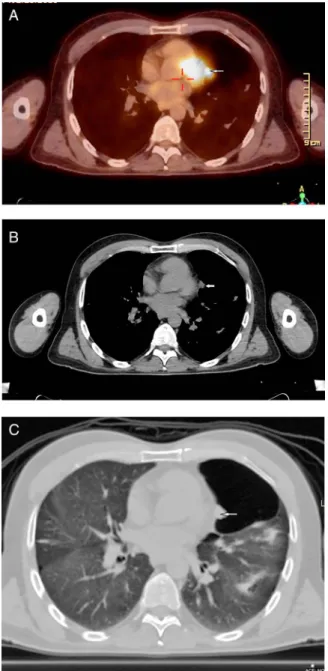
Rare presentation of a localised malignant pleural mesothelioma with cranial metastasis
Tam metin
Şekil
Benzer Belgeler
裝戴假牙注意事項 返回 醫療衛教 發表醫師 發佈日期 2010/02/03 裝卸
12 yaşından önce veya 40 yaşından sonra yeni ortaya çıkan davranış değişiklikleri ve psi- kiyatrik şikayetlerin varlığı, önceden psikiyatrik has- talık
A comparative analysis was applied to various Time series forecasting algorithm, in order to find which algorithm is the best algorithm to predict the future
In this article, we present a 59-year-old male patient who was admitted to our hospital with right pleural effusion and right-sided chest pain and diagnosed as
Thoracic computed tomography revealed a 12 mm ground-glass opacity lesion with a nodular component located at the superior segment of the lower lobe of the right lung.. The
Computed tomography also revealed a lytic lesion at medullary location in proximal radial diaphyseal area that caused a bow-like appearance in inner tabula and cortical
We present here a case of pulmonary cement embolism who presented with chest pain and shortness of breath 5 days after vertebroplasty for a thoracic vertebrae fracture,
Tomografilerde, daha önce tanımlanan servikal ve supraklavikular lenf nodlarının kaybolduğu, mediastinal kompartmanlarda patolojik boyutta lenf nodu olmadığı,
