Conventional Corneal Collagen Cross-Linking Versus
Transepithelial Diluted Alcohol and Iontophoresis-Assisted
Corneal Cross-Linking in Progressive Keratoconus
Kamil Bilgihan, MD,* Nilufer Yesilirmak, MD,* Yesim Altay, MD,
† Armagan Yuvarlak, MD,* and
Huseyin Baran Ozdemir, MD*
Purpose: To compare clinical outcomes of conventional corneal cross-linking (C-CXL) and diluted alcohol and iontophoresis-assisted corneal cross-linking (DAI-CXL) for the treatment of progressive keratoconus (KC).
Methods:Ninety-three eyes of 80 patients with KC were treated by C-CXL (n = 47) or DAI-CXL (n = 46). Visual acuity, keratometry, KC indexes, pachymetry, and aberrations were recorded before treatment and 1, 3, 6, and 12 months after treatment. The demarcation line was assessed 1 month after treatment.
Results: A significant improvement in visual acuity was
observed at month 3 and month 6 after DAI-CXL and C-CXL, respectively. A significant decrease in maximum keratometry was observed in both groups at month 6. The front symmetry index significantly improved in both groups after 6 months, whereas the Baiocchi Calossi Versaci index significantly improved only after DAI-CXL at month 12 (P = 0.01). Average keratometry and other KC indexes were stable during 12 months of follow-up. Central corneal thickness decreased by 28.6 and 40.2mm after DAI-CXL and C-CXL at month 1, respectively (P, 0.01), and it reached baseline at the 12th month (P = 0.14) only in the DAI-CXL group. Higher-order aberrations, coma, and spherical aberration signif-icantly worsened at month 1 (P , 0.01) only after C-CXL; however, they improved significantly at month 12 compared with baseline (P , 0.05) in both groups. The demarcation line was visible in all cases at month 1 at a mean depth of 3026 56 mm and 311 6 57 mm after DAI-CXL and C-CXL, respectively (P = 0.7).
Conclusions: The DAI-CXL protocol seems as effective as the C-CXL protocol in halting KC progression after 1 year of follow-up.
Key Words: keratoconus, cross-linking, iontophoresis, diluted alcohol (Cornea 2017;36:1492–1497)
K
eratoconus (KC) is a bilateral progressive corneal ectatic disorder resulting in corneal thinning and visual impair-ment.1 Corneal collagen cross-linking (CXL) was proposedby Wollensak et al2in 2003 for the management of mild to
moderate KC by halting its progression. This conventional corneal cross-linking (C-CXL) procedure referred as the Dresden protocol involves removal of corneal epithelium, instillation of riboflavin solution in 20% dextran every 3 to 5 minutes for 30 minutes (to achieve adequate stromal saturation with riboflavin), and irradiation of the cornea using a 365-nm ultraviolet A (UVA) light source with 3 mW/cm2
for 30 minutes with continued instillation of riboflavin drops every 5 minutes. Although this standard procedure is well established and effective, the primary postoperative compli-cations related to epithelium removal—mostly postoperative pain and discomfort and rarely corneal ulcers, infiltrates, haze, and scars—are the main concerns.3,4
Transepithelial (TE)-CXL was developed as a modified procedure in 2004 to avoid epithelial debridement, and, to date, several modified riboflavin solutions consisting of enhancers such as benzalkonium chloride, ethylenediamine-tetraacetic acid (EDTA), polyethylene glycol, lysine, NC 1059, Ricrolin TE, gentamicin, tetracaine, and 20% ethanol have been used to facilitate riboflavin penetration into the stroma.5–7However, it has been shown that all these TE-CXL
approaches are still less effective because of the insufficient riboflavin concentrations in the corneal stroma compared with the standard CXL protocol.8,9
Most recently, iontophoresis has been proposed as an alternative riboflavin delivery technique for TE-CXL, which allows intrastromal riboflavin diffusion through intact corneal epithelium using 1.0-mA electric current. Both ex vivo and in vivo studies showed promising results with the iontophoresis-assisted corneal cross-linking (I-CXL) technique compared with standard TE-CXL.10–12However, compared with standard epi-off CXL, I-CXL is still found to be less effective because of insufficient stromal riboflavin saturation.13,14
In this study, we describe a new CXL protocol using a combination of 2 enhancers, which are dilute alcohol (10% ethanol) and iontophoresis (DAI), to enhance riboflavin diffusion into the corneal stroma through intact epithelium. Received for publication April 27, 2017; revision received August 1, 2017;
accepted August 3, 2017. Published online ahead of print September 14, 2017.
From the *Department of Cornea, Gazi University Hospital, Ankara, Turkey; and†Department of Cornea, Ufuk University Hospital, Ankara, Turkey. The authors have no funding or conflicts of interest to disclose.
Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal’s Web site (www.corneajrnl.com). Reprints: Kamil Bilgihan, MD, Gazi Universitesi Tip Fakultesi Hastanesi, Goz Hastaliklari Anabilim Dali, Besevler, Ankara 06500, Turkey (e-mail: [email protected]).
We compared visual, topographic, tomographic, and aberro-metric results of this new CXL protocol (DAI-CXL) with the results of the C-CXL protocol.
MATERIALS AND METHODS
Patient Population
This retrospective, comparative study included patients with KC who underwent CXL treatment either with the standard epi-off protocol or the newly developed DAI pro-tocol at the Gazi University Hospital, Ophthalmology Depart-ment, Ankara, Turkey, between June 2013 and January 2016. Patients were treated with the C-CXL protocol until 2014, and after that, patients were treated with DAI-CXL (used as a new CXL protocol for all patients). Before the study, institutional ethical approval was obtained.
Inclusion and Exclusion Criteria
Patients who underwent CXL treatment either with the standard epi-off protocol or the newly developed DAI pro-tocol for progressive KC and had 1, 3, 6, and 12 months of follow-up after treatment were included in this study. Patients with a history of previous ocular surgery, herpetic keratitis, other ocular disease and inflammation, corneal opacities, pregnancy, oral estrogen treatment, and lactation were not included. Progressive KC was described as an increase in Kmax $0.75 D during the last 6 months, worsening in refractive astigmatism$0.75 D in the previous 12 months, or a decrease in central corneal thickness (CCT) by 30 mm or more in the previous 6 months.
Surgery Technique
All procedures were performed under topical anesthesia using 0.5% proparacaine hydrochloride (Alcaine; Alcon, Puurs, Belgium) just before treatment.
DAI-CXL Protocol
An alcohol dispenser was attached on the corneal surface, and 10% alcohol solution (ethanol) was applied for only 10 seconds; then, the alcohol solution was absorbed by dry sponges (Merocel). Then, the cornea was impregnated with 0.2% riboflavin 59 monophosphate sodium salt solution (Sigma-Aldrich-Buchs), which was prepared in the Immu-nology Department of Gazi University Medical School in a laminar airflow cabinet as follows. The 0.2 mm-filtered 10· stock solution of riboflavin in 9% NaCl was added to
autoclave-sterilized distilled water to obtain ready-to-use 0.2% riboflavin, 0.9% NaCl (pH 5.9) solution. No additional enhancer was added, and the ready-to-use solution was applied to the surgical area using a custom-made iontopho-resis device (Engineering Faculty of Gazi University and Yuratek Electronics and Medical Devices Company, Ankara, Turkey) that can provide 1-mA continuous current with a high-sensitivity power supply. The positive electrode was fixed on the malar bone on the ipsilateral side (of the same side of the eye) (Fig. 1A). The negative electrode within a 9-mm barrel was applied over the corneal surface andfilled with 0.2% riboflavin solution (Fig. 1B). The device was set at 1.0 mA for 10 minutes (after the electric current started, bubbles appeared on the negative electrode). The riboflavin solution was refreshed after 5 minutes to maintain a high riboflavin concentration in the barrel. At the end of the iontophoresis procedure, penetration of riboflavin into the corneal stroma and anterior chamber was confirmed by a slit-lamp examination and blue cobaltfilter (Fig. 1C). Corneal CXL was then performed by exposing the central 8.0-mm cornea to UVA irradiation of 365-nm wavelength (CXL-Vario; Peschke Meditrade GmbH, Huenenberg, Switzerland) at 9 mW/cm2power for 13.3 minutes,
with a total dose of 7.2 J/cm2. During UVA administration,
a balanced salt solution was applied on the fifth minute to avoid desquamation of the corneal epithelium due to dryness. Finally, topical 0.5% moxifloxacin (Vigamox; Alcon Inc, Fort Worth, TX) was applied, and a therapeutic contact lens (Acuvue Oasys; Johnson & Johnson Vision Care, Inc) was positioned.
C-CXL Protocol
Epithelium was removed mechanically, and the cornea was impregnated with 0.1% riboflavin suspended in dextran T500 20% solution (Ricrolin; Sooft Italia SP) for 30 minutes, refreshing every minute.2 Then, CXL was
performed by exposing the central 8.0-mm of the cornea to UVA light of 365-nm wavelength (CXL-Vario; Peschke Meditrade GmbH) at 3-mW/cm2 power for 30 minutes
(with riboflavin installation every 5 minutes), with a total dose of 5.4 J/cm2. At the end of the procedure, topical 0.5%
moxifloxacin was applied, and a therapeutic contact lens (Acuvue Oasys; Johnson & Johnson Vision Care, Inc) was positioned.
After the procedures, all patients received treatment including topical moxifloxacin 4 times daily for 1 week, unpreserved topical tear drops (Refresh; Allergan Inc, Irvine, CA) every 2 hours for 1 month, andfluorometholone acetate 0.1% (Flarex; Alcon Inc) 3 times daily for 1 month.
FIGURE 1. A, Application of 10% alcohol solution for 10 seconds and position of the positive electrode. B, Negative electrode within a 9-mm barrel and filled 0.2% riboflavin solution. C, Penetration of riboflavin into the corneal stroma.
Main Outcome Measures
Patient demographics, pre- and post-treatment (1-, 3-, 6-, and 12-month) uncorrected distance visual acuity (UCDVA), best-corrected distance visual acuity (BCDVA), topographic and aberrometric values [maximum K (Kmax), average K (Kavg), cylinder (Cyl), CCT, minimum corneal thickness (MCT), front and back symmetry indexes (SIf and SIb), front and back KC vertexes (KVf and KVb), Baiocchi Calossi Versaci index (BCV), anterior higher-order aberrations (HOAs), coma, and spherical aberrations] using Scheimpflug-Placido topography (Sirius; CSO, Scandicci, Italy), and the demarcation line using anterior segment optical coherence tomography (Heidelberg Engineering GmbH, Dossenheim, Germany) were recorded.
Statistical Analysis
SPSS Statistics 22.0 was used to calculate means and standard deviations for all variables. All data were reported as mean 6 SD. The Shapiro–Wilk W test was performed to confirm the normal distribution of the data before analysis. Changes from baseline in each group were analyzed using the paired-samples t test. The independent-samples t test was applied to assess the significance of differences between groups. Differences with P , 0.05 were considered statistically significant.
RESULTS
This study included 93 eyes of 80 patients who met the inclusion and exclusion criteria. Forty-six eyes of 40 patients (21 males and 19 females) underwent DAI-CXL and 47 eyes of 40 patients (22 males and 18 females) underwent C-CXL. The KC stage was graded according to the Amsler–Krumeich classification system.15
After DAI-CXL, the epithelium was intact and the therapeutic contact lenses were easily removed in all eyes on the first postoperative day, whereas in the C-CXL group, epithelial healing occurred within 2 to 3 days. None of the patients had infections, visually significant haze, or other complications during 12-month follow-up.
Table 1 shows the baseline characteristics of the patients, both groups were comparable (P . 0.05). Sup-plemental Tables 1 and 2 (SupSup-plemental Digital Content,
http://links.lww.com/ICO/A565) show the preoperative and postoperative visual, topographic, and aberrometric outcomes of the patients who underwent DAI-CXL and C-CXL, respectively.
Visual Acuity
Statistical analysis showed a significant improvement in UCDVA and BCDVA compared with baseline in both groups (P , 0.05). The DAI-CXL group showed a significant improvement in UCDVA and BCDVA at 3-month follow-up, whereas the C-CXL group showed a significant improve-ment in UCDVA (Fig. 2A) and BCDVA (Fig. 2B) after 6 months.
Topographic Results
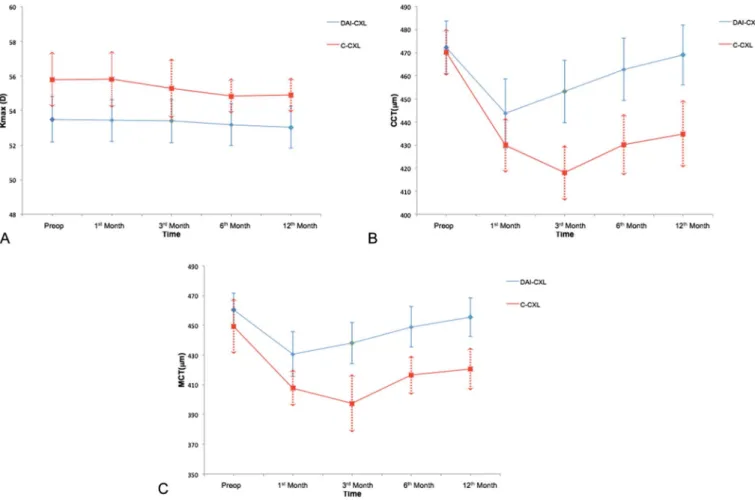
Topographic results for DAI-CXL and C-CXL are shown in Supplemental Digital Contents 1 and 2, respectively (http://links.lww.com/ICO/A565). Stabilization of keratome-try values (Kavg, Ks, and Kf) was achieved in both groups during 12 months of follow-up. A significant decrease of Kmax was observed after 6 months of follow-up in both DAI-CXL and C-DAI-CXL groups (Fig. 3A). SIf significantly improved in both DAI-CXL and C-CXL groups after 6 months of follow-up (P , 0.05), whereas the BCV significantly improved only in the DAI-CXL group at 12 months of follow-up. Other KC screening parameters (SIb, KVf, and KVb) remained stable throughout 12 months of follow-up in both groups.
Pachymetry Results
In the DAI-CXL group, MCT and CCT values decreased at month 1 (P, 0.001), and they started to recover after 3 months and reached baseline at 12-month follow-up (P . 0.05). In the C-CXL group, MCT and CCT values decreased at month 1 (P, 0.001), and they remained decreased compared with baseline during 12 months of follow-up (P , 0.001). Figs. 3B, C show the MCT and CCT values, respectively, in both DAI-CXL and C-CXL groups.
Tomographic Results
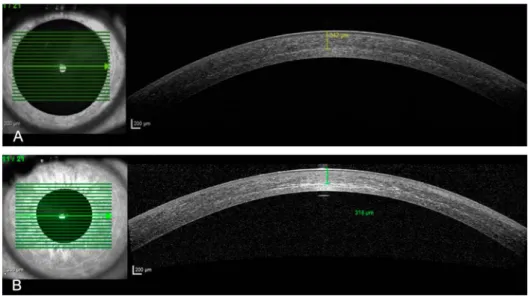
The corneal demarcation line was visible by anterior segment optical coherence tomography 1 month after surgery in all cases at a mean depth of 302 6 56 mm and 311 6 57 mm after DAI-CXL (Fig. 4A) and C-CXL (Fig. 4B), respectively (P = 0.7). The demarcation line was completely absent in all these patients 12 months after treatment.
Aberrometric Results
In the DAI-CXL group, aberrometric results showed a significant improvement in HOAs after 6 months and in coma and spherical aberration at 12 months compared with baseline (P, 0.05). However, in the C-CXL group, there was significant worsening in HOAs, coma, and spherical aberra-tion at the first month (P , 0.05), and they showed a significant improvement at the 12th month compared with baseline (P, 0.05).
TABLE 1. Baseline Characteristics of the Patients
Parameter DAI-CXL C-CXL P Age, yrs 24.06 5.6 22.06 5.1 0.66 KC grade 1.46 0.5 1.56 0.5 0.53 Kavg, D 46.96 2.7 47.96 3.1 0.24 Kmax, D 53.56 4.4 55.86 5.4 0.26 CCT,mm 472.36 37.8 470.16 34.5 0.54 MCT,mm 460.36 37.4 449.46 63.2 0.73 UCDVA (logMAR) 0.626 0.27 0.646 0.37 0.11 BCDVA (logMAR) 0.406 0.28 0.446 0.34 0.19
DISCUSSION
Achieving an adequate riboflavin concentration in the corneal stroma through intact epithelium is a subject under-going intense study. For this purpose, several new TE-CXL protocols are being developed with using different riboflavin formulas, UVA illumination levels, and frequencies or using the femtosecond laser to create a central corneal pocket for
superficial intrastromal administration of riboflavin without deepithelialization.7,16–19 Despite all these efforts, the
acquired intrastromal riboflavin diffusion level, which directly reflects CXL success,2 is not comparable to the
level acquired by the epi-off technique. In addition, this much diversity inevitably causes confusion on the way of finding the most effective and safe TE-CXL protocol.
FIGURE 2. UCDVA (A) and BCDVA (B) preoperatively and at 1, 3, 6, and 12 months after TE DAI-CXL (lower line) and C-CXL (upper line).
FIGURE 3. Maximum K (Kmax) (A) CCT (B), and MCT (C) preoperatively and at 1, 3, 6, and 12 months after TE DAI-CXL (lower line) and C-CXL (upper line).
With the introduction of iontophoresis in CXL, the barrier effect of epithelium against diffusion of riboflavin is expected to be minimized. Because riboflavin is a low-weight negatively charged molecule, iontophoresis could enhance its diffusion through epithelium to increase its stromal concentration and consequently could induce a good bio-mechanical effect. However, according to the literature, stromal riboflavin concentrations are still lower with I-CXL than with C-CXL.10,13 Therefore, researchers attempted to
increase the current and/or duration of iontophoresis or combine it with accelerated irradiation aiming at better re-sults.14,20They found that I-CXL could stop disease progression
24 months after the procedure but it is still less effective than C-CXL because of more superficial riboflavin concentrations.
After evaluating initial and promising I-CXL out-comes reported in the literature, we decided to apply iontophoresis-assisted CXL in our clinical practice with some modifications to achieve higher stromal riboflavin concentrations. We used enhancer-free 0.2% riboflavin solution with the guidance of our previous experimental study,21 in which the cornea was impregnated with 0.2%
riboflavin using iontophoresis and the 80% intrastromal concentration of the standard epi-off method was achieved. Moreover, we applied 10% alcohol solution for 10 seconds as an enhancer in the light of previous studies22,23 to
separate hemidesmosomal attachments and increase epi-thelial permeability. Then, we applied a total dose of 10 mA/10 minutes iontophoresis (DAI) for riboflavin diffusion and performed accelerated CXL with a total dose of 7.2 J/cm2
to compensate for the barrier effect of epithelium (in the light of previous clinical and laboratory studies that demonstrated that an energy dose of 7.2 J/cm2is effective and safe).24–26We
reported our preliminary, but encouraging, DAI-CXL results during the 34th ESCRS meeting in Copenhagen in 2016. In this study, we decided to compare the effectiveness of our new DAI-CXL protocol with that of the C-CXL protocol used for our patients with KC by evaluating their preoperative and postoperative visual, topographic, tomographic, and aberrometric outcomes.
Our results showed a significant improvement in the visual, topographic, and aberrometric parameters in both DAI-CXL and C-CXL groups during 12-month follow-up after treatment. We observed an earlier improvement in the UCDVA and BCDVA with DAI-CXL (after 3 months) compared with C-CXL (after 6 months), consistent with previous studies.16,19,27
Previous studies13,17,27 have shown that Kmax was
stable with I-CXL; however, we found that it decreased after 6 months in both DAI-CXL and C-CXL groups. Only 8.5% of eyes with C-CXL and no eyes with DAI-CXL progressed more than 1 D during 12 months of follow-up. Both DAI-CXL and C-DAI-CXL groups showed a significant improvement in the corneal symmetry index after 6 months of follow-up, consistent with a recent prospective study.27In addition, the
BCV significantly improved only in the DAI-CXL group at 12 months of follow-up. The BCV evaluates the presence and status of ectasia through analysis of the combination of corneal HOAs.28A significant improvement in the BCV at 12
months in the DAI-CXL group may be associated with a better improvement in KC.
We observed a significant decrease in CCT and MCT in the early postoperative period after both protocols. Nevertheless, they returned to preoperative levels 12 months after DAI-CXL, whereas they remained lower 12 months after C-CXL, consistent with a recent prospective study.27A
longer follow-up period is needed to assess the long-term results.
The demarcation line inside the corneal stroma is considered an indirect measurement of CXL penetration within the stroma, and it is normally observed at 1 month post-operatively.29Our results demonstrated that the demarcation line
was observed in all patients in both DAI-CXL and C-CXL groups at postoperative 1 month, and it was completely absent in all these patients 12 months after treatment. The mean depth of the demarcation line was also comparable between groups. However, in previous I-CXL reports, the demarcation line was more superficial and not measurable in most patients at 1 month postoperatively.13,14,17,30,31
FIGURE 4. Demarcation line 1 month after (A) TE DAI-CXL and (B) C-CXL.
HOAs have been shown to contribute to decreased visual acuity and contrast sensitivity in patients with KC. Studies have demonstrated a significant improvement mostly in coma after CXL treatment.32Some recent reports
compar-ing C-CXL with I-CXL showed worsencompar-ing in HOAs and coma at month 1 and improvement/stabilization after 6 to 12 months with both protocols. In this study, HOAs, coma, and spherical aberration values worsened at 1 month and improved at 12 months in the C-CXL, group consistent with the literature; however, in the DAI-CXL group, there was no significant worsening in HOAs, coma, and spherical aberra-tion at 1 month and a significant improvement observed in HOAs after 6 months, and in coma and spherical aberration at 12 months compared with baseline. This result may be attributed to the existence of intact epithelium in DAI-CXL. It has been stated in previous epi-off CXL studies that HOA worsening during early post-op period is related to the superficial corneal irregularity, superficial corneal edema and haze.33
Our results are limited by the retrospective design of the study and the relatively short-term follow-up (12 months). However, to the best of our knowledge, this is thefirst I-CXL study that uses enhancer-free 0.2% riboflavin solution as a photosensitizer, 10% alcohol solution as an enhancer, and a total dose of 7.2 J/cm2for UVA irradiation. Particularly, as
we observed, the epithelial problem (as being a barrier) of TE approaches seems resolved with the effect of dilute alcohol solution (10% ethanol for 10 minutes) on hemidesmosomal attachments and epithelial permeability.
In conclusion, the DAI-CXL protocol seems as effec-tive and safe as the C-CXL protocol in halting KC pro-gression. Furthermore, the relatively short overall treatment time and epithelial healing time may be considered as other advantages of the DAI-CXL protocol.
REFERENCES
1. Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42:297–319. 2. Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced
collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003;135:620–627.
3. Ghanem VC, Ghanem RC, de Oliveira R. Postoperative pain after corneal collagen cross-linking. Cornea. 2013;32:20–24.
4. Dhawan S, Rao K, Natrajan S. Complications of corneal collagen cross-linking. J Ophthalmol. 2011;2011:869015.
5. Raiskup F, Pinelli R, Spoerl E. Riboflavin osmolar modification for transepithelial corneal cross-linking. Curr Eye Res. 2012;37:234–238. 6. Zhang Y, Sukthankar P, Tomich JM, et al. Effect of the synthetic
NC-1059 peptide on diffusion of riboflavin across an intact corneal epithelium. Invest Ophthalmol Vis Sci. 2012;53:2620–2629.
7. Barbara R, Abdelaziz L, Barua A, et al. Collagen corneal cross-linking and the epithelium. Int J Kerat Ect Cor Dis. 2012;1:179–184. 8. Mastropasqua L. Collagen cross-linking: when and how? A review of the
state of the art of the technique and new perspectives. Eye Vis (Lond). 2015;2:19.
9. Wollensak G, Iomdina E. Biomechanical and histological changes after corneal crosslinking with and without epithelial debridement. J Cataract Refract Surg. 2009;35:540–546.
10. Cassagne M, Laurent C, Rodrigues M, et al. Iontophoresis transcorneal delivery technique for transepithelial corneal collagen crosslinking with riboflavin in a rabbit model. Invest Ophthalmol Vis Sci. 2016;57: 594–603.
11. Mastropasqua L, Nubile M, Calienno R, et al. Corneal cross-linking: intrastromal riboflavin concentration in iontophoresis-assisted imbibition
versus traditional and transepithelial techniques. Am J Ophthalmol. 2014; 157:623–630.
12. Bikbova G, Bikbov M. Transepithelial corneal collagen cross-linking by iontophoresis of riboflavin. Acta Ophthalmol. 2014;92:e30–e34. 13. Jouve L, Borderie V, Sandali O, et al. Conventional and iontophoresis
corneal cross-linking for keratoconus: efficacy and assessment by optical coherence tomography and confocal microscopy. Cornea. 2017;36:153– 162.
14. Bikbova G, Bikbov M. Standard corneal collagen crosslinking versus transepithelial iontophoresis-assisted corneal crosslinking, 24 months follow-up: randomized control trial. Acta Ophthalmol. 2016;94:600– 606.
15. Amsler M. Kératocône classique et kératocône frustre, arguments unitaires [in French]. Ophthalmologica. 1946;111:96–101.
16. Bottós KM, Schor P, Dreyfuss JL, et al. Effect of corneal epithelium on ultraviolet-A and riboflavin absorption. Arq Bras Oftalmol. 2011;74: 348–351.
17. Bouheraoua N, Jouve L, El Sanharawi M, et al. Optical coherence tomography and confocal microscopy following three different protocols of corneal collagen-crosslinking in keratoconus. Invest Ophthalmol Vis Sci. 2014;55:7601–7609.
18. Sorkin N, Varssano D. Corneal collagen crosslinking: a systematic review. Ophthalmologica. 2014;232:10–27.
19. Kanellopoulos AJ. Collagen cross-linking in early keratoconus with riboflavin in a femtosecond laser-created pocket: initial clinical results. J Refract Surg. 2009;25:1034–1037.
20. Lanzini M, Curcio C, Spoerl E, et al. Confocal microscopy evaluation of stromal fluorescence intensity after standard and accelerated iontophoresis-assisted corneal cross-linking. Int Ophthalmol. 2017;37: 235–243.
21. Novruzlu S, Türkcü UO, Kivrak I, et al. Can riboflavin penetrate stroma without disrupting integrity of corneal epithelium in Rabbits? Iontophoresis and ultraperformance liquid chromatography with electrospray ionization tandem mass spectrometry. Cornea. 2015; 34:932–936.
22. Gabler B, Winkler von Mohrenfels C, Dreiss AK, et al. Vitality of epithelial cells after alcohol exposure during laser-assisted subepithelial keratectomyflap preparation. J Cataract Refract Surg. 2002;28:1841– 1846.
23. Wang Y, Tong J, Chang B, et al. Effects of alcohol on intestinal epithelial barrier permeability and expression of tight junction-associated proteins. Mol Med Rep. 2014;9:2352–2356.
24. Moramarco A, Iovieno A, Sartori A, et al. Corneal stromal demarcation line after accelerated crosslinking using continuous and pulsed light. J Cataract Refract Surg. 2015;41:2546–2551.
25. Mazzotta C, Moramarco A, Traversi C, et al. Accelerated corneal collagen cross-linking using topography-guided UV-a energy emission: preliminary clinical and morphological outcomes. J Ophthalmol. 2016; 2016:2031031.
26. Medeiros CS, Giacomin NT, Bueno RL, et al. Accelerated corneal collagen crosslinking: technique, efficacy, safety, and applications. J Cataract Refract Surg. 2016;42:1826–1835.
27. Vinciguerra P, Romano V, Rosetta P, et al. Transepithelial iontophoresis versus standard corneal collagen cross-linking: 1-year results of a pro-spective clinical study. J Refract Surg. 2016;32:672–678.
28. Safarzadeh M, Nasiri N. Anterior segment characteristics in normal and keratoconus eyes evaluated with a combined Scheimpflug/Placido corneal imaging device. J Curr Ophthalmol. 2016;28:106–111. 29. Seiler T, Hafezi F. Corneal cross-linking-induced stromal demarcation
line. Cornea. 2006;25:1057–1059.
30. Bonnel S, Berguiga M, De Rivoyre B, et al. Demarcation line evaluation of iontophoresis-assisted transepithelial corneal collagen cross-linking for keratoconus. J Refract Surg. 2015;31:36–40.
31. Vinciguerra P, Randleman B, Romano V, et al. Transepithelial iontophoresis corneal collagen cross-linking for progressive keratoconus: initial clinical outcomes. J Refract Surg. 2014;30:746–753.
32. Muzychuk A, Penner V, Rocha G. High order aberration outcomes of corneal collagen crosslinking in eyes with keratoconus and post-LASIK ectasia. Int J Kerat Ect Cor Dis. 2014;3:107–112.
33. Abbondanza M, Abdolrahimzadeh B, Zuppardo M, et al. Refractive changes following CXL. Cataract Refract Surg Today Europe. 2009;4: 33–38.