Staphylococcus aureus can be found as a commensal on the skin and nasal flora, and may cause local, severe, and invasive infections, such as bacteremia or pneumonia (1). The anterior nostrils represent the most common area for colonization of staphylococci; in fact, longitudinal studies have shown that ~50% of individuals are S. aureus nasal carriers (2,3). Curi-ously, nasal colonization has been identified as a major risk factor for the development of community-acquired and noso-comial S. aureus infections (4,5).
The capacity of S. aureus to acquire antibiotic resistance genes is important. Methicillin-resistant S. aureus (MRSA)
isolates have been subsequently reported in hospital and community settings worldwide. The increasing prevalence of MRSA in the hospital acquired (HA-MRSA) and the com-munity acquired (CA-MRSA) is threatening. By definition, all MRSA (carrying mecA gene) species are resistant to beta-lactam antibiotics. In addition, MRSA isolates can obtain other resistance determinants. Nevertheless, nowadays, S. aureus colonizer strains are mostly methicillin-susceptible ones (MSSA) (3). Although some studies including healthy people have shown that the prevalence of S. aureus and the
Background: Staphylococus aureus can be found as a commensal on skin and nasal flora or it may cause local and invasive infections. S. aureus has a large number of virulence factors.
Aims: To investigate the methicillin resistance and frequen-cy of various virulence factors in S. aureus nasal isolates. Study Design: Descriptive study.
Methods: Nasal samples collected from university students were cultured in media. S. aureus was iden-tified by conventional methods and the Staphyloslide latex test (Becton Dickinson, Sparks, USA). Antibiotic susceptibility tests were conducted, and the methicil-lin resistance was determined. The mecA, nuc, pvl and staphylococcal toxin genes were examined by poly-merase chain reaction (PCR).
Results: S. aureus was isolated in 104 of 600 (17.3%) nasal samples. In total, 101 (97.1%) S. aureus isolates were methicillin-sensitive and the remaining 3 (2.9%)
were methicillin-resistant. Furthermore, all but five isolates carried at least one staphylococcal enterotox-in gene, with seg beenterotox-ing predomenterotox-inant. The tst and eta genes were determined in 29 (27.9%), and 3 (2.9%) isolates, respectively. None of the S. aureus isolates harbored see, etb, and pvl genes.
Conclusion: A moderate rate of S. aureus carriage and low frequency of MRSA were detected in healthy students. S.
aureus isolates had a high prevalence of staphylococcal
enterotoxin genes and the tst gene. In this study, a large number of virulence factors were examined in S. aureus nasal isolates, and the data obtained from this study can be used for monitoring the prevalence of virulence genes in
S. aureus strains isolated from nasal carriers.
Keywords: Methicillin resistance, Staphylococcus
au-reus, virulence factors
Detection of Methicillin Resistance and Various Virulence Factors in
Staphylococcus aureus Strains Isolated from Nasal Carriers
Department of Microbiology, Selçuk University Faculty of Medicine, Konya, Turkey
Hatice Türk Dağı, Duygu Fındık, Gamze Demirel, Uğur Arslan
A part of this study was presented as a poster at the 5th Eurasia Congress of Infectious Diseases, 15-18 May 2013, Tirana, Albania. Address for Correspondence: Dr. Hatice Türk Dağı, Department of Microbiology, Selçuk University Faculty of Medicine, Konya, Turkey Phone: +90 505 253 36 38 e-mail: [email protected]
Received: 08.11.2013 Accepted: 05.12.2014 • DOI: 10.5152/balkanmedj.2015.150186 Available at www.balkanmedicaljournal.org
detection of MRSA is increasing (6), in many other studies, the frequency of MRSA nasal healthy carriers is very low (7-9).
S. aureus has numerous cell-associated and secreted viru-lence factors that promote cellular adhesion, invasion, bac-terial reproduction, and a deficiency of immune responses. Some of the virulence factors include Panton-Valentine leukocidin (PVL), toxic shock syndrome toxin 1 (TSST-1), hemolysins, exfoliative toxins (ETs), and staphylococcal en-terotoxins (SEs) (10). PVL is a toxin that is usually related to complicated skin and soft tissue infections, diffuse cellu-litis, necrotizing pneumonia, and osteomyelitis (11). Several toxins such as TSST-1 and SEs belong to the superantigen (SAg) family. More than 20 SAgs have been identified in S. aureus strains, and a minimum of 80% of clinical strains harbor at least one. SEs cause staphylococcal food poison-ing, whereas TSST-1 and ETs are responsible for toxic shock syndrome (TSS) and staphylococcal scalded-skin syndrome (SSSS), respectively (12).
This study aims to investigate the methicillin resistance and rates of the TSST gene (tst), Panton-Valentine leukocidin gene (pvl), exfoliative toxin genes (eta and etb), and enterotoxin genes (sea, seb, sec, sed, see, seg, seh, sei, and sej) in S. aureus nasal isolates from healthy students in our university.
MATERIALS AND METHODS
Specimen collection and bacteriological methods
University students without any disease excluding medical school and health science students were included in the study. The students were informed about the procedure and verbal informed consents were obtained. The samples were taken from both nostrils of students using a swab. The swabs were inoculated in a tryptic soy broth and incubated at 37°C for 18-24 hours. Then, 10 μL of broth was inoculated onto Columbia agar added 5% sheep blood and mannitol salt agar (Becton Dickinson, Sparks, USA) using a sterile pipette. The media were incubated at 37°C for 18-24 hours. All colonies similar to S. aureus were identified by conventional methods (Gram staining, catalase test) and Staphyloslide latex test (Becton Dickinson, Sparks, USA). Only one of the strains isolated from both agars was included in this study.
Susceptibility tests
Antibiotic susceptibility tests were conducted, and methicil-lin resistance was detected by the Kirby-Bauer disk diffusion method as recommended by the Clinical and Laboratory Stan-dards Institute (CLSI). The D-test was carried out to detect the inducible clindamycin resistance (13). The following
antibiot-ics were tested: penicillin (10 U), oxacillin (1 μg), cefoxitin (30 μg), erythromycin (15 μg), clindamycin (2 μg), gentami-cin (10 μg), tetracycline (30 μg), ciprofloxagentami-cin (5 μg), moxi-floxacin (5 μg), trimethoprim-sulfamethoxazole (1.25-23.75 μg), linezolid (30 μg), and mupirocin (200 μg). The vanco-mycin susceptibility was investigated by an E-test strip (AB Biodisk, Solna, Sweden). S. aureus ATCC 25923 was used as a quality control strain.
Molecular methods
DNA extraction was performed with a commercial DNA isolation kit (Qiagen, Valencia, CA, USA) according to the manufacturer’s recommendations. The presence of mecA (staphylococci methicillin resistance gene), nuc (S. aureus thermonuclease gene used to confirm S. aureus), and pvl was examined by modification using multiplex polymerase chain reaction (PCR) with specific primers (14-16). The PCR reac-tion mix (50 μL) included 1 μL of DNA, 5 μL of 10X PCR buffer, 25 mM MgCl2, 10 μM dNTPs, 1 μL of each primer (50
pmol/mL) and 5U Taq DNA polymerase. For multiplex PCR, the amplification was performed under the following condi-tions: 94°C for 10 min, followed by 35 cycles of 94°C for 90 s, 49°C for 90 s, and 72°C for 90 s, with a final elongation of 72°C for 10 min. The staphylococcal toxin genes were inves-tigated by PCR as previously described (17,18). The ampli-fication was carried out in the LightCycler 2.0 thermocycler (Roche Applied Science, Germany). All PCR amplification products were separated on 2% agarose gel and visualized by staining with ethidium bromide using a UV light transillumi-nator.
The S. aureus strains ATCC 49775 (mecA negative, pvl positive) and ATCC 25923 (mecA negative, pvl positive, sea positive), and N315 (mecA positive, tst positive) were used as control strains for PCR.
RESULTS
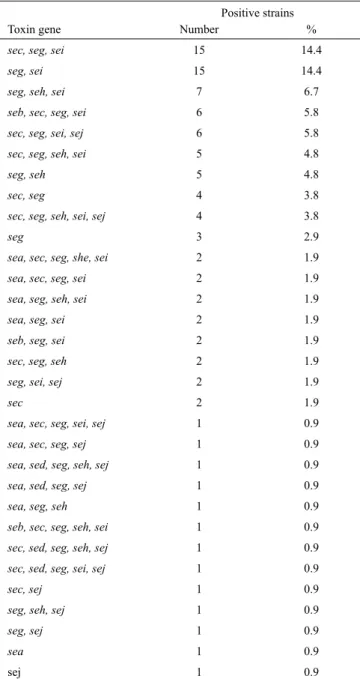
S. aureus was isolated in 104 of the 600 (17.3%) nasal sam-ples assessed. All isolates were found to be nuc-positive. Of these, 101 isolates (97.1%) were MSSA, and the remaining 3 isolates (2.9%) were MRSA according to both PCR and anti-biotic susceptibility tests results. The rate of MRSA carriage was 0.5%. Except for five of the isolates, all others (95.2%) were positive for at least one staphylococcal enterotoxin gene. The seg gene was detected in 93 (89.4%) isolates, followed by sei in 68 (65.4%), sec in 55 (52.9%), seh in 37 (35.6%), sej in 23 (22.1%), sea in 14 (13.5%), seb in 9 (8.7%) and sed in 5 (4.8%). The tst and eta genes were determined in 29 (27.9%) and 3 (2.9%) isolates, respectively. None of the S. aureus
iso-lates harbored see, etb, and pvl genes. In this study, the most common combination was determined to be seg plus sei and seg plus sec in 65.4% and 49% of all isolates, respectively. Only 7 isolates encoded a single gene (Table 1).
All S. aureus strains were susceptible to vancomycin, tri-methoprim/sulfamethoxazole, and linezolid. The suscepti-bilities of S. aureus strains for other antibiotics were 98% for gentamicin, ciprofloxacin, and moxifloxacin, 96% for tetracycline and mupirocin, 88% for erythromycin, and 20% for penicillin. The prevalence of inducible clindamycin re-sistance was 3%.
DISCUSSION
S. aureus is a major human pathogen with a high virulence that causes both hospital-acquired and community-acquired staphylococcal infections. S. aureus causes skin and soft tissue infections of varying severity, from uncomplicated abscesses to life-threatening infections such as bacteremia and sepsis. S. aureus nasal carriage has been considered as a risk factor for the occurrence of human infections (19). In some studies, the S. aureus nasal carriage was detected at a frequency as high as 30% (3,20). In a study from Turkey, the carriage rate of S. aureus in Turkish elementary school children was 24.7% (21). The rate of these bacteria differs according to the popula-tion surveyed. We investigated the carriage of S. aureus in uni-versity students, representing young adults. Medical school and health science students were excluded because they are in contact with patients. A moderate rate of S. aureus nasal car-riage (17.3%) has been detected in healthy university students. The treatment of MRSA infections is becoming increasingly difficult because MRSA strains are resistant to beta-lactam an-tibiotics, and can acquire other resistance determinants. Espe-cially in the community, the frequency of infections caused by MRSA has increased in the last decade (22). It is believed that the prevalence of MRSA carriage increases in a healthy com-munity and, therefore, the surveillance of MSSA and MRSA in the nasal carriage has been investigated in healthy individu-als. The rates determined in other studies that analyzed healthy adult and children were usually less than 1% (7,21,23). In ac-cordance with previous studies, the prevalence of MRSA na-sal carriers is very low (0.5%) in our study.
The capacity of S. aureus antibiotic resistance is also impor-tant. In this study, all strains were susceptible to trimethoprim-sulfamethoxazole, vancomycin, and linezolid. The suscepti-bilities of S. aureus strains for other antibiotics were 98% for gentamicin, ciprofloxacin and levofloxacin, 96% for tetra-cycline and mupirocin, 88% for erythromycin, and 20% for penicillin. The prevalence of inducible clindamycin resistance was 3%. The higher resistance to erythromycin could be clari-fied by the common use of macrolides in empirical treatment. S. aureus is a pathogen with a wide range of virulence fac-tors. The severity of S. aureus infections may be related to the production of some of these toxins. Exotoxins provide tis-sue destruction and escape from the host immune response. Toxins such as α-hemolysin or PVL cause cytolysis of leuko-cytes and erythroleuko-cytes (24). PVL is a virulence marker that is often identified in CA-MRSA strains associated with necro-tizing pneumonia and severe skin and soft tissue infections. The lukS-lukF genes encoding the PVL toxin are located in a phage, and can be transferred among S. aureus (25). The stud-ies conducted in our country have revealed that PVL is spread Positive strains
Toxin gene Number %
sec, seg, sei 15 14.4
seg, sei 15 14.4
seg, seh, sei 7 6.7
seb, sec, seg, sei 6 5.8 sec, seg, sei, sej 6 5.8 sec, seg, seh, sei 5 4.8
seg, seh 5 4.8
sec, seg 4 3.8
sec, seg, seh, sei, sej 4 3.8
seg 3 2.9
sea, sec, seg, she, sei 2 1.9 sea, sec, seg, sei 2 1.9 sea, seg, seh, sei 2 1.9 sea, seg, sei 2 1.9
seb, seg, sei 2 1.9
sec, seg, seh 2 1.9
seg, sei, sej 2 1.9
sec 2 1.9
sea, sec, seg, sei, sej 1 0.9 sea, sec, seg, sej 1 0.9 sea, sed, seg, seh, sej 1 0.9 sea, sed, seg, sej 1 0.9 sea, seg, seh 1 0.9
seb, sec, seg, seh, sei 1 0.9 sec, sed, seg, seh, sej 1 0.9 sec, sed, seg, sei, sej 1 0.9
sec, sej 1 0.9
seg, seh, sej 1 0.9
seg, sej 1 0.9
sea 1 0.9
sej 1 0.9
TABLE 1. The enterotoxin genes and combinations detected in the 104 S. aureus strains
at different rates between MSSA, CA-MRSA and HA-MRSA isolates without discrimination (26). All S. aureus strains were pvl-negative in our study. It was interpreted that these strains had been isolated from the carriers and not infectious agents.
Superantigens activate T-lymphocytes and macrophages lead to the extreme release of inflammatory cytokines, result-ing in septic shock. At least 20 serologically distinct staphy-lococcal superantigens have been described, including SEs A through V and TSST-1. These bacterial toxins are pyrogenic and related to food poisoning and TSS. SEA and SED are the first and second most common staphylococcal toxins as-sociated with food poisoning worldwide (27). According to these data, SEA was the most common toxin (40.1%) in hos-pital- and community-acquired S. aureus isolates in a study from Turkey (28). In the present study, the seg gene was the most common (89.4%). In relation to the standard enterotoxin genes, the sec gene (52.9%) was found to be the most frequent gene, followed by sea (13.5%). None of the S. aureus isolates harbored see. It was only determined in less than 1% of the samples in various studies (29-31).
Enterotoxigenic S. aureus strains with a combination of dif-ferent SE genes can also promote the incidence and severity of S. aureus infections. In this study, the most common com-binations detected were seg plus sei and seg plus sec in 65.4% and 49% of all isolates, respectively. Only 7 isolates encoded a single gene.
S. aureus isolates producing TSST-1 has been most com-monly isolated from patients with important clinical symp-toms. The tst gene encoding the TSST-1 was detected in 29 (27.9%) isolates in our study at similar rates to another study including healthy people (32).
S. aureus strains harboring ETs can cause SSSS and im-petigo. Although there are differences in the prevalence between countries, approximately 5% of S. aureus human isolates produce ETs (25,29). However, these genes showed significantly higher rates in nasal and clinical MSSA strains in the study (30). In our study, 3 (2.9%) strains carried the eta gene, encoding the exfoliative toxin A; however, all iso-lated S. aureus strains were negative for the exfoliative toxin B gene. In a study conducted in our country, these genes were not detected in healthy controls but etb was determined in 18 (58.1%) patients with psoriasis, suggesting a potential relationship (33).
In conclusion, a moderate rate of S. aureus carriage and very low frequency of MRSA were detected in healthy students. S. aureus nasal isolates showed a very high prevalence of staph-ylococcal enterotoxin genes and the tst gene. Most S. aureus isolates were susceptible to antimicrobial agents. In this study, a large number of virulence factors were examined in S. au-reus nasal isolates, and the data obtained from this study can
be used for monitoring the prevalence of virulence genes in S. aureus strains isolated from nasal carriers.
Ethics Committee Approval: Ethics committee approval was
re-ceived for this study from the ethics committee of Selçuk University Faculty of Medicine.
Informed Consent: The students were informed about the
proce-dure and verbal informed consents were obtained.
Peer-review: Externally peer-reviewed.
Author contributions: Concept - H.T.D., U.A.; Design - H.T.D.,
U.A. ; Supervision - D.F., H.T.D.; Resource - T.M., M.D.; Materi-als - G.D.; Data Collection &/or Processing - G.D.; Analysis &/or Interpretation - H.T.D., U.A., D.F.; Literature Search - H.T.D.; Writ-ing - H.T.D., D.F.; Critical Reviews - H.T.D., U.A., D.F.
Acknowledgements: We thank to Meral Demirayak for her
con-tributions.
Conflict of Interest: No conflict of interest was declared by the
authors.
Financial Disclosure: This study was financially supported by
Tales medical. The sponsor played no role in the study.
REFERENCES
1. Miller LG, Perdreau-Remington F, Rieg G, Mehdi S, Perlroth J, Bayer AS, et al. Necrotizing fasciitis caused by community-associated methicillin-resistant Staphylococcus aureus in Los Angeles. N Engl J Med 2005;352:1445-53. [CrossRef]
2. Wertheim HF, Melles DC, Vos MC, van Leeuwen W, van Belkum A, Verbrugh HA, et al. The role of nasal carriage in Staphylococcus aureus infections. Lancet Infect Dis 2005;5:751-62. [CrossRef]
3. van Belkum A, Verkaik NJ, de Vogel CP, Boelens HA, Verveer J, Nouwen JL, et al. Reclassification of Staphylococcus aureus nasal carriage types. J Infect Dis 2009;199:1820-6. [CrossRef]
4. von Eiff C, Becker K, Machka K, Stammer H, Peters G. Nasal carriage as a source of Staphylococcus aureus bacteremia. Study Group. N Engl J Med 2001;344:11-6. [CrossRef]
5. Rebollo-Perez J, Ordonez-Tapia S, Herazo-Herazo C, Reyes-Ramos N. Nasal carriage of Panton Valentine leukocidin-pos-itive methicillin-resistant Staphylococcus aureus in healthy preschool children. Rev Salud Publica (Bogota) 2011;13:824-32. [CrossRef]
6. Bloomfield SF, Cookson BD, Falkiner FR, Griffith C, Cleary V. Methicillin-resistant Staphylococcus aureus, Clostridium diffi-cile, and extended-spectrum β-lactamase-producing Escherichia coli in the community: assessing the problem and controlling the spread. Am J Infect Control 2007;35:86-8. [CrossRef]
7. Sakwinska O, Kuhn G, Balmelli C, Francioli P, Giddey M, Perreten V, et al. Genetic diversity and ecological success of
colonizing Staphylococcus aureus. Appl Environ Microbiol 2009;75:175-83. [CrossRef]
8. Mertz D, Frei R, Periat N, Zimmerli M, Battegay M, Flückiger U, et al. Exclusive Staphylococcus aureus throat carriage: at-risk populations. Arch Intern Med 2009;169:172-8. [CrossRef]
9. Ben Slama K, Gharsa H, Klibi N, Jouini A, Lozano C, Gómez-Sanz E, et al. Nasal carriage of Staphylococcus aureus in healthy humans with different levels of contact with animals in Tunisia: genetic lineages, methicillin resistance, and virulence factors.
Eur J Clin Microbiol Infect Dis 2011;30:499-508. [CrossRef]
10. Jarraud S, Mougel C, Thioulouse J, Lina G, Meugnier H, Forey F, et al. Relationships between Staphylococcus aureus genetic background, virulence factors, agr groups (alleles), and human disease. Infect Immun 2002;70:631-41. [CrossRef]
11. Nhan TX, Leclercq R, Cattoir V. Prevalence of toxin genes in con-secutive clinical isolates of Staphylococcus aureus and clinical im-pact. Eur J Clin Microbiol Infect Dis 2011;30:719-25. [CrossRef]
12. Xu SX, McCormick JK. Staphylococcal superantigens in col-onization and disease. Front Cell Infect Microbiol 2012;2:52.
[CrossRef]
13. Clinical and Laboratory Standards Institute (CLSI). 2011. Per-formance standards for antimicrobial susceptibility testing. Twenty-first informational supplement, M100-S21, National Committee for Clinical Laboratory Standards, Wayne PA. 14. Oliveira DC, De Lencastre H. Multiplex PCR strategy for rapid
identification of structural types and variants of the mec ele-ment in methicillin-resistant Staphylococcus aureus. Antimicrob
Agents Chemother 2002;46:2155-61. [CrossRef]
15. Kim CH, Khan M, Morin DE, Hurley WL, Tripathy DN, Kehrli Jr M, et al. Optimization of the PCR for detection of Staphylo-coccus aureus nuc gene in bovine milk. J Dairy Sci 2001;84:74-83. [CrossRef]
16. Lina G, Piemont Y, Godail-Gamot F, Bes M, Peter MO, Gaud-uchon V, et al. Involvement of Panton-Valentine leukocidin-producing Staphylococcus aureus in primary skin infections and pneumonia. Clin Infect Dis 1999;29:1128-32. [CrossRef]
17. Monday SR, Bohach, GA. Use of multiplex PCR to detect clas-sical and newly described pyrogenic toxin genes in staphylococ-cal isolates. J Clin Microbiol 1999;37:3411-4.
18. Sila J, Sauer P, Kolar M. Comparison of the prevalence of genes coding for enterotoxins, exfoliatins, Panton-Valentine leukoci-din and tsst-1 between methicillin-resistant and methicillin-sus-ceptible isolates of Staphylococcus aureus at the university hos-pital in Olomouc. Biomed Pap Med Fac Univ Palacky Olomouc
Czech Repub 2009;153:215-8. [CrossRef]
19. Manious AG, Hueston WJ, Everett CJ, Diaz VA. Nasal carriage of Staphylococcus aureus and methicillin-resistant S. aureus in the Unit-ed States, 2001-2002. Ann Fam MUnit-ed 2006;4:132-7. [CrossRef]
20. Zanelli G, Sansoni A, Zanchi A, Cresti S, Pollini S, Rossolini GM, et al. Staphylococcus aureus nasal carriage in the community: A survey from central Italy. Epidemiol Infect 2002;129:417-20.
[CrossRef]
21. Kiliç A, Mert G, Senses Z, Bedir O, Aydogan H, Basustaoglu AC, Appelbaum PC. Molecular characterization of
methicil-lin resistant Staphylococcus aureus nasal isolates from Turkey.
Antonie Van Leeuwenhoek 2008;94:615-9. [CrossRef]
22. Adhikari RP, Ajao AO, Aman MJ, Karauzum H, Sarwar J, Lydecker AD, et al. Lower antibody levels to Staphylococ-cus aureus exotoxins are associated with sepsis in hospital-ized adults with invasive S. aureus infections. J Infect Dis 2012;206:915-23. [CrossRef]
23. Dinic M, Vukovic S, Kocic B, Stankovic Dordevic D, Bogdanovic M. Nasal carriage of Staphylococcus aureus in healthy adults and in school children. Acta Fac Med Naiss 2013;30:31-6.
24. DeLeo FR, Diep BA, Otto M. Host defense and pathogenesis in Staphylococcus aureus infections. Infect Dis Clin North Am 2009;23:17-34. [CrossRef]
25. Lozano C, Gomez-Sanz E, Benito D, Aspiroz C, Zarazaga M, Torres C. Staphylococcus aureus nasal carriage, virulence traits, antibiotic resistance mechanisms, and genetic lineages in healthy humans in Spain, with detection of CC398 and CC97 strains. Int J Med Microbiol 2011;301:500-5. [CrossRef]
26. Duman Y, Tekeroğlu MS, Otlu B. Investigation of the Presence of Panton-Valentine Leukocidin and Clonal Relationship of Community- and Hospital-Acquired Clinical Isolates of Staphy-lococcus aureus. Mikrobiyol Bul 2013;47:389-400. [CrossRef]
27. Pinchuk IV, Beswick EJ, Reyes VE. Staphylococcal enterotox-ins. Toxins (Basel) 2010;2:2177-97. [CrossRef]
28. Yılmaz S, Kılıç A, Karagöz A, Bedir O, Uskudar Guclu A, Başustaoglu AC. Investigation of various virulence factors among the hospital and community-acquired Staphylococ-cus aureus isolates by real-time PCR method. Mikrobiyol Bul 2012;46:532-45.
29. Becker K, Friedrich AW, Lubritz G, Weilert M, Peters G, Von Eiff C. Prevalence of genes encoding pyrogenic toxin superanti-gens and exfoliative toxins among strains of Staphylococcus au-reus isolated from blood and nasal specimens. J Clin Microbiol 2003;41:1434-9. [CrossRef]
30. Shukla SK, Karow ME, Brady JM, Stemper ME, Kislow J, Moore N, et al. Virulence genes and genotypic associations in nasal carriage, community-associated methicillin susceptible and methicillin-resistant USA400 Staphylococcus aureus iso-lates. J Clin Microbiol 2010;48:3582-92. [CrossRef]
31. Schaumburg F, Ateba Ngoa U, Kösters K, Köck R, Adegnika AA, Kremsner PG. Virulence factors and genotypes of Staphy-lococcus aureus from infection and carriage in Gabon. Clin
Mi-crobiol Infect 2011;17:1507-13. [CrossRef]
32. Megevand C, Gervaix A, Heininger U, Berger C, Aebi C, Vau-daux B, et al. Molecular epidemiology of the nasal colonization by methicillin-susceptible Staphylococcus aureus in Swiss chil-dren. Clin Microbiol Infect 2010;16:1414-20. [CrossRef]
33. Balci DD, Duran N, Ozer B, Gunesacar R, Onlen Y, Yenin JZ. High prevalence of Staphylococcus aureus cultivation and supe-rantigen production in patients with psoriasis. Eur J Dermatol 2009;19:238-42.