CASE
REPORT
–
OPEN
ACCESS
InternationalJournalofSurgeryCaseReports14(2015)77–79
ContentslistsavailableatScienceDirect
International
Journal
of
Surgery
Case
Reports
j o u r n al ho m e p a g e :w w w . c a s e r e p o r t s . c o m
Retroperitoneal
paraganglioma
presenting
with
pancytopenia:
A
rare
case
with
rare
manifestation
Mutlu
Ünver
a,∗,
S¸
afak
Öztürk
a,
Varlık
Erol
b,
Erdem
Barıs¸
Cartı
c,
Osman
Bozbıyık
d,
Eyüp
Kebapc¸
ı
e,
Mustafa
Ölmez
e,
Gökhan
Akbulut
ea˙IzmirUniversity,DepartmentofGeneralSurgery, ˙Izmir,Turkey bBas¸kentUniversity,DepartmentofGeneralSurgery, ˙Izmir,Turkey cAydınStateHospital,DepartmentofGeneralSurgery,Aydın,Turkey dAfyonKocatepeUniversity,DepartmentofGeneralSurgery,Afyon,Turkey
eTepecikEducationandResearchHospital,DepartmentofGeneralSurgery, ˙Izmir,Turkey
a
r
t
i
c
l
e
i
n
f
o
Articlehistory: Received2July2015
Receivedinrevisedform18July2015 Accepted20July2015
Availableonline28July2015
Keywords: Paraganglioma Pancytopenia Retroperitoneal Reactivethrombocytosis
a
b
s
t
r
a
c
t
INTRODUCTION:Paragangliomas aretumorsthatarisefromextraadrenalchromaffincellsand most ofthemareasymptomaticpresentingwithpainlessmass.Retroperitonealparagangliomasaremostly benignwithgoodprognosis;however,theycanpresentwithabdominalpain,palpablemass,or hyper-tensiveepisodes.Surgicalresectionisstillthemaintreatmentandnecessaryforhistologicalassessment. CASEREPORT:A41yearoldfemalepatientpresentedwith6monthsoflossofappetite,weightloss, weaknessandbreathlessnessonexertion..Thepatient’sinitialbloodexaminationshowedmarked ane-mia,reducedleukocytecountwithneutropeniaandlymphopeniaandamarkedreductionintheplatelet count.Thepatientwasadmittedforevaluationofherpancytopenia.Magneticresonanceimagingrevealed a8×7×8cmsizedmassclosedtothepancreatictailinvadingsplenichilum.Alargemasswasidentified retroperitoneally,closedtothetailofpancreaswithasplenichiluminvasion.Totalmassresectionand splenectomywasperformed.
DISCUSSION:Completesurgicalexcisionisthetreatmentofchoiceforextra-adrenalparagangliomasas wellasforrecurrentormetastaticneoplasms.Reactivethrombocytosisisacommoncauseof thrombocy-tosis.Splenectomywasfoundtobeoneofthemaincausesofextremereactivethrombocytosis.Reactive thrombocytosisisapredictablefindingaftersplenectomyandmanagementofthethrombocytosisand preventionofcomplicationsshouldbeinitiated.
©2015TheAuthors.PublishedbyElsevierLtd.onbehalfofSurgicalAssociatesLtd.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Paragangliomasaretumorsthatarisefromextraadrenal chro-maffincellsandcandevelopeatvarioussitesofthebodyincluding thehead,neck,thoraxand theabdomen.Mostof the paragan-gliomasareasymptomaticpresentingwithpainlessmass.About 75%ofparagangliomasare sporadicand 85%ofparagangliomas developintheabdominalcavity[1].
Whenpresentingwithintheabdominalcavity,theymayariseas aprimaryretroperitonealneoplasmandcanmimicvascular mal-formationsorotherconditionsrelatedtospecificretroperitoneal organssuchasthepancreas,kidneys,oradrenals.Retroperitoneal paragangliomasarisefromspecializedneuralcrestderived cells distributed alongthe aortainassociationwiththesympathetic
∗ Correspondingauthorat: ˙IzmirUnivercity,DepartmentofGeneralSurgery,Yeni GirneBulv.1825skno.12,Kars¸ıyaka, ˙Izmir,Turkey.Fax:+902323423371.
E-mailaddress:[email protected](M.Ünver).
chain.Retroperitonealparagangliomasmainlyaffectadultswho are in the fourth or fifth decade of life, and they have nosex predilection[2].Retroperitonealparagangliomasaremostlybenign withgood prognosis; however, theycan present with abdomi-nal pain, palpable mass, or hypertensive episodes [3]. Patients withsecretorytumorsexperienceparoxysmalepisodic hyperten-sion, as wellas the typical triad of symptoms associated with pheochromocytomas, for example, palpitations, headache and sweating.Nonfunctionalparagangliomasmostcommonlymanifest asabdominalpainoramass[4].Inthepresentcase,wereporta rarecaseofaretroperitonealparagangliomapresentingwith pan-cytopenia.
2. Casereport
A41yearoldfemalepatientpresentedwith6monthsofloss of appetite,weightloss,weakness,and breathlessnesson exer-tion.Therewasnohistoryofsmokingandalcohol abuse.There wasnoremarkablefamilyhistory.Onadmission,vitalsigns(blood
http://dx.doi.org/10.1016/j.ijscr.2015.07.021
2210-2612/©2015TheAuthors.PublishedbyElsevierLtd.onbehalfofSurgicalAssociatesLtd.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://
creativecommons.org/licenses/by-nc-nd/4.0/).
Downloaded for Anonymous User (n/a) at Baskent University from ClinicalKey.com by Elsevier on November 20, 2019. For personal use only. No other uses without permission. Copyright ©2019. Elsevier Inc. All rights reserved.
CASE
REPORT
–
OPEN
ACCESS
78 M.Ünveretal./InternationalJournalofSurgeryCaseReports14(2015)77–79
Fig.1.T2weightedaxialMRIimage(redarrowshowsthespleenandyellowarrow showsthemasswhichiscentrallyhyperintenseandperiferallyhypointense).(For interpretationofthereferencestocolorinthisfigurelegend,thereaderisreferred tothewebversionofthisarticle.)
pressure,heartrate,respirationrate,andbodytemperature)were withinnormallimits.Therewasnoperipherallymphadenopathy, hepatomegalyorsplenomegalyinphysicalexamination.Theinitial bloodexaminationshowedmarkedanemia(Hb=7.6g/dl),reduced leukocytecount(2100/cumm)withneutropeniaandlymphopenia andamarkedreductionintheplateletcount(70,000platelets/cu mm).Arepeatcompletebloodcount(CBC)showedsimilarresults. Basic metabolic panel,chest X-ray film,and electrocardiogram resultswereallnormal.Tumormarkerassaysshowedthat alpha-fetoproteinwas7.2n/ml(normal0–8.1),carcinoembryonicantigen (CEA)was3ng/ml(normal0–5),carbohydrateantigen19–9(CA 19–9)was11U/ml(normal0–37).
The patient was admitted for evaluation of her pancytope-nia by haematology department. All the results, testing for humanimmunodeficiencyvirus(HIV), Epstein–Barrvirus(EBV), cytomegalovirus,hepatitis,parvovirusB19,andantinuclear anti-bodieswerenegative.B12andfolatelevelswereinnormallimits. Upper GI endoscopy and colonoscopy were also normal. Then bonemarrowaspirationwasperformedtoevaluatethecauseof pancytopenia.Theaspiratewasnormocellularandshowed nor-malmaturationofallthethreeseries.Thebonemarrowreaction wasnormoblastic.AbdominalUSGwasperformedtorevealedthe dimensionsofthespleen.A 8×7sizecm massfrompancreatic tailtosplenichilumwasobservedintheabdominalUSG. Mag-neticresonanceimagingrevealeda8×7×8cmsizedmassclosed tothepancreatictailinvadingsplenic hilum(Fig.1).Thepatient underwentalaparotomywithamediansuperiorincision.Alarge masswasidentifiedretroperitoneally,closedtothetailofpancreas withasplenicveinocclusion.Totalmassresectionand splenec-tomywasperformed(Fig.2).Meanoperativetimewas120minand meanbloodlosswas200cc.Asignificantimprovementinthetotal leucocyteandplateletcountwasseenonthethirddayofsurgery. Therewasanincreaseinthehaemoglobinconcentrationbutwas thelastparametertoshowimprovement.Herplateletcountwas abnormallyelevatedto677,000platelets/cummpostoperativeday 6.Thepatientremainedasymptomaticatdischarge,andthe recom-mendationsfor reactivethrombocytosisaftersplenectomywere discussedwithher.Werecommendedmobilizationandincreased fluidintake.Shewasstartedon100mgofaspirindaily.Thepatient
Fig.2. Grosslycharacteristicbrownappearenceofthetumor.Tumormassis well-surcumscribedwithafibrouscapsule.
wasdischargedafter7postoperativeday.Onemonthfollowing surgery,bloodcountswereinnormallimits.Pathological exami-nationofthespecimenwasreportedasparaganglioma(Fig.3).
At 6-months follow-up, the patient’s complete blood count remainsnormalandabdominalCTdidnotrevealanyrecurrence ofthemass.
3. Discussion
Paragangliomas are extra-adrenal chromaffin tumours that developattheexpenseofneuroectodermalcellsoftheautonomous nervoussystem[5].Paragangliomascandevelopeatvarioussitesof thebodyincludingthehead,neck,thoraxandtheabdomen.Despite mostoftheparagangliomasareasymptomatic,retroperitonealand nonfunctioningformsareveryrare[6].Thefirstimagingmodality inthediagnosisofextra-adrenalparagangliomasismagnetic reso-nanceimaging(MRI)secondarytosuperiortissuecharacterization and absence of radiation hazards [7]. Computerized tomogra-phy(CT)scanalsohassensitivityof around90%for identifying extra-adrenalparagangliomasand theyappearas highly vascu-larstructurewithareasofintralesionalhemorrhageandnecrosis [8]. Metaiodobenzylguanidine scintigraphy (MIBG scintigraphy) hasoftenbeenusedasanimagingmodalityin thediagnosisof neuroendocrinetumors,butitlackssensitivityforextra-adrenal paragangliomas[1].
Completesurgicalexcisionisthetreatmentofchoicefor extra-adrenal paragangliomas as well as for recurrent or metastatic neoplasms[2].Patientwithmetastaticdiseasewillrequire adju-vantradiotherapywhilechemotherapyisrestrictedtopatientsnot accessibleforsurgeryandresistanttoradionuclidetherapy[9].
Reactivethrombocytosisisacommoncauseof thrombocyto-sis[10].Splenectomywasfoundtobeoneofthemaincausesof extremereactivethrombocytosisasinthepresentcase[11]. Reac-tivethrombocytosisisapredictablefindingaftersplenectomy,with theplateletcountpeakingat1to3weeksandreturningtonormal levelsinweeks,months,and,rarely,years[12].Essential throm-bocytosisisnot awell-recognizedcauseforarterialandvenous thrombosis.Managementofthethrombocytosisandpreventionof complicationsshouldbeinitiated[13].Thefirstlineoftherapyis theadministrationofplatelet-antiaggregatingmedicationsuchas aspirin[14].
Histopathologicalfindingsare notmuch useful to differenti-atebetweenbenignandmalignantparagangliomasonlyextensive localinvasion and distant metastasistoliver,bone, and lymph nodeshavebeenusedasindicatorsformalignancy[1,8]. Follow-up imaging is necessary in cases of patients with elevated
Downloaded for Anonymous User (n/a) at Baskent University from ClinicalKey.com by Elsevier on November 20, 2019. For personal use only. No other uses without permission. Copyright ©2019. Elsevier Inc. All rights reserved.
CASE
REPORT
–
OPEN
ACCESS
M.Ünveretal./InternationalJournalofSurgeryCaseReports14(2015)77–79 79
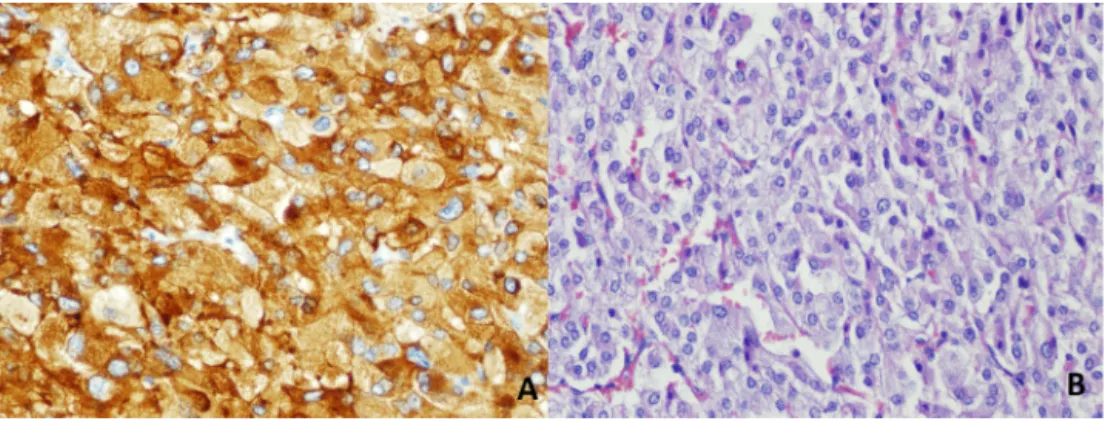
Fig.3.(A):ChromograninA:TumorcellsarediffuselypositiveforneuroendocrinemarkerChromograninAimmunohistochemically.(B):H&E:Welldefinednestsofcuboidal cellsseparatedbyhighlyvascularizedfibroussepta.Individualcellshaveamoderatelyabundantgranularbasophiliccytoplasm.
metanephrine and catecholaminelevelsor withnon functional original tumors [3]. Because of malignant potential and higher recurrencerateinparagangliomas,lifelongfollowupisalways rec-ommended[15].
4. Conclusion
Paragangliomas are very rare entities and has never been reported beforemanifesting withpancytopenia. Surgical resec-tion is still the main treatment and necessary for histological assessment.Reactivethrombocytosisisapredictablefindingafter splenectomyasinthepresentcase.Managementofthe thrombocy-tosisandpreventionofcomplicationsshouldbekeptinmindafter splenectomy.
Funding None. Consent
Writteninformedconsentwasobtainedfromthepatientfor publicationofthiscasereportandanyaccompanyingimages. Ethicalapproval
N/A.
Conflictofinterest None.
Authorcontribution
MutluÜnverM.D.;Studyconceptordesign,datacollection,data analysisorinterpretation,writingthepaper.
S¸afakÖztürkM.D.;Studyconceptordesign,datacollection,data analysisorinterpretation,writingthepaper.
VarlıkErol M.D.;Dataanalysis orinterpretation,writingthe paper.
ErdemBarıs¸CartıM.D.;Dataanalysisorinterpretation,writing thepaper.
OsmanBozbıyıkM.D.;Dataanalysisorinterpretation,writing thepaper.
EyüpKebapc¸ıM.D.;Studyconceptordesign,datacollection. MustafaÖlmezM.D.;Studyconceptordesign,datacollection. GökhanAkbulutM.D.;Studyconceptordesign,datacollection, dataanalysisorinterpretation,writingthepaper.
Gurantor MutluÜnver. References
[1]P.Brahmbhatt,P.Patel,A.Saleem,R.Narayan,M.Young,Retroperitoneal
paragangliomapresentingasachestpain:acasereport,CaseRep.Oncol.
Med.2013(2013)329472.
[2]W.C.Lin,H.Y.Wang,C.W.Chang,J.L.Lin,C.H.Tsai,Retroperitoneal
paragangliomamanifestingasparalyticileus:acasereport,J.Med.CaseRep.
6(June(1))(2012)158.
[3]D.Erickson,Y.C.Kudva,M.J.Ebersold,G.B.Thompson,C.S.Grant,J.A.van
Heerden,W.F.YoungJr,Benignparagangliomas:clinicalpresentationand
treatmentoutcomesin236patients,J.Clin.Endocrinol.Metab.86(2001)
5210–5216.
[4]G.A.Kaltsas,G.M.Besser,A.B.Grossman,Thediagnosisandmedical
managementofadvancedneuroendocrinetumors,Endocr.Rev.25(2004)
458–511.
[5]F.Crozier,E.Lechevallier,C.Eghazarian,M.André,D.Sammama,P.Wilshire,
V.Vidal,P.Pascal,J.M.Bartoli,Retroperitonealnonsecretingparaganglioma,J.
Radiol.80(1999)150–152.
[6]L.Louafy,A.Lakhloufi,R.Hamddaoui,F.Chehab,D.Khaiz,A.Bouzidi,
Non-functionalretroperitonealparaganglioma,Prog.Urol.11(2001)512–516.
[7]K.Y.Lee,Y.W.Oh,H.J.Noh,Y.J.Lee,H.S.Yong,E.Y.Kang,K.A.Kim,N.J.Lee,
Extraadrenalparagangliomasofthebody:imagingfeatures,AJRAm.J.
Roentgenol.187(2)(2006August)492–504.
[8]G.Sangster,D.Do,C.Previgliano,B.Li,D.LaFrance,M.Heldmann,Primary
retroperitonealparagangliomasimulatingapancreaticmass:acasereport
andreviewoftheliterature,HPBSurg.2010(2010)645728.
[9]K.F.Andersen,R.Altaf,A.Krarup-Hansen,B.Kromann-Andersen,T.Horn,N.J.
Christensen,H.W.Hendel,Malignantpheochromocytomasand
paragangliomas—theimportanceofamultidisciplinaryapproach,Cancer
Treat.Rev.37(April(2))(2011)111–119.
[10]M.Griesshammer,M.Bangerter,T.Sauer,R.Wennauer,L.Bergmann,H.
Heimpel,Aetiologyandclinicalsignificanceofthrombocytosis:analysisof
732patientswithanelevatedplateletcount,J.Intern.Med.245(3)(1999)
295–300.
[11]D.H.Buss,A.W.Cashell,M.L.O’Connor,F.Richards2nd,CaseLD,Occurrence,
etiology,andclinicalsignificanceofextremethrombocytosis:astudyof280
cases,Am.J.Med.96(3)(1994)247–253.
[12]Wintrobe’sClinicalHematology,in:J.P.Greer,J.Foerster,J.N.Lukens,G.M.
Rodgers,F.Paraskevas,B.Glader(Eds.),11thed.,LippincottWilliams&
Wilkins,Philadelphia,1981,pp.1128–1134.
[13]A.Tefferi,H.C.Hoagland,Issuesinthediagnosisandmanagementofessential
thrombocythemia,MayoClin.Proc.69(7)(1994)651–655.
[14]P.N.Khan,R.J.Nair,J.Olivares,L.E.Tingle,Z.Li,Postsplenectomyreactive
thrombocytosis,Proc.(Bayl.Univ.Med.Cent.)22(January(1))(2009)9–12.
[15]U.Shah,A.Giubellino,PacakK.Pheochromocytoma,implicationsin
tumorigenesisandtheactualmanagement,MinervaEndocrinol.37(June(2))
(2012)141–156.
OpenAccess
ThisarticleispublishedOpenAccessatsciencedirect.com.ItisdistributedundertheIJSCRSupplementaltermsandconditions,which permitsunrestrictednoncommercialuse,distribution,andreproductioninanymedium,providedtheoriginalauthorsandsourceare credited.
Downloaded for Anonymous User (n/a) at Baskent University from ClinicalKey.com by Elsevier on November 20, 2019. For personal use only. No other uses without permission. Copyright ©2019. Elsevier Inc. All rights reserved.