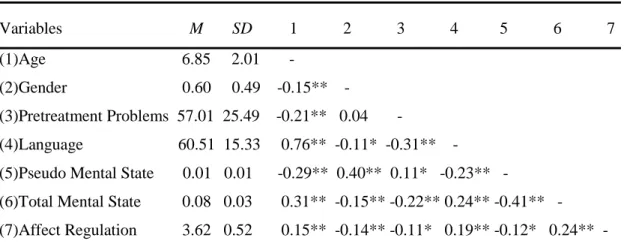
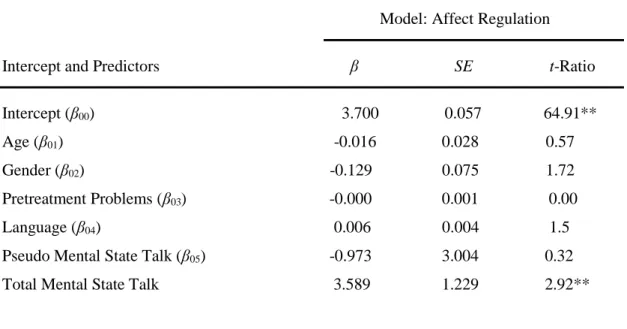
The relationship between the mentalization capacity of the children and affect regulation over the course of treatment
Tam metin
Şekil
Benzer Belgeler
Although our algorithm can solve the lot-sizing problem with any piecewise con- cave function, to compare the algorithm’s performance with an MIP solver, we use piecewise linear
However, in the current case, the patient denied any family medical history of detected hypertrophy of the palatine tonsil.. It was impossible to determine whether any other evidence
ağırlıklı olarak , kardiyak malformasyonlar, ho- loprozensefali ve ambigus genitalia ya eşlik eden imperfore anüs bulguları ile ring kromozom 13’e uyumlu olduğu görüldü 5
Küçük renal kitle (T1a) nedeniyle yapılan nefron koruyucu cerrahi yöntemlerin, radikal nefrektomi olguları ile benzer onkolojik sonuçlara ve uzun dönemde daha iyi fonksiyonel
En yaygın kullanılan traktör esaslı mekanizasyon düzeyi göstergeleri işlenen alana düşen traktör gücü (kW/ha), 1000 ha işlenen alana düşen traktör sayısı
Araştırma sonuçları baz alındığında, daha önce otel işletmelerinde eğlence hizmetleri yönetimiyle ilgili bir çalışmaların çok az olması ve çalışmanın
Regresyon analizi sonucuna göre, genel ruh sağlığını bağımsız ve anlamlı ölçüde yordayan faktörlerin ruhsal bozukluk öyküsü, düşük gelir düzeyi, kardeş
