A Research for People to Determine the Relationship between Oral Hygiene and Socio-Economic Status
Tam metin
Şekil
Benzer Belgeler
nelik çalışmaları ile klasik anaokulu kavra mından temel eğitim dışında tamamen ayrı lan okulda, temel eğitim programını sosyal ve görsel etkinliklerle
For several authors the main pathogenesis of each of the two types of isolated pontine infarction is suggested that the pathogenic mechanism of SDPI involves
Analytical methods are classified according to the measurement of some quantities proportional to the quantity of analyte. Classical Methods and
structure made out of stages that were attached to long spokes which converged at a central sun. This big construct was then tilted vertically, at a roughly 45 degree angle, in
Even with the limited number of total or partial facial transplant cases, we believe that a treatment protocol should be established for dental therapies in this patient group..
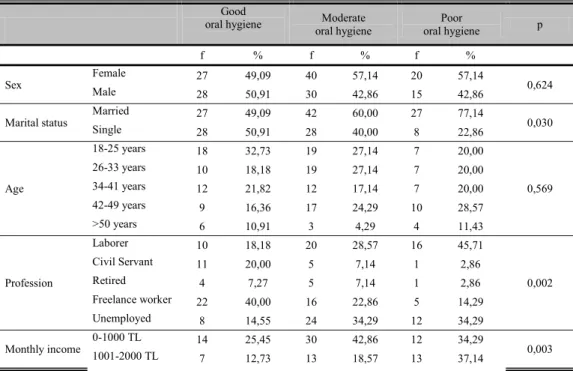
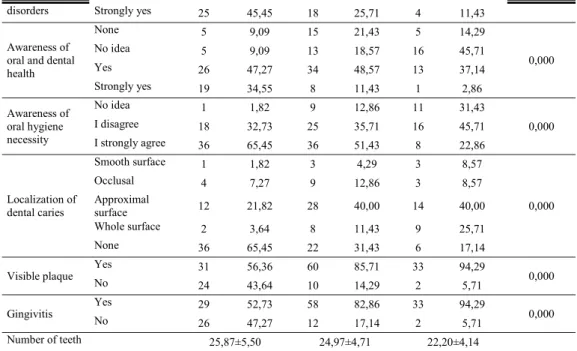
In this study, we aimed to determine the oral health care habits of patients admitted for treatment to a faculty of dentistry, along with the dental periodontal health status
In our study, there was no statistically significant relationship between the socio-economic levels and malocclusion classification of children reform of the health care
High and middle socio-eco- nomic status were found to be associated with atopic dermatitis; in contrast, subjects with a longer education period, higher family income, and having a
