0 sN1 sN2 sN3 Total N0 55 13 1 – 69 N1 7 2 1 – 10 N2 11 2 4 – 17 N3 1 1 1 – 3 Total 74 18 7 – 99 Agreement(c/p) 74% 1% 58% – 62% Table5
ResultsofsemiquantitativeparametersofprimarytumorsincTNMchangedgroup.
SUVmax SUVpeak* TLG* MTV*
US(mean/median) 14.52±6.02/13.91 10.51 94.44 10.67 DS(mean/median) 13.05±11.92/9.47 7.05 22.05 4.08
pValue 0.061 0.105 0.013 0.006
US:upstaged,DS:downstaged.
* Onlymedianvaluesareexpressedbecauseofhighlevelsofstandarddeviation inmeanvalues.
groups,medianTLGwascalculatedas94.44inUSgroupand22.05 inDSgroup.MedianvalueofMTVinUSgroupwasagainhigherthan thevalueinDSgroup(10.67vs.4.08),andthestatisticalanalysis showedsignificantdifferenceforbothparameters(p=0.013and p=0.006,respectively).Theresultsofsemiquantitativeparameters oftheprimarytumorsforUSandDSpatientsareshowninTable5. Topredictmediastinallymphnodemetastases,acut-offvalue of5.05wascalculatedwiththesensitivityandspecificityof60% and64%,respectivelyforSUVmax.ForSUVpeak,cut-offvaluewas foundas3.84with67%sensitivityand75%specificity.Areasunder curveswere0.632forSUVmaxand0.731forSUVpeak.Ontheother hand,forvolumetrictumorparametersthecut-offvaluewas4.23 withasensitivityof67%andspecificityof90%forMTVand12.97 forTLGwithsensitivityandspecificityof78%and75%,respectively. Areasunderthecurveswerefoundas0.786forMTVand0.772for TLG.
Discussion
Studiescomparingclinicalandpathologicstaginginlung carci-nomaunderlinetheinaccuracyofclinicalstagingand,furthermore pooledresultssupportthatthetrueextentofintrathoracic dis-easeisunderoroverestimatedinspiteofthetechnologicadvances inimagingmodalities.4,6,7,13Gdeedoetal.reportedthat,imaging TNMprovidesnoaccurateinformation,CTisinadequatefor medi-astinallymphnodestagingandT3andT4determinationsofCTare unreliableinlungcancer.7ThelimitedroleofCTin demonstrat-ingmediastinalinvolvementandinT4definitioninpatientswith non-smallcarcinomawerealsoemphasizedinanotherstudyby C¸etinkayaetal.,later.4AnotherstudybyLopez-Encuentraetal., compared clinicalagainst pathological staging in 2994cases of lungcancer,foundlowdiagnosticaccuracyofclinicalstagingand finalizedtheirreportwiththehopesofintegratedPETsystemsto improveclinicalTNstaging.6Vermaetal.,lookedforananswer forthisquestionrecently;reported42%TNMupstagedpatients
postoperativelyandfoundoutthathighprimarytumorSUVmax ofadenocarcinomamightpredictpostsurgicalupstaging.14
Wefoundaclinicalandsurgicalconcurrenceof43%and post-operativestagechangingwasobservedinmorethanhalfofthe patientsinwhomdownstagingwasmoreprominent.Inthe con-ductedstudiescomparingclinicalstagingwithsurgicalstagingin lungcarcinomabeginningfromtheearly1990s;56%,1535%7 and
47%4,6,13agreementlevelswerereportedinpatientsmajorityof
whomunderwentCT.Althoughdifferentclinicalstagingmodality andaTNMstagingsystemconsistingofmoresubstageswasused, ourresultwassimilarwiththelevelof47%whichwasreported bymostoftheexperiences.Weobservedhigheraccuracyinthe determinationofTstatusthanNstations(72%and62%, respec-tively;Tables 3and4)whichwasalsoasimilarresultwiththe otherstudies.4,7,11,13,15
Overestimationorunderestimationofthestagingvariesamong studies and this is mostly caused by false negative or positive interpretationsofmediastinalnodalassessments.Withtheclinical introductionofofintegratedFDGPET/CTclinically,improvement initsdiagnosticpowerandaccuracyofstaginginnonsmallcell car-cinomacomparedtoPETsystemsalonehasbeenwellestablished. TheeffectivenessofFDGPET/CTsystemsindecreasingthenumber offutilethoracotomiesandalsoshowingunexpectedmetastatic diseaseisdemonstratedaswell.16,17IntegratedFDGPET/CTisalso usefulforpredictingnegativityofthemediastinallymphnode sta-tus,howeverfalsepositiveresultscausedbyinflammatoryprocess hasbeenreportedinmediastinalstationswhichwasalsoobserved byus.Elevenofthe17patients(65%)whowereclassifiedascN2 and7of 10patients(70%) ofcN1werefinallystagedassN0in ourstudy(Table4).Thereisnotanyconsensusintheliterature forcut-offvaluesofSUVmaxinmediastinallymphnodesinorder toclarifytheonescontainingtumorcellsandrecommended val-uesrangefrom2.5–5.3.18Becauseofthiswidespectrumofcut-off values,wecalculatedthemeanoftheSUVmaxofbloodpoolfrom randomlyselectedpatientsassuggestedintheliterature.18 How-everoureffortsofcalculatingameanvalueinsteadofregardingan arbitrarycut-offcouldnothelpusandtheunreliabilityof mediasti-nalnodalassessmentstillexistedinourstudy.False-positivelymph nodesexceedingourthresholdvalueof3.30wererelatedto inflam-matoryreactionincludingallof3patientswhowereclassifiedas cN3whofirstgonethroughmediastinoscopyandlatertoracotomy whenmetastaticinvolvementwasruledout(Figs.3and4).Onthe othersideofthecoin,13of18patients(72%)ofsN1category,were falsenegativelystagedascN0andonly2ofthem(1%)couldbe cor-rectlyclassified(Table4).Thisinaccuracyofpredictinghilarlymph nodeinvolvementwasalsoobservedbyC¸etinkayaetal.andLin etal.,4,18Al-Sarrafetal.,showedthatthedistinctionbetween pri-marytumorandadjacentlymphnodeinvasioncanbedifficultin casesofhilartumors.19Inourstudy,7of13(54%)patientshadhilus locatedtumorallesionswhichsupportsthishypothesis;howeverin 6,thelocationsoftumorswereoutsidethehilum,butwewerestill unabletodiscriminateperibronchialandintrapulmonarylymph nodeinvolvement,theresolutionofcurrentFDGPET/CTsystems.
In terms of cTstaging, thehighest diagnosticaccuracy was observedinT1assessments(84%)andthelowestinT4(50%).When welookedatthesubstagesofT1category;FDGPET/CTwasable todiscriminateT1ctumorsbetterthanothercategoriesandwas worstatdefinitionofT1a(65%and44%clinicalandsurgical con-cordance,respectively).Inthe8theditionTNMstagingsystem,7 categoriespersizeascomparedwith6thecategoriesexistwith1 moresubdivisioninT1categorywhichmakesdifficulttoresolve thetumorsofsmallerthan1cmstandinginT1acategorywhichwas alsomentionedbyKandathiletal.20Althoughthespatialresolution hasimprovedfrom25mmto5mmwithimprovementin scan-nerdesignandperformance,21 inaccuraciesexistinmicroscopic determinationoftumormarginswhichwasalsoemphasizedby
Fig.3. TransaxialPET(a),CT(b),andfused(c)imagesofa68yearoldfemalepatientdepictedtheprimarytumorintheupperlobeoftherightlung(arrow,c).Mediastinal windowoftransaxialPET(d),CT(e),andfused(f)imagesofthesamepatientshowedlymphnodewithelevatedFDGuptakeintherightparatrachealregion(arrow,f). SUVmaxofthelymphnodewascalculatedas9.51,thepatientwasclinicallystagedascIIIA.Histopathologicevaluationrevealedinflammatoryreactioninthelymphnode andconfirmedadenocarcinomaintheprimarytumorsothefinalstageofthepatientwassIA2.ThecalculatedMTVlevelfromthislymphnodewasfoundas3.98.
Fig.4.IntransaxialPET(a),CT(b),andfused(c)imagesofa70yearoldmalepatient,theprimarytumorlocatedinthelefthilium(arrow,c)whichthenprovedas adenocarcinoma,wasseen.TransaxialPET(d),CT(e),andfused(f)imagesofsamepatientshowedincreasedFDGuptakewithcalculatedresultsof7.70and3.88forSUVmax andMTVrespectivelyinrighthilarlymphnodes(arrow,f).BeingclinicallystagedascIIIB,thefinalstageturnedouttosIIBwithinflammatoryreactionintherighthilar lymphnodeswhichwereremovedbymediastinoscopy,however,metastaticinvolvementintheleftonesinthefinalpathologicevaluationofthesurgicalspecimen.
Vermaetal.,14Inourstudy,agreementinT3determinationwas higherthaninT4(62%vs.50%,respectively)butwasstilllower thanT1andT2stages.AmongsT4patients,1ofthemwasfalsely classifiedascT3becauseofaseparatelesionindifferentlobeof thesamelungwasnotedintheexcisedpathologyspecimenand thiswasnotobservedbyPETscan.Intheremaining2ofsT4and 5of13ofsT3patientswhowerefalselyclassifiedascT3andcT2 respectively,thelongestdimensionofthetumorwasmeasured smallerthantheactualsizewhichmaybesecondaryto consolida-tivechangesaroundthetumorwhichwerenotregardedaspart ofmalignancy.OurresultofobservingthesuccessofcTNMinT1
andT2stagingandunreliabilityindeterminationofT3andT4 sta-tusisconcordantwiththeresultsofotherstudiesreportedinthe literature.6,7
Althoughthehighestdiagnosticaccuracyof67%seemstobe observedincIIIBstageinourstudywhichisdiscordantwiththe otherresultsreportedbefore,wethoughtthatthisfindingevolved secondarytothelownumberpatientsinsIIIBgroupwhich con-sistedonly3patients(Table2).FollowedbyclinicalIIIBstage,cIA3 tookthesecondhighestclinicalandsurgicalconcurrenceratioof 56%whichwasconcordantwiththehighagreementlevelinstage IobservedbyLopez-Encuentraetal.6
Oneof the main advantages of PET imaging is its ability of quantifyingthemetabolicactivityofthetumorwhichisunique forthismodality.Besidesusingfordifferentiatebetweenbenign andmalignant lesions,semiquantitativemeasurements arealso valuableforevaluation prognosisand assessingtheresponseto treatmentin oncologyarmamentarium. Amongthese,SUVmax, whichrepresentsthehighest voxelvaluewithintheROI, isthe mostcommonly used one becauseof its observer-independent natureandbeingavailableincommercialworkstations.However, SUVmaxcanbesubstantiallyaffectedbyimagenoise,thiscanbe eliminatedbycalculatingSUVpeak,whichwassuggestedamore robustalternativethanSUVmax.22DuanXYetal.reportedthatthe histopathologictypeandgradeoftumorwererelatedtoSUVmax inpatientswithlungcancer.23Vermaetal.reportedthatSUVmax oftheprimarytumorwasfoundasapredictorforupstaging in patientswithadenocarcinomaoflungcancerwhichmayserveas asurrogateforpreoperativenodalsamplingoflymphnodeswith equivocalFDGuptake.14Inourstudy,allofthesemiquantitative parameterscalculatedfromtheprimarytumorweresignificantly higherinsquamouscellcarcinomathanadenocarcinomawhich demonstratesthedifferenceinmetabolismaccordingtohistologic subtypeswhichwasalsoreportedbyKimetal.24Concordantwith theresultsofVermaetal.,14resultsofSUVmaxandaswellasother semiquantitativeparameters,wereallsignificantlyhigherin US patientscomparedtootherpatients.However,onthecontraryto studiessupportingSUVasarespresentativeparameteroftumor aggressiveness,SUVmaxandSUVpeakvaluescalculatedfromthe primarytumorwerenotsignificantlydifferentinpatientsbetween USandDSinourstudy.ThismaybebecauseSUVmaxshowingthe highestintensityofFDGuptakewithintheregionofinterestcannot representtotaltumoruptakefortheentiretumormass.Resultsof MTVandTLGderivedfromprimarytumorontheotherhand,were significantlyhigherinUSpatientsthanDSpatientswhichmay sup-portthehypothesisoftheirbeingbetterprognosticmeasuresfor diseaseprogressionthanSUVmaxreportedforsurgicaland nonsur-gicalpatientswithnon-smallcellcarcinomabefore.2Forpredicting malignancyinmediastinallymphnodes,theareaundercurvein ROCanalysiswasthelargestforMTVandcalculatedcut-offlevel forthisparameterwasfoundasthemostspecificonefor predict-inglymphnodemetastaseswithanacceptablesensitivityinour study.Buttheproblemofwhetherthesemiquantitativedataof onereportcanbetranslatablefromonecentertoanotherisstill unansweredandadoptingstandardizedtechniquesfor measure-mentsoftheprimarytumorandaswellofthelymphnodeshave beenrecommendedbyBryantetal.,25Wethinkthat,determining centerspecificcut-offvaluesforsemiquantitativeparametersmay helpdeterminingpostsurgicalupstagingandclarifylymphnodes harboringtumoralinvolvement.
Thelimitationsofourstudyareitsretrospectiveoriginand rel-ativelylownumberofpatientsinsubgroups.Furtherstudieswith largernumberofpatientsareneededtovalidatetheroleofMTVin predictingmedistinallymphnodemetastases.Excludingpatients withmetastasesbecauseofstudydesignalsolimitedevaluatingthe roleofFDGPET/CTinidentifyingunexpectedmetastaticdisease.
Inconclusion,clinicalstagingofTstatusismoreaccuratethan nodalstaging with FDGPET/CT in patientswithnon-small cell carcinoma.ThequantitativenatureofFDGuptakeoftheprimary tumorplayroleinpostsurgicalupstaging.VolumedependentPET parametersmaybemorevaluablethanSUVmaxinpredictingnodal involvement.Adoptingcenterspecificcut-offvaluesforMTVfor interpretationofFDGuptakesin mediastinal lymphnodesmay improvethediagnosticaccuracyofFDGPET/CTinnodal assess-mentswhichenablescorrectclinicalstaging.
Conflictofinterest
Theauthorshavenoconflictsofinteresttodeclare.
References
1.KayFU,KandathilA,BatraK,SabooSS,AbbaraS,RajiahP.RevisiontotheTumor, NodeMetastasisstagingoflungcancer(8thedition):rationale,radiologic find-ingsandclinicalimplications.WorldJRadiol.2017;9:269–79.
2.ZhangH,WroblewskiK,LiaoS,KampalathR,PenneyBC,ZhangY,etal.Prognostic valueofmetabolictumorburdenfrom18F-FDGPETinsurgicalpatienytswith
non-smallcelllungcancer.AcadRadiol.2013;20:32–40.
3.KligermanS,AbbottG.AradiologicreviewofthenewTNMclassificationsystem. AmJRoentgenol.2010;194:562–73.
4.CetinkayaE,TurnaA,YildizP,DodurgaliR,BedirhanMA,GürsesA,etal. Com-parisonofclinicalandsurgical–pathologicalstagingofpatientswithnon-small celllungcarcinoma.EurJCardiothoracSurg.2002;22:1000–5.
5.PerigaudC,BridjiB,RousselJC,SaganC,MugniotA,DuveauD,etal.Prospective preoperativemediastinallymphnodestagingbyintegratedpositronemission tomography-computerisedtomographyinpatientswithnon-smallcelllung cancer.EurJCardiothoracSurg.2009;36:731–6.
6.Lopez-EncuentraA,Garcia-LujanR,RivasJJ,Rodriguez-RodriguezJ,Torres-Lanza J,Varela-SimoG,etal.Comparisonbetweenclinicalandpathologicalstagingin 2994casesoflungcancer.AnnThoracSurg.2005;79:974–9.
7.GdeedoA,SchilPV,CorthoutsB,MieghemFV,MeerbeeckJV,MarckEV,etal. ComparisonofTNM[(i)TNM]andpathologicalTNM[pTNM]instagingof bron-chogeniccarcinoma.EurJCardiothoracSurg.1997;12:224–7.
8.CerfolioRJ,OjhaB,BryantAS,RaghuveerV,MountzJM,BartolucciAA.The accu-racyofintegratedPET-CTcomparedwithdedicatedPETaloneforthestagingof patientswithnonsmallcelllungcancer.AnnThoracSurg.2004;78:1017–23.
9.LardinoisL,WederW,HanyTF,KamelEM,KoromS,SeifertB,etal.Stagingof non-small-celllungcancerwithintegratedpositron-emissiontomographyand computedtomography.NEngJMed.2003;348:2500–7.
10.RahimMK,KimSE,SoH,KimHJ,CheonGJ,LeeES,etal.Recenttrendsin PETimageinterpertationsusingvolumetricandtexture-basedquantification methodsinnuclearoncology.NuclMedMolImaging.2014;48:1–15.
11.LeeP,BazanJG,LavoriPW,WeerasuriyaDK,QuanA,LeQT.Metabolictumor volumeisanindependentprognosticfactorinpatientstreateddefinitivelyfor non-small-celllungcancer.ClinLungCancer.2012;13:52–8.
12.LiaoS,PenneyBC,WroblewskiK,ZhangH,SimonCA,KampalathR,etal. Prog-nosticvalueofmetabolictumorburdenon18F-FDGPETinnonurgicalpatients
withnon-smallcelllungcancer.EurJNuclMedMolImaging.2012;39:27–38.
13.FernandoHC,GoldstrawP.Theaccuracyofclinicalevaluativeintrathoracic staginginlungcancerasassessedbypostsurgicalpathologicstaging.Cancer. 1990;65:2503–6.
14.VermaS,ChanJ,ChewC,SchultzC.PET-SUVmaxandupstagingoflungcancer. HeartLungCirc.2019;28:436–42.
15.BülzebruckH,BoppR,DringsP,BauerE,KrysaS,ProbstG,etal.Newaspectsin thestagingoflungcancer.Cancer.1992;70:1102–10.
16.VanTinterenH,HoekstraOS,SmitE,vandenBerghJH,SchreursAJ,Stallaert RA,etal.Effectivenessofpositronemissiontomographyinthepreoperative assessmentofpatientswithsuspectednon-smallcelllungcancer:thePLUS multicentretrial.Lancet.2002;359:1388–93.
17.WederW,SchmidRA,BruchhausH,HillingerS,SteinertHC,vonSchulthessGK, etal.Detectionofextrathoracicmetastasesbypositronemissiontomography inlungcancer.AnnThoracSurg.1998;66:86–92.
18.LinWY,HsuWH,LinKH,WangSJ.RoleofpreoperativePET-CTinassessingin earlystagelungcancer.JChinMed.2012;75:203–8.
19.Al-SarrafN,AzizR,GatelyK,LuceyJ,WilsonL,McGovernE,etal.Patternand predictorsofoccultmediastinallymphnodeinvolvementinnon-smallcelllung cancerpatientswithnegativemediastinaluptakeonpositronemission tomog-raphy.EurJCardiothoracSurg.2006;82:417–22.
20.KandathilA,KayFU,ButtYM,WachsmannJW,SubramaniamRM.RoleofFDG PET/CTintheeighteditionofTNMstagingofnon-smallcelllungcancer. Radio-graphics.2018;38:2134–49.
21.ZanzonicoP. Positronemission tomography:a reviewof basicprinciples, scannerdesign and performance, and current systems. Semin NuclMed. 2004;34:87–111.
22.PakK,KimSJ.WhatdowemeasureinOncologyPET?NuclMedMolImaging. 2017;51:212–6.
23.DuanXY,WangW,LiM,LiY,GuoYM.Predictivesignificanceof standard-izeduptakevalueparametersofFDG-PETinpatientswithnon-smallcelllung carcinoma.BrazJMedBiolRes.2015;48:267–72.
24.KimE,WuHG,KeamB,KimTM,KimDW,PaengJC,etal.Significanceof 18F-FDGPETparametersaccordingtohistologicsubtypeinthetreatmentoutcomeof stageIIInon-small–celllungcancerundergoingdefinitiveconcurrent chemora-diotherapy.ClinLungCancer.2019;20:e9–23.
25.BryantAS,CerfolioRJ,KlemmKM,OjhaB.Maximumstandarduptakevalue ofmediastinallymphnodesonintegratedFDG-PET-CTpredictspathologyin patientswithnon-smallcelllungcancer.AnnThoracSurg.2006;82:417–23.