Mediterranean region and Middle East. Cur-rent estimates of the prevalence of gastroin-testinal involvement in patients with Behçet disease vary between 1.4% and 60% [3–7]. The intestinal lesions occur in two forms: small-vessel disease with mucosal inflam-mation and large-vessel disease resulting in ischemia and infarction [11, 12]. Histopatho-logic analysis of the bowel wall reveals evi-dence of perivasculitis with lymphocytic in-filtration, lymphocytic vasculitis of the small veins and venules, and large cavitating ul-cers. A nonspecific chronic inflammatory re-action is found in the ulcer and directly ad-jacent mucosa, and the rest of the mucosa is normal [10, 11].
The diagnosis of Behçet disease is based on collective information gained from clini-cal, laboratory, histologic, and imaging data that must be interpreted correctly. The diag-nosis of intestinal Behçet disease is made if the patient has both bowel ulcerations and
Intestinal Behçet Disease:
Evaluation With MR Enterography—
A Case-Control Study
Elif Peker
1Ayşe Erden
1İlhan Erden
1Nurşen Düzgün
2,3Peker E, Erden A, Erden İ, Düzgün N
1Department of Radiology, Ankara University, School of Medicine, Talatpaşa Bulvarı, Sıhhiye, 06100, Ankara, Turkey. Address correspondence to A. Erden ([email protected]).
2Department of Internal Medicine–Rheumatology, School of Medicine, Ankara University, Ankara, Turkey. 3Present address: Department of Internal Medicine-Rheumatology, School of Medicine, Ufuk University, Ankara, Turkey.
AJR 2018; 211:767–775 0361–803X/18/2114–767 © American Roentgen Ray Society
B
ehçet disease is a rare, recurrent, multisystemic form of vasculitis first described by the Turkish der-matologist Hulusi Behçet in 1937 as a syndrome consisting of oral aphthous ul-cers, genital ulcerations, and ocular inflamma-tion [1, 2]. Besides the original triple-symptom complex, other important manifestations may include skin lesions, gastrointestinal ulcer-ations, neurologic involvement, vascular aneu-rysms, thrombosis, and arthritis [3–10]. The disease runs a chronic course with unpredict-able exacerbations and remissions, which can cause complete debilitation. The underlying cause of Behçet disease is still unknown, but current evidence favors a multifactorial cause with an immunologic basis.One of the important and rare manifes-tations of Behçet disease is intestinal ulcer-ations. Symptomatic or documented intesti-nal involvement is common among patients in eastern Asia, but it is rare in patients in the Keywords: Behçet disease, MR enterography
doi.org/10.2214/AJR.17.19174
Received October 14, 2017; accepted after revision February 16, 2018.
OBJECTIVE. The purposes of this study were to discern imaging findings that distin-guish Behçet disease from small-bowel Crohn disease, to find initial performance estimates for these findings, and to evaluate the diagnostic value of MR enterography (MRE) for detect-ing intestinal Behçet disease.
MATERIALS AND METHODS. The MRE examinations of 30 consecutively registered patients with established intestinal Behçet disease were reviewed by two blinded readers. The frequencies of MRE findings were compared with those obtained for 30 control subjects with small-bowel Crohn disease who were matched for sex and age. The performance estimates were generated with ileocolonoscopic and histopathologic findings as the reference standard.
RESULTS. Polypoid pattern and homogeneous mural enhancement were the findings seen more frequently in Behçet disease (p = 0.000) than in Crohn disease (p = 0.003). Stric-ture formation, long-segment disease, and involvement of more proximal ileal segments fa-vored small-bowel Crohn disease. The ROC AUCs for polypoid pattern and homogeneous mural enhancement in the detection of intestinal Behçet disease were 0.806 and 0.779. The accuracy of MRE was 70.00% (95% CI, 50.60–85.27%); sensitivity, 57.14% (95% CI, 34.02– 78.18%), and specificity, 100% (95% CI, 66.37–100%).
CONCLUSION. MRE has potential for use as a radiation-free alternative for clarifying the cause of nonspecific gastrointestinal symptoms in patients with known Behçet disease. However, additional studies are needed to determine the actual value of MRE in patients with Behçet disease and to validate the clinical usefulness of the technique in the detection of un-known intestinal Behçet disease.
Peker et al.
MR Enterography of Behçet Disease Gastrointestinal Imaging Original Research
clinical manifestations that meet the diag-nostic criteria of either the International Study Group for Behçet Disease [13] or the Behçet Disease Research Committee of Ja-pan [14]. Using these previously established criteria for the diagnosis of systemic Behçet disease is not necessarily inclusionary of in-testinal Behçet disease, because various ex-traintestinal manifestations emerge at differ-ent times throughout the disease course. In 2009, Cheon et al. [15] proposed novel diag-nostic criteria that may be particularly use-ful to patients with ileocolonic ulcers whose condition does not fully satisfy the diagnos-tic criteria for systemic Behçet disease.
The diagnosis of intestinal Behçet disease remains difficult for several reasons. Be-cause it is a rare disease, even in countries where it is prevalent, it is not considered in the main differential diagnosis of abdominal complaints. When its symptoms are mild, intestinal Behçet disease can be overlooked and even be recognized after many years. Furthermore, intestinal lesions may be pres-ent in patipres-ents who do not have symptoms. Because of similar clinical presentations, the disease can be confused with Crohn disease, which is much more commonly encountered in clinical practice. In the absence of extrain-testinal manifestations, it may be impossi-ble to differentiate intestinal Behçet disease from Crohn disease [16–18].
Cross-sectional imaging techniques such as CT and MRI yield valuable information about transmural and extraintestinal changes [19–22]. In this regard, in 2014 it was report-ed that approximately one-fourth of patients with intestinal Behçet disease were exposed to potentially harmful levels of diagnostic ra-diation from CT examinations. Thus, it has been proposed that clinicians should reduce the number of unnecessary CT examinations and consider an alternative modality, such as MR enterography (MRE) [23]. Current-ly there are onCurrent-ly scarce data on the useful-ness of MRE for the evaluation of intestinal Behçet disease [18, 24]. The purposes of our study were to determine imaging findings that differentiate Behçet disease from small-bowel Crohn disease, to discern initial per-formance estimates for these findings, and to evaluate the diagnostic value of MRE for de-tecting intestinal Behçet disease.
Materials and Methods
The institutional review board approved this retrospective observational study and waived the requirement for informed consent.
Study Population
The study population was derived from eligible patients who were known to have intestinal Behçet disease or patients with Behçet disease with sus-pected intestinal involvement who needed MR en-terographic investigation of the small intestine to assess the extent of disease, to detect evidence of postoperative recurrence, or to detect enteric com-plications. These subjects were enrolled in the study from April 2012 to August 2017. Matched control subjects were patients with an established diagnosis of Crohn disease who underwent MRE at the same institution during the same period.
The inclusion criteria were presence of a definite diagnosis of Behçet disease and histopathologic re-sults obtained by ileocolonoscopy. The diagnosis of Behçet disease was made according to criteria based on the clinical findings specified by the In-ternational Study Group for Behçet’s Disease [13]. Eligible patients were at least 18 years old, had con-firmed intestinal Behçet disease, or had suspected intestinal involvement of Behçet disease. Exclusion criteria were any contraindication to MRI, inabil-ity to receive gadolinium chelate compounds (al-lergy, renal insufficiency), claustrophobia, subopti-mal image quality (motion artifacts on images of patients who were unable to suspend respiration during 3D fat-suppressed contrast-enhanced gradi-ent-echo T1-weighted imaging), inadequate bowel distention, and the presence of surgical clips or a hip prosthesis, which can cause extensive artifacts. No eligible patient was excluded from the study on the basis of these exclusion criteria.
After initial identification of a patient’s eligibil-ity for the study, the institution’s electronic med-ical records (radiology, ileocolonoscopy, patholo-gy, and discharge summary) for each patient were reviewed to document demographic and clinical characteristics. In each case, the following data were collected: age at MRE; sex; family history; duration from the first diagnosis of Behçet disease; pathergy test (hypersensitivity reaction of the skin to a needle prick [16]) results (if available); C-re-active protein (CRP) level; erythrocyte sedimen-tation rate (ESR); and presence and character of recurrent oral aphthous ulcerations, ocular mani-festations (uveitis, retinal vasculitis), genital ulcer-ation, recurrent thrombophlebitis, arthralgia or ar-thritis, cutaneous lesions (papulopustular eruption, pseudofolliculitis, erythema nodosum), neurolog-ic symptoms (encephalitis, peripheral neuropathy, hemiparesis, depression), disease of central and pe-ripheral arteries (manifesting as aneurysms or oc-clusions), and location of enteric involvement.
A total of 30 patients with Behçet disease were enrolled in the study. Cases were matched manual-ly to those of 30 patients with Crohn disease of the same sex, who were the control subjects. To meet
our matching objective, we accepted an age dif-ference up to 3 years between case and control pa-tients. Matching was done randomly from a list of patients with Crohn disease; their clinical and im-aging findings were not known. Patients with Crohn disease were chosen as control subjects not only be-cause of the similarities between Crohn disease and Behçet disease but also because of the accessibility of all types of medical records and reports of MR enterographic examinations of the patients. MR Enterographic Technique
The patients were asked to fast after midnight on the day before the examination. An enteric con-trast agent composed of 1500 mL drinking water and 125 mL of lactulose solution was adminis-tered orally to achieve small-bowel distention. Pa-tients were instructed to drink this solution dur-ing the 60 minutes before undergodur-ing MRE. To ensure consistent bowel distention, the patients consumed approximately 550-mL aliquots of the solution every 20 minutes (a total of three doses) before image acquisition. Just before entering the MRI unit, the patients were asked to drink an ad-ditional 500 mL of water for distention of the duo-denum and proximal jejunum. At the beginning of the examination, immediately after cine imaging, patients were given 0.5 mg of glucagon IV to re-duce motion artifacts arising from bowel peristal-sis. A second 0.5-mg IV dose was injected imme-diately before performance of a 3D fat-suppressed contrast-enhanced gradient-echo T1-weighted se-quence, which is the most likely to be affected by motion artifacts.
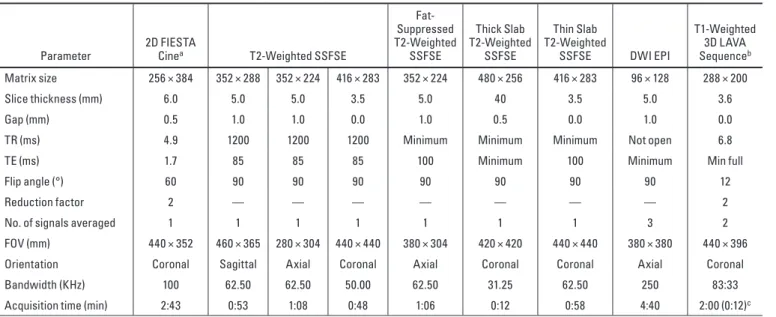
MRE was performed with a 1.5-T system (Op-tima 450w, GE Healthcare). Acquisition was per-formed with a 12-channel torso array coil with the patient in the prone position. The following pro-tocol was used for assessment of the small bowel: cine imaging with 2D balanced steady-state free precession; sagittal, coronal, and axial single-shot fast spin-echo (SSFSE) imaging; axial fat-sup-pressed fast spin-echo imaging; coronal heavily T2-weighted thick slab SSFSE imaging; and cor-onal heavily T2-weighted thin slices. DW images with b values of 0 and 600 s/mm2 were obtained in the axial plane by use of a single-shot multislice echo-planar imaging sequence. After IV adminis-tration of 0.2 mL/kg of gadolinium chelate at an in-jection rate of 2–3 mL/s, dynamic imaging, includ-ing unenhanced, arterial, enteric (45–50 seconds after initiation of contrast injection), and equilib-rium phases, was performed in the coronal plane with a 3D fat-suppressed gradient-echo T1-weight-ed (LAVA-flex, GE Healthcare) sequence. The table time for MRE was approximately 35–40 minutes. The pulse sequence parameters used in our study are listed in detail in Table 1.
Endoscopy
All ileocolonoscopy examinations were per-formed in a clinical setting by a gastroenterologist using the standard technique. Each ileocolonos-copy procedure was performed as a part of rou-tine clinical practice. The endoscopist knew that the indication for the procedure was inflammatory bowel disease. The terminal ileum was intubated, and mucosal biopsy samples were obtained for all patients. Ileocolonoscopic and MRE examinations were performed within 2 weeks of each other. MRI Data Analysis
All MRE studies were reviewed by two experi-enced radiologists who were unaware of the clini-cal, surgiclini-cal, and laboratory data. The following imaging findings were evaluated: intestinal wall thickness (≥ 3 mm was considered abnormal), pat-tern of wall thickening (smooth or polypoid), patpat-tern of mural hyperenhancement (homogeneous or lay-ered), degree of wall enhancement in enteric phase, scored as mild or marked, compared with enhance-ment of adjacent normal bowel, mural edema (high or intermediate wall signal intensity on T2-weighted images), ulcerations (irregularity and deep depres-sions at mucosal surface), comb sign, mesenteric lymph node enlargement, fibrofatty proliferation, perienteric inflammation (mesenteric heterogene-ity, edema, nestlike or serpentine hypervascularheterogene-ity, spiculations, or enhancement adjacent to the serosal surface of the small bowel), perienteric free fluid, cecal deformity (changes in size or shape of cecum
as contraction or distortion), ileocecal valve in-volvement (thickened, deformed), and the presence of penetrating disease (sinus, fistula, abscess). Stric-ture was diagnosed in the presence of proximally dilated small-bowel loops (diameter > 2.5 cm from outer wall to outer wall). The length and location of abnormal segments were also noted.
Statistical Analysis
Descriptive statistics were used to summarize all study variables of interest. The imaging find-ings listed in MRI Data Analysis evaluated for frequency for all 60 patients (30 with Behçet dis-ease, 30 with Crohn disease) were selected with-out use of reference standards. For categoric vari-ables, counts and percentages were reported. For continuous variables, mean ± SD were reported when the values had approximately normal distri-bution. A chi-square or Fisher exact test was used to compare categoric variables. The significance level was set at p < 0.05.
The levels of interobserver agreement were as-sessed with kappa statistics. Kappa values less than 0.20 indicated slight agreement; 0.21–0.40, fair agreement; 0.41–0.60, moderate agreement; 0.61–0.80, substantial agreement; and 0.81–0.99, excellent agreement between the observers.
The performance estimates were generated with ileocolonoscopic and histopathologic find-ings as standards of reference. The estimated val-ues were calculated for imaging findings that were significantly associated with Behçet disease.
Out of all imaging findings, polypoid pat-tern and homogeneous mural enhancement were significantly associated with Behçet disease. The performance estimates were determined for these findings. ROC analysis was performed for polyp-oid pattern and homogeneous mural enhancement to evaluate the utility of each parameter in identi-fying Behçet disease. Spearman rank correlation coefficient was used to evaluate the associations of parameters used for discrimination of intestinal Behçet disease and Crohn disease.
Performance estimates of MRE technique were also determined. They were analyzed only for the 30-patient Behcet population for presence or absence of all MRI findings. Accuracy, sensitiv-ity, specificsensitiv-ity, and positive and negative predic-tive values with corresponding 95% CIs for MRE in the detection of intestinal Behçet disease were calculated with MedCalc software (version 16, MedCalc Software).
Results
Demographics of Case and Control Population Thirty patients with Behçet disease (16 men [mean age, 43.7 ± 10.9 years; range, 24– 62 years], 14 women [mean age, 36.0 ± 8.8 years; range, 19–50 years]; mean age, 40.1 ± 10.1 years; range, 19–62 years) were recruit-ed into this study. The control group consist-ed of 30 patients with Crohn disease (16 men [mean age, 44.9 ± 11.2 years; range, 27–65 years], 14 women [mean age, 37.0 ± 9.2 years; TABLE 1: MRI Pulse Sequence Parameters Used in Study
Parameter 2D FIESTA Cinea T2-Weighted SSFSE
Fat- Suppressed T2-Weighted SSFSE Thick Slab T2-Weighted SSFSE Thin Slab T2-Weighted
SSFSE DWI EPI
T1-Weighted 3D LAVA Sequenceb Matrix size 256 × 384 352 × 288 352 × 224 416 × 283 352 × 224 480 × 256 416 × 283 96 × 128 288 × 200 Slice thickness (mm) 6.0 5.0 5.0 3.5 5.0 40 3.5 5.0 3.6 Gap (mm) 0.5 1.0 1.0 0.0 1.0 0.5 0.0 1.0 0.0
TR (ms) 4.9 1200 1200 1200 Minimum Minimum Minimum Not open 6.8
TE (ms) 1.7 85 85 85 100 Minimum 100 Minimum Min full
Flip angle (°) 60 90 90 90 90 90 90 90 12
Reduction factor 2 — — — — — — — 2
No. of signals averaged 1 1 1 1 1 1 1 3 2
FOV (mm) 440 × 352 460 × 365 280 × 304 440 × 440 380 × 304 420 × 420 440 × 440 380 × 380 440 × 396
Orientation Coronal Sagittal Axial Coronal Axial Coronal Coronal Axial Coronal
Bandwidth (KHz) 100 62.50 62.50 50.00 62.50 31.25 62.50 250 83:33
Acquisition time (min) 2:43 0:53 1:08 0:48 1:06 0:12 0:58 4:40 2:00 (0:12)c
Note—Dash (—) indicates acquisitions without parallel imaging. FIESTA = fast imaging employing steady-state acquisition, SSFSE = single-shot fast spin-echo, EPI = echo-planar imaging, LAVA = liver imaging with volume acceleration-flexible, Min full = minimum achievable TE with full echo acquisition.
aCine imaging consisted of a 2D balanced steady-state free precision sequence. bLava Flex, GE Healthcare.
cValue in parentheses isbreath-hold time for each phase of dynamic acquisition.
range, 17–51 years]; mean age, 41.2 ± 10.9 years; range, 17–65 years). The patients and control subjects were similar with respect to age (p = 0.685) and sex (p = 1.000).
Clinical Features of Patients With Behçet Disease
The duration of systemic Behçet disease ranged from 2 to 30 years (median, 10 years). The median duration between the onset of intestinal symptoms and MRE was 4 years (range, 2.5 months–10 years). Abdominal pain was the most predominant gastrointesti-nal symptom (27/30 patients [90%]). The oth-er symptoms woth-ere diarrhea (n = 9/30 [30%]), nausea and vomiting (n = 6/30 [20%]), anorex-ia (3/30 [10%]), and gastrointestinal bleeding (1/30 [3%]). The frequency of extraintestinal
manifestations, as observed in our series of pa-tients with the diagnosis of intestinal Behçet dis-ease examined with MRE in our department is shown in Table 2. Oral aphthous ulcers were the most common symptom in 100% of our patients. Interestingly, it was followed by joint manifestations (78%). ESR was nor-mal in 75% of patients. Mean ESR was 15.2 ± 9.2 mm/h (range, 2–43 mm/h). CRP level was normal in 95% of patients (5.4 ± 12.8 mg/L; range, 0–53.9 mg/L). Pathergy test results were available for 50% of patients and were positive in 80% (12/15) of cases.
Features of Group With Intestinal Behçet Disease and Positive MR Enterographic Findings
Nine of 30 patients with symptoms previ-ously diagnosed as intestinal Behçet disease
had normal findings at MRE, ileocolonosco-py, and biopsy. Nine patients had abnormal findings at both ileocolonoscopy and biopsy but normal findings at MRE. Among 30 pa-tients with an established diagnosis of intesti-nal Behçet disease, 12 (nine men, three wom-en) had abnormal results of all diagnostic procedures (MRE, ileocolonoscopy, and bi-opsy). On the other hand, 29 (15 men, 14 wom-en) of 30 patients with Crohn disease had ab-normal findings of all diagnostic procedures (only one patient had normal MRE findings). The mean age of patients with MRE-positive intestinal Behçet disease was 40.5 years and of those with MRE-positive Crohn disease was 40.2 years. No statistical difference was found between the groups with respect to sex (p = 0.152) or age (p = 0.933).
Determination of Imaging Findings Specific for Behçet Disease
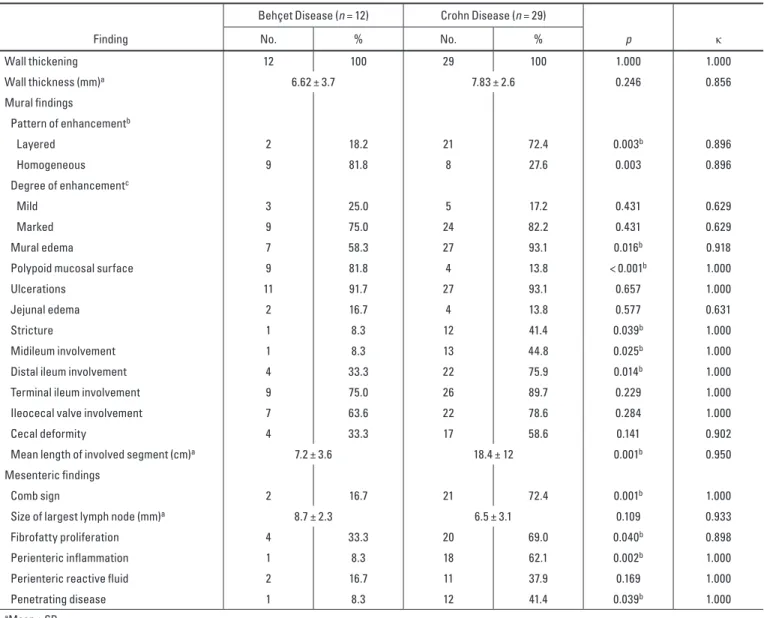
The frequency of MRE findings in the Behçet and Crohn disease groups, the statistical dif-ferences in frequencies of abnormal MRI findings between the two groups, and kappa values between the readers regarding MRE findings are shown in Table 3. Homoge-neous enhancement (p = 0.003) and polypoid mural surface (p < 0.001) were significant-ly more common in Behçet disease than in Crohn disease (Figs. 1–3). The length of in-volved segment was shorter in Behçet dis-ease than in Crohn disdis-ease (p = 0.001). No significant difference was found between the two groups in terms of presence and sever-ity of bowel wall thickening. Mural edema, TABLE 2: Frequency of Extraintestinal Clinical Features in Study Patients
With Behçet Disease With Intestinal Involvement
Featurea No. Frequency (%)
Oral aphthous ulcers 30/30 100
Genital ulceration 18/30 60
Eye diseaseb 14/30 47
Deep venous thrombosis, thrombophlebitis 6/29 21
Papulopustular lesions 20/28 71
Erythema nodosum–like lesions 11/27 41
Neurologic signs 10/27 37
Arthritis, arthropathy 21/27 78
aRare manifestations of Behçet disease in study patients were cardiac involvement (n = 2), perianal fistula (n = 2), pulmonary symptoms (n = 2), abdominal aortic aneurysm (n = 1), aortic occlusion (n = 1), submandibular gland involvement (n = 1), and primary sclerosing cholangitis (n = 1).
bUveitis, iridocyclitis.
A
Fig. 1—49-year-old man with 15-year history of intestinal Behçet disease and 6-month history of abdominal symptoms. Biopsy showed inflammation characterized by ulcer and cryptitis.
A, Coronal T2-weighted single-shot fast spin-echo (SSFSE) MR image shows polypoid mural thickening (arrows) in terminal ileum. Lobulated surface facing lumen is evident. B, Coronal heavily T2-weighted thin-slice SSFSE image shows deep and shallow ulcers (arrows) between polypoid lesions in terminal ileum.
C B
stricture, mid or distal ileal involvement, and mesenteric findings, such as fibrofatty prolif-eration, comb sign, perienteric inflammation, and penetrating disease, were significantly more prevalent in the Crohn disease group than in the intestinal Behçet disease group (Table 3).
DW images showed mural restricted dif-fusion in all 12 patients with abnormal MRE findings. Ileoileal fistula as a complication of intestinal Behçet disease was detected at MRE in one patient (Fig. 4). A patient with a history of intestinal obstruction 10 years previously who was treated by right hemico-lectomy and ileotransversostomy had MRE findings of recurrent disease along the ileal side of the ileocolic anastomosis. In
addi-tion, a patient with normal MRE findings had colonoscopic findings of colonic perforation 6 years previously, and another patient had a previous gastrointestinal bleeding episode as a complication of Behçet disease.
The kappa values for the two readers are shown in Table 3. Concerning the degree of mural contrast enhancement (κ = 0.629) and jejunal edema (κ = 0.631), interobserver agree-ment was moderate. The kappa values for all other findings ranged between 0.896 and 1.000, indicating excellent interobserver agreement. Initial Performance Estimates
Out of all imaging findings, polypoid pattern (p = 0.003) and homogeneous mural enhance-ment (p = 0.000) were the findings
significant-ly associated with Behçet disease. The sensi-tivity, specificity, and accuracy of these two qualitative variables for differentiating Behçet disease and Crohn disease in patients are shown in Table 4 with corresponding 95% CIs. The ROC curves of the polypoid mural surface and homogeneous enhancement pattern yield-ed AUCs of 0.806 (95% CI, 0.644–0.968) and 0.779 (95% CI, 0.621–0.936).
Because the interobserver agreement was very good, the diagnostic efficacy of MRE was calculated only for the experi-enced reader. The sensitivity of MRE was 57.14% (95% CI, 34.02–78.18%); specifici-ty, 100% (95% CI, 66.37–100%); accuracy, 70.00% (95% CI, 50.60–85.27%); positive predictive value, 100% (95% CI, 85.90– A
Fig. 2—24-year-old man with 10-year history of Behçet disease and 4-year history of intestinal involvement. Histopathologic examination revealed diffuse active ileitis.
A, Coronal steady-state free precession MR image shows mural polypoid (P) wall thickening with deep penetrating ulcers. Asterisks indicate ileocecal valve with ulcer (arrow) on its surface. Small ulcers at ileocecal valve have also been reported at colonoscopy. C indicates deformed cecum. B, Coronal contrast-enhanced fat-suppressed T1-weighted 3D gradient-echo image shows homogeneous enhancement (arrow) in thickened bowel wall. C indicates deformed cecum.
B
A
Fig. 3—55-year-old man with 5-year history of intestinal Behçet disease. Intestinal involvement was initial manifestation. At colonoscopy, superficial erosions with stenosed orifice were detected on ileocecal valve. Terminal ileum was partially intubated. Histopathologic diagnosis was focal active ileitis.
A–C, Coronal single-shot fast spin-echo (SSFSE) (A), coronal heavily T2-weighted thin-slice SSFSE (B), and coronal contrast-enhanced fat-suppressed T1-weighted 3D gradient-echo (C) MR images show wall thickening and mucosal irregularity (ulcerations) with small polypoid structures (P, A, C) in terminal ileum (large arrow). Small arrows indicate stricture at level of ileocecal valve. Asterisks indicate upper and lower lips of lipomatous and hypertrophied ileocecal valve. C indicates cecum.
C B
TABLE 3: Frequency of Abnormal MRI Findings at MR Enterography
Finding
Behçet Disease (n = 12) Crohn Disease (n = 29)
p κ No. % No. % Wall thickening 12 100 29 100 1.000 1.000 Wall thickness (mm)a 6.62 ± 3.7 7.83 ± 2.6 0.246 0.856 Mural findings Pattern of enhancementb Layered 2 18.2 21 72.4 0.003b 0.896 Homogeneous 9 81.8 8 27.6 0.003 0.896 Degree of enhancementc Mild 3 25.0 5 17.2 0.431 0.629 Marked 9 75.0 24 82.2 0.431 0.629 Mural edema 7 58.3 27 93.1 0.016b 0.918
Polypoid mucosal surface 9 81.8 4 13.8 < 0.001b 1.000
Ulcerations 11 91.7 27 93.1 0.657 1.000
Jejunal edema 2 16.7 4 13.8 0.577 0.631
Stricture 1 8.3 12 41.4 0.039b 1.000
Midileum involvement 1 8.3 13 44.8 0.025b 1.000
Distal ileum involvement 4 33.3 22 75.9 0.014b 1.000
Terminal ileum involvement 9 75.0 26 89.7 0.229 1.000
Ileocecal valve involvement 7 63.6 22 78.6 0.284 1.000
Cecal deformity 4 33.3 17 58.6 0.141 0.902
Mean length of involved segment (cm)a 7.2 ± 3.6 18.4 ± 12 0.001b 0.950
Mesenteric findings
Comb sign 2 16.7 21 72.4 0.001b 1.000
Size of largest lymph node (mm)a 8.7 ± 2.3 6.5 ± 3.1 0.109 0.933
Fibrofatty proliferation 4 33.3 20 69.0 0.040b 0.898
Perienteric inflammation 1 8.3 18 62.1 0.002b 1.000
Perienteric reactive fluid 2 16.7 11 37.9 0.169 1.000
Penetrating disease 1 8.3 12 41.4 0.039b 1.000
aMean ± SD.
bStatistically significant result. cEnhancement in enteric phase.
Fig. 4—47-year-old man with surgically verified ileoileal fistula due to intestinal Behçet disease and 20-year history of Behçet disease. Colon and terminal ileum were macroscopically normal at colonoscopy. A and B, Coronal T2-weighted single-shot fast spin-echo (A) and coronal contrast-enhanced fat-suppressed T1-weighted 3D gradient-echo (B) MR images show ileoileal fistula (center arrow). Polypoid (P) mural thickening and spiculations are adjacent to serosal surface of involved distal ileum. Ileocecal valve is open (upper left arrows). Histopathologic examination revealed active ileitis. C indicates cecum.
99.70); and negative predictive value, 50.00% (95% CI, 37.90–62.10%).
Discussion
In our study, we found high specificity and positive predictive value of MRE in the detec-tion of intestinal Behçet disease. In a patient with known Behçet disease, the presence of ab-normal MRE findings suggests that the patient most likely has intestinal involvement. Howev-er, as found in our study, this method has low sensitivity of only 57.14% in the detection of the small-bowel lesions of Behçet disease. The low sensitivity found in our study may be ex-plained by the fact that most patients had subtle bowel lesions.
Data obtained in conventional and capsule endoscopic studies have shown that most pa-tients with intestinal Behçet disease have mild changes in the small bowel [25, 26] and that well-established techniques of imaging of the small intestine, such as barium studies, are in-sufficient for identifying small-intestinal le-sions [27]. Although the frequency of ulcers increases toward the distal intestine in Behçet disease [26], several capsule endoscopic stud-ies have revealed a considerable number of le-sions not only in the terminal ileum, which is known to be a more frequently affected site of Behçet disease, but also in the proximal and mid portions of the small bowel [25, 28].
Neves et al. [29] reported that the jejunum is the most frequently affected part of the small bowel in intestinal Behçet disease and that je-junal erosions and ulcerations are found in 80% of patients. The lesions of intestinal Behçet disease are predominantly superficial and even radiologically invisible, including erythema-tous color changes, petechiae, and erosions [25, 29]. These subtle changes, even if they are suspected radiologically, can cause problems in that they cannot be reached with routine en-doscopic methods and so they cannot be con-firmed clinically.
Biopsy can reveal histopathologic changes even though colonoscopic findings are mac-roscopically normal with respect to Behçet disease lesions. For example, Köklü et al. [25] reported that 61% of patients with Be-hçet disease with normal endoscopic find-ings in the colon and terminal ileum had ab-normal histologic findings in the ileum. The problem is not only determining the presence of gastrointestinal involvement in a patient with known Behçet disease but also making the diagnosis of Behçet disease in a patient in whom nonspecific lesions, such as ulcers, are found at ileocolonoscopy.
Intestinal Behçet disease often mimics in-flammatory bowel disease, particularly Crohn disease [9, 16–19]. In our study, patients with Crohn disease who had undergone MRE dur-ing the study period were accepted as control subjects for evaluation of the clinical signifi-cance of the small-bowel lesions of Behçet dis-ease. We can refer to two MRE findings that have been found to be fairly characteristic of intestinal involvement: polypoid appearance of the intestinal surface and homogeneous (not layered) enhancement of the small-bow-el wall (AUC values for polypoid surface and homogeneous enhancement were 0.806 and 0.779). These two findings were significantly more frequent in patients with Behçet disease than those with Crohn disease in our study. Layered (stratified) enhancement pattern, on the contrary, was more common in patients with Crohn disease. The so-called target sign, which is, in a way, similar to the layered pat-tern, was also reported to be a significantly frequent finding in Crohn disease compared with Behçet disease [18].
The polypoid mural surface seen in the study patients with Behçet disease may be caused by nodular intestinal mucosa sur-rounding the penetrating ulcers or may devel-op as a consequence of alternating cycles of inflammation and regeneration of the ulcer-ated epithelium (which can be categorized as pseudopolyps). Ha and colleagues [19] previ-ously reported polypoid lesions as a notewor-thy finding, Those authors evaluated the CT findings of intestinal Behçet disease and found them present in 10 of 28 (35.7%) patients. These lesions, which may exhibit marked con-trast enhancement, frequently involve both the terminal ileum and the cecum [12].
In a pediatric case of intestinal Behçet dis-ease [23], diffuse bowel wall thickening with a polypoid appearance was remarkable on MRE images. In a study conducted by Zhang et al. [18], intraluminal pseudopolyp formation was encountered at imaging in only 19% of pa-tients with intestinal Behçet disease, but it was found in 59.8% of patients with Crohn disease. In that study, however, detailed information about the nature and morphologic features of the lesions that the authors considered pseu-dopolyps was not given. The appearance they referred to as pseudopolyp could be quite dif-ferent from what we considered polypoid mu-ral surface.
In Behçet disease, intestinal ulcers are gen-erally large (> 2 cm), sharply demarcated, and deep and have nodular margins [30–32]. They have a punched-out appearance and penetrate
T A B LE 4 : E st im at ed P er fo rm an ce V al ue s f or P ol yp oi d a nd H om og en eo us P at te rn a nd C om bi na ti on o f t he T w o V ar ia bl es f or D iff er en ti at in g B eh çe t D is ea se ( n = 1 2) a nd C ro hn D is ea se ( n = 2 9) i n P at ie nt s W it h A bn or m al M R E nt er og ra ph ic F in di ng s Pa tter n Tr ue - Po si tive (n o. ) Tr ue - N ega tiv e (n o. ) Fa lse - Po si tive (n o. ) Fa lse -N ega tiv e (n o. ) Se ns iti vi ty Sp eci fici ty Ac cu ra cy AU C % No . 95 % C I % No . 95 % C I % No . 95 % C I Va lu e 95 % C I Po ly poi d p at te rn 9 25 4 3 75 .0 0 9/ 12 42 .8 1–94 .5 1 86 .21 25 /29 68 .3 4– 96 .11 82 .9 3 34 /41 67 .9 4– 92 .85 0. 80 6 0. 64 4– 0. 96 8 Ho m og ene ou s pa tter n 10 21 8 2 83. 33 10 /1 2 51 .59 –97 .9 1 72 .4 1 21/ 29 52. 76 –8 7. 27 75 .61 31 /41 59 .7 0– 87. 64 0.7 79 0. 62 1– 0. 93 6 Po ly po id o r h om og ene ou s pa tter n a 11 17 12 1 91. 67 11 /1 2 61 .5 2– 99. 79 58 .6 2 17/ 29 38 .9 4– 76. 48 68 .2 9 28/ 41 51. 91 –8 1. 92 0. 75 1 0. 59 8– 0. 90 5 Bo th po ly poi d a nd h om og en eo us pa tter n b 8 29 0 4 66 .6 7 8/ 12 34 .8 9– 90 .0 8 10 0 29/2 9 88 .06 –1 00 90 .2 4 37/ 41 76. 87 –9 7. 28 0. 83 3 0. 66 5– 1. 00 2 N ot e— N um be rs w ith v irg ul es a re r aw d at a u se d t o c al cu la te p er ce nt ag es . aPr es en ce o f o ne o f t he c rit er ia i s e no ug h f or B eh çe t d is ea se d ia gn os is . bPr es en ce o f b ot h c rit er ia i s n ee de d f or B eh çe t d is ea se d ia gn os is .
deeply into the muscularis propria. The ul-cers of Crohn disease, however, are mostly longitudinal in shape [18]. Cheon and Kim [33], who suggested novel diagnostic criteria for intestinal Behçet disease, using systemic and colonoscopic features, regarded five or fewer lesions, oval shape, deep penetrating nature, discrete border, and ileocecal loca-tion as typical ulceraloca-tions of Behçet disease. Ulcerations that did not fulfill all of the char-acteristics, such as several tiny, shallow, oral aphthous ulcers, were regarded as atypical. Su-perficial ulcers in Turkish patients, mostly lo-cated in the terminal ileum, differ from the sin-gle, large, sharply demarcated ulcers described in eastern Asia [11, 32]. These superficial le-sions are considered potentially reversible and may be efficiently treated medically.
In Behçet disease, volcano-type and geo-graphic ulcers have also been described. Cecal contraction, widening of the ileoce-cal valve, fold thickening as a consequence of ulceration, and, occasionally, aneurysmal dilatation of the terminal ileum are the im-portant manifestations of intestinal Behçet disease [30, 34, 35]. The ulcers of Behçet disease are much more prone to perforation and bleeding [16, 36]. One study showed the rate of perforation to be 12.7%; fistula, 7.6%; stricture, 7.2%; and abscess, 3.3% [37, 38]. In our study, enteroenteric fistula and stricture with proximal dilatation were detected in only one patient each. One of these patients had perforation, and the other had a gastroin-testinal bleeding episode.
Although ileocecal involvement is most commonly (88–96%) described [18, 32, 39], Behçet disease may involve any segment of the alimentary tract and the various gastro-intestinal organs [27, 29, 40]. The involved small-bowel segment was shorter than in Crohn disease (7.2 ± 3.6 vs 18.4 ± 12 cm), and this emerged as a statistically significant (p = 0.001) finding in our study. The aver-age length of involved bowel was 6.4 cm in one report [12]. The involvement is more lo-calized than in Crohn disease [11], and the number of involved segments is reported to be significantly fewer in Behçet disease than in Crohn disease (76% vs 38%) [18].
The frequency of recurrence after surgical treatment varies from 40% to 80% among patients who have undergone surgical in-tervention [41, 42]. In those patients, lesions tend to recur at the anastomotic site, espe-cially along the ileal side of ileocolic anas-tomoses [12]. Most recurrent ulcers devel-op within 2 years after surgery [42]. In our
study, recurrence after right hemicolecto-my was detected with both colonoscopy and MRE in one patient.
Oral ulcers are known to be the most com-mon manifestation of Behçet disease; the prevalence ranges from 92% to 100%. In our study, the oral ulcers were found in 100% of cases. Genital ulcers and cutaneous lesions, together with ocular and articular involve-ments, are found to be the most frequent fea-tures of the disease in all countries [43]. Gas-trointestinal findings usually develop 4.5–6 years after the onset of oral ulcerations [33, 40, 44]. It is interesting that in our study ar-ticular manifestations, such as arthralgia and arthritis, were more common than genital ul-cers, ocular lesions, and cutaneous involve-ment. Joint problems were present in 77% of the study patients. The frequency of articu-lar involvement varies considerably in dif-ferent studies. It is reported to be present in 11.6–84% of patients with Behçet disease [3, 43, 45]. The number of joint problems in our study may have been high because the main contributor to the patient group was a rheu-matologist from a multidisciplinary Behçet disease team at our hospital. Nonspecific ar-thralgia without objective signs of arthritis, such as swelling and effusion, is common in patients with Behçet disease.
Our study had several limitations. These include its single-center design, small sample size, reliance on retrospective medical chart review for evaluation of the patient data, and lack of a reference standard, such as capsule endoscopy or surgical findings, for verifica-tion of the intestinal lesions. Studies con-ducted with video capsule endoscopy have shown that Behçet disease can involve the entire small bowel. This technique can show all lesions, including erosions and oral aph-thous ulcers, located throughout the small bowel, not only at the level of the distal ileum [26, 28, 29]. Moreover, because capsule en-doscopy was not performed, we could not discern the real nature of mural T2 hyperin-tensity in the jejunum in both the Behçet dis-ease and the Crohn disdis-ease groups, which we speculated was jejunal edema.
Conclusion
Intestinal Behçet disease shares several MRE findings with Crohn disease and falls within the category of diagnosis of exclusion. MRE has potential for use as a radiation-free alternative for clarifying the cause of nonspe-cific gastrointestinal symptoms in patients with known Behçet disease. In patients
with-out an established diagnosis of Behçet disease, polypoid pattern of the bowel surface may be a valuable finding and favor a diagnosis of intestinal Behçet disease over Crohn disease. Stricture formation, long-segment disease, and involvement of more proximal ileal seg-ments favor small-bowel Crohn disease. The radiologist’s familiarity with these findings can be used to suggest intestinal Behçet dis-ease in patients with small-bowel inflamma-tion or to distinguish it from Crohn disease. However, additional studies involving more subjects and correlation with capsule endos-copy are needed to determine the actual value of MRE in patients with Behçet disease and to validate the clinical usefulness of the tech-nique in the detection of unknown intestinal Behçet disease.
References
1. Behcet H. Rezidivierende aphthose, durch ein virus verusachte geschwure am auge und an den genital-ien. Dermatol Wochenschr 1937; 105:1152–1157 2. Behçet H, Matteson EL. On relapsing, aphthous
ulcers of the mouth, eye and genitalia caused by a virus [1937]. Clin Exp Rheumatol 2010; 28(suppl 60):S2–S5
3. Tursen U, Gurler A, Boyvat A. Evaluation of clin-ical findings according to sex in 2313 Turkish pa-tients with Behçet’s disease. Int J Dermatol 2003; 42:346–351
4. Alpsoy E, Donmez L, Onder M, et al. Clinical fea-tures and natural course of Behcet’s disease in 661 cases: a multicentre study. Br J Dermatol 2007; 157:901–906
5. Balta I, Akbay G, Kalkan G, Eksioglu M. Demo-graphic and clinical features of 521 Turkish pa-tients with Behçet’s disease. Int J Dermatol 2014; 53:564–569
6. Davatchi F, Shahram F, Chams-Davatchi C, et al. Behcet’s disease: from East to West. Clin
Rheumatol 2010; 29:823–833
7. Lakhanpal S, Tani K, Lie JT, Katoh K, Ishigatsubo Y, Ohokubo T. Pathologic features of Behçet’s syndrome: a review of Japanese autopsy registry data. Hum Pathol 1985; 16:790–795
8. Chae EJ, Do KH, Seo JB, et al. Radiologic and clin-ical findings of Behçet disease: comprehensive re-view of multisystemic involvement. RadioGraphics 2008; 28:e31
9. Park JJ, Kim WH, Cheon JH. Outcome predictors for intestinal Behçet’s disease. Yonsei Med J 2013; 54:1084–1090
10. Chung SY, Ha HK, Kim JH, et al. Radiologic find-ings of Behçet syndrome involving the gastroin-testinal tract. RadioGraphics 2001; 21:911–924; discussion, 924–926
11. Kara T, Düşmez Apa D. Pathologic
tures of Behçet’s disease in the tubular gut. Patholog Res Int 2012; 2012:216254
12. Ebert EC. Gastrointestinal manifestations of Behçet’s disease. Dig Dis Sci 2009; 54:201–207
13. International Study Group for Behçet’s Disease. Criteria for diagnosis of Behçet’s disease. Lancet 1990; 335:1078–1080
14. Mizushima Y, Inaba G, Himura Y, Ohno S. Diag-nostic criteria for Behçet’s disease in 1987, and guideline for treating Behçet’s disease. Saishin
Igaku 1988; 43:391–393
15. Cheon JH, Kim ES, Shin SJ, et al. Development and validation of novel diagnostic criteria for intestinal Behçet’s disease in Korean patients with ileocolonic ulcers. Am J Gastroenterol 2009; 104:2492–2499 16. Grigg EL, Kane S, Katz S. Mimicry and
decep-tion in inflammatory bowel disease and intestinal Behçet disease. Gastroenterol Hepatol (NY) 2012; 8:103–112
17. Valenti S, Gallizzi R, De Vivo D, Romano C. Intestinal Behçet and Crohn’s disease: two sides of the same coin. Pediatr Rheumatol Online
J 2017; 15:33
18. Zhang T, Hong L, Wang Z, et al. Com-parison between intestinal Behçet’s disease and Crohn’s disease in characteristics of symptom, endoscopy, and radiology. Gastroenterol Res
Pract 2017; 2017:3918746
19. Ha HK, Lee HJ, Yang SK, et al. Intestinal Behçet syndrome: CT features of patients with and pa-tients without complications. Radiology 1998; 209:449–454
20. Johnson WK, Beierle E, Ros PR. CT evaluation of the gastrointestinal tract in a patient with Behçet’s syndrome. AJR 1994; 162:349–350
21. Park MJ, Lim JS. Computed tomography enterog-raphy for evaluation of inflammatory bowel dis-ease. Clin Endosc 2013; 46:327–336
22. You JK, Kim MJ, Park S, Chung JJ, Kim WH. In-testinal Behçet’s disease: breath-hold MR imag-ing. Abdom Imaging 2001; 26:309–314
23. Jung YS, Park DI, Moon CM, et al. Radiation ex-posure from abdominal imaging studies in pa-tients with intestinal Behçet disease. Gut Liver 2014; 8:380–387
24. D’Angelo T, Gallizzi R, Romano C, Cicero G, Mazziotti S. Magnetic resonance enterography findings of intestinal Behçet disease in a child.
Case Rep Radiol 2017; 2017:8061648
25. Köklü S, Yüksel O, Onur I, et al. Ileocolonic in-volvement in Behçet’s disease: endoscopic and his-tological evaluation. Digestion 2010; 81:214–217 26. Arimoto J, Endo H, Kato T, et al. Clinical value of
capsule endoscopy for detecting small bowel le-sions in patients with intestinal Behçet’s disease.
Dig Endosc 2016; 28:179–185
27. Hamdulay SS, Cheent K, Ghosh C, Stocks J, Ghosh S, Haskard DO. Wireless capsule endoscopy in the investigation of intestinal Behçet’s syndrome.
Rheumatology (Oxford) 2008; 47:1231–1234
28. Satake M, Sakuraba H, Hiraga H, et al. Capsule endoscopy for differentiating early Crohn’s dis-ease from Behçet’s disdis-ease. J Inflamm Bowel Dis
Disord 2016; 1:108
29. Neves FS, Fylyk SN, Lage LV, et al. Behçet’s dis-ease: clinical value of the video capsule endosco-py for small intestine examination. Rheumatol Int 2009; 29:601–603
30. Rosenberger A, Adler OB, Haim S. Radiological aspects of Behçet’s disease. Radiology 1982; 144:261–264
31. Goldstein SJ, Crooks DJ. Colitis in Behçet’s syn-drome. Radiology 1978; 128:321–323
32. Lee CR, Kim WH, Cho YS, et al. Colonoscopic findings in intestinal Behçet’s disease. Inflamm
Bowel Dis 2001; 7:243–249
33. Cheon JH, Kim WH. An update on the diagnosis, treatment, and prognosis of intestinal Behçet’s disease. Curr Opin Rheumatol 2015; 27:24–31 34. Kim JH, Choi BI, Han JK, Choo SW, Han MC.
Colitis in Behçet’s disease: characteristics on double-contrast barium enema examination in 20
patients. Abdom Imaging 1994; 19:132–136 35. Korman U, Cantasdemir M, Kurugoglu S, et al.
Enteroclysis findings of intestinal Behçet disease: a comparative study with Crohn disease. Abdom
Imaging 2003; 28:308–312
36. Moon CM, Cheon JH, Shin JK, et al. Prediction of free bowel perforation in patients with intestinal Behçet’s disease using clinical and colonoscopic findings. Dig Dis Sci 2010; 55:2904–2911 37. Jung YS, Cheon JH, Park SJ, Hong SP, Kim TI,
Kim WH. Long-term clinical outcomes of Crohn’s disease and intestinal Behçet’s disease. Inflamm
Bowel Dis 2013; 19:99–105
38. Chung HJ, Goo BC, Lee JH, et al. Behçet’s dis-ease combined with various types of fistula.
Y onsei Med J 2005; 31:625–628
39. Wu QJ, Zhang FC, Zhang X. Adamantiades-Behçet‘s disease complicated gastroenteropathy. World J
Gastroenterol 2012; 18:609–615
40. Skef W, Hamilton MJ, Arayssi T. Gastrointestinal Behçet’s disease: a review. World J Gastroenterol 2015; 7:3801–3812
41. Kasahara Y, Tanaka S, Nishino M, Umemura H, Shi-raha S, Kuyama T. Intestinal involvement in Behçet’s disease: review of 136 surgical cases in the Japanese literature. Dis Colon Rectum 1981; 24:103–106 42. Iida M, Kobayashi H, Matsumoto T, et al.
Postop-erative recurrence in patients with intestinal Behçet’s disease. Dis Colon Rectum 1994; 37:16–21 43. Alpsoy E. Behçet’s disease: a comprehensive
re-view with a focus on epidemiology, etiology and clinical features, and management of mucocuta-neous lesions. J Dermatol 2016; 43:620–632 44. Kim DH, Cheon JH. Intestinal Behcet’s disease: a
true inflammatory bowel disease or merely an in-testinal complication of systemic vasculitis? Yonsei Med J 2016; 57:22–32
45. Seo J, Lee M, Choi MJ, et al. Predictive value of bone scintigraphy for the detection of joint in-volvement in Behçet’s disease: dermatologists’ perspectives. Eur J Dermatol 2015; 25:477–482