HEALTH WORKERS IN TURKEY
SEVİLAY SİTRAVA-GÜNENÇ
107629012
İSTANBUL BİLGİ ÜNİVERSİTESİ
SOSYAL BİLİMLER ENSTİTÜSÜ
KLİNİK PSİKOLOJİ YÜKSEK LİSANS PROGRAMI
YARD. DOÇ. DR. MURAT PAKER
2010
Betimleyici Çalışma: Türkiye’deki Ruh Sağlığı
Çalışanlarının Profesyonel ve Sosyo-kültürel
Profilleri
Sevilay Sitrava-Günenç
107629012
Yard. Doç. Dr. Murat Paker
: ...
Yard. Doç. Dr. Ayten Zara
: ...
Yard. Doç. Dr. Özlem Sertel-Berk : ...
Tezin Onaylandığı Tarih
: 15.09.2010
Toplam Sayfa Sayısı: 198
Anahtar Kelimeler
Key Words
1) Ruh sağlığı
1) Mental health
2) Ruh sağlığı çalışanları
2) Mental health workers
3) Profesyonel profil
3) Professional profile
4) Sosyo-kültürel profil
4) Socio-cultural profile
Thesis Abstract
A Descriptive Study: PROFESSIONAL AND SOCIO-CULTURAL PROFILES OF MENTAL HEALTH WORKERS IN TURKEY
Sevilay Sitrava-Günenç
The main purpose of the study was to describe the mental health workers in Turkey in terms of four aspects, which were socio-demographic
characteristics, educational background, professional information, and political and religious related social identities. A sample of 245 mental health professionals, consisting of psychologists, psychiatrists,
psychological counselors, clinical psychologists and clinical psychology MA students filled out the questionnaire. Two methods were utilized. The public link of the questionnaire was sent to the major email groups in which mental health workers were the members. Via the link, the purpose and the content of the study were stated. In addition, the questionnaire was
converted into a hard copy, and then distributed to major hospitals, psychological counseling centers, and private psychotherapy clinics in Istanbul. The findings displayed detailed information about the mental health workers in terms of five groups. These were socio-demographic characteristics, educational and training background, experience related
characteristics, client related characteristic and proposed interventions. The study further investigated factors that predict healing in clients, drop-out rates and reasons, proposed primary interventions, and difficulties experienced by professionals with different cases. Lastly, limitations and implications for further studies were discussed.
Tez Özeti
Betimleyici Çalışma: TÜRKİYE’DEKİ RUH SAĞLIĞI ÇALIŞANLARININ PROFESYONEL VE SOSYO-KÜLTÜREL
PROFİLLERİ
Sevilay Sitrava-Günenç
Bu çalışmanın temel amacı, Türkiye’deki ruh sağlığı çalışanlarını, sosyo-demografik özellikler, eğitim geçmişi, profesyonel bilgiler ve politika ve dinle ilişkili sosyal kimlikler olmak üzere dört açıdan betimlemektir. Araştırma anketini, psikolog, psikiyatrist, psikolojik danışman, klinik psikolog ve klinik psikoloji yüksek lisans öğrencilerinden oluşan toplam 245 kişi doldurdu. İki yöntem kullanıldı. Anketin linki, ruh sağlığı çalışanlarının üye olduğu e-posta gruplarına gönderildi. Bu linkte, ayrıca çalışmanın içeriği ve amacı belirtildi. Buna ek olarak, anketin basılı kopyası hazırlanarak, İstanbul’daki belli başlı hastanelere, psikolojik danışmanlık ve psikoterapi merkezlerine gönderildi. Araştırmanın sonuçları, ruh sağlığı çalışanlarının beş ayrı gruptaki detaylı bilgilerini göstermektedir. Bunlar, sosyo-demografik özellikler, eğitim geçmişi, deneyimle ilişkili özellikler, danışanlarla ilişkili özellikler ve önerilen müdahalelerdir. Ayrıca, bu çalışma danışanlardaki iyileşme oranını, klinik tedaviyi yarıda bırakma oranı ve sebeplerini, önerilen birincil müdahaleleri, farklı vakalarla
çalışırken profesyonellerin yaşadığı zorluk derecelerini yordayan faktörler incelenmiştir. Son olarak, çalışmanın kısıtlılıkları ve gelecek araştırmalara dair öneriler tartışılmıştır.
Acknowledgements
I owe many thanks to everyone who made contributions and provided support during my thesis process.
Firstly, I would like to express my deepest gratitude to my thesis advisor Assist. Prof. Murat Paker for his invaluable help and contibution. Although he had an extremely heavy schedule, he was supportive and encouraging me in this process. He was always accessible and ready to answer my questions. I felt his cooperation and support deeply. I owe him a great deal for his valuable guidance, trust, encouragement and time.
I thank to committee member Assist. Prof. Ayten Zara for her openness to help and trust in me. I am also grateful to the other committee member Assist. Prof. Özlem Sertel-Berk for her invaluable enthusiasm and constructive criticisms. Her feedbacks and suggestions immensely enhanced my motivation for further research.
I would like to express my great thanks to Prof. Doğan Şahin, Assoc. Prof. Levent Küey, Dr. Zeynep Çatay, Neşe Hatiboğlu, Hejan Epözdemir, Ege Ortaçgil, Billur Kurt, and Ebru Sorgun for their valuable contributions and generous helps in data collection process. Without their support, it was impossible to gather expected amount of data.
I owe special thanks to Yavuz Erten for believing, supporting, and his invaluable contribution to my improvement in professional life.
I would like to express my special thanks to Assoc. Prof. Hanna Nita Scherler for her invaluable encouragement and contributions to my
occupational life. I am also thankful for her help and support during data collection of this study.
I am very thankful to Alev Çavdar for her invaluable contributions to share new and different ideas and help for data analysis, greatest support, providing motivation and openness for any question during thesis process.
I would like to express my thanks to Ezgi Soncu for being such a wonderful project partner and giving support during data collection and analyses.
I am very thankful to my business friends in Mezura for their support, disburdening my mind in spite of busy time schedule and intense work.
I express my greatest thanks to Simge Çelikoğlu for her faithful friendship, always being with me, sharing everything in both bad and good times.
I have the deepest gratitude to Behzat Cem Günenç for coming into my life. I feel myself lucky to have the unconditional love and emotional support he has given me in life. He always makes me feel understood, cared, and loved. I am very thankful to him to help me overcome the unbearable times, stressful occasions, believing and trusting me in every moment of life. I love you...
Finally, I would like to thank to my father, Aygün Sitrava who made all the possible contributions for my career, relational, and educational development in life. I am very thankful to my elder brother Kubilay Sitrava, who always shared his constructive criticisms with me, and inspired me in
life. I have special thanks to my mother, Arzu Sitrava, who is in the sky, for her invaluable caring, support, exertion and love from the first day of my life. I love you all... I would like to dedicate this thesis to my parents and my brother, who have always made me feel whole.
Table of Contents
Title Page………...i
Approval………...ii
Thesis Abstract ... ……….…. ....iii
Tez Özeti ... v Acknowledgements ... vii Table of Contents...x List of Tables...xiii 1. Introduction...1 1.1. Literature Review...2 1.1.1. What is health?...2
1.1.2. What is mental health? ...3
1.2. Mental health services in general... ...4
1.2.1. History of mental health services in general...4
1.2.2. The diversity of mental health in general...8
1.2.3. The importance and function of mental health ... 10
1.3. Mental health service in Turkey...13
1.3.1. History of evolution of mental health service...13
1.3.2. Demographic information of mental health workers...15
1.3.3. Occupational features of mental health workers...16
1.3.3.1. Work settings...16
1.3.3.2. Experience years...17
1.3.3.4. Professional and academic profiles of the mental health
workers...20
1.3.3.5. Personal psychotherapy for the mental health workers...21
1.3.3.6. Political and religious views of the mental health workers...22
1.4. Research Questions and Explorations...23
1.4.1. Research Questions...23
1.4.2. Explorations...23
2. Method...25
2.1. Participants...25
2.2.Instruments...30
2.2.1. Questionnaire for the mental health workers...30
2.3. Procedure...32
2.4. Data Analyses...33
3. Results...35
3.1. Descriptive Analyses...35
3.1.1. Socio-demographic characteristics...35
3.1.2. Educational and training background...43
3.1.3. Experience-related characteristics...59
3.1.4. Client-related characteristics...84
3.1.5. Proposed interventions...106
3.2. Results of Multiple regression analyses...116
4. Discussion...123
4.2. Limitations of the current study and recommendations for future research...146 References...148 Appendices...153
List of Tables
Table1. Demographic characteristics………..26
Table 2. Characteristics of occupation, educational level, and work setting………..28
Table 3. Socio-demographic characteristics………...37
Table 4. Social identities of mental health professionals………...41
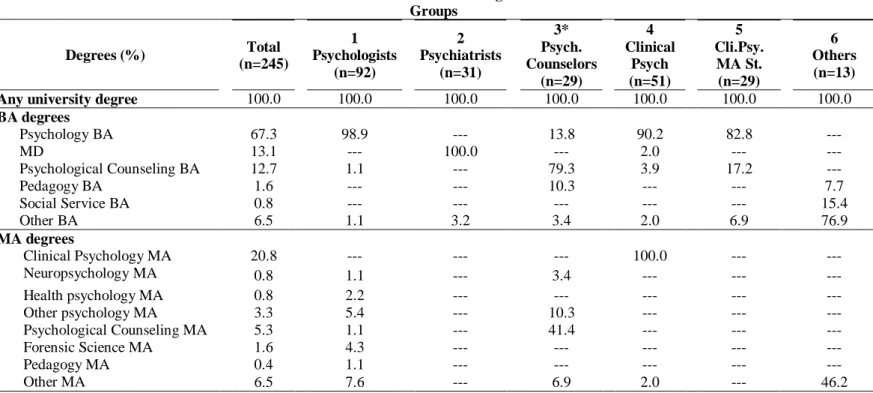
Table 5. Educational background………...45
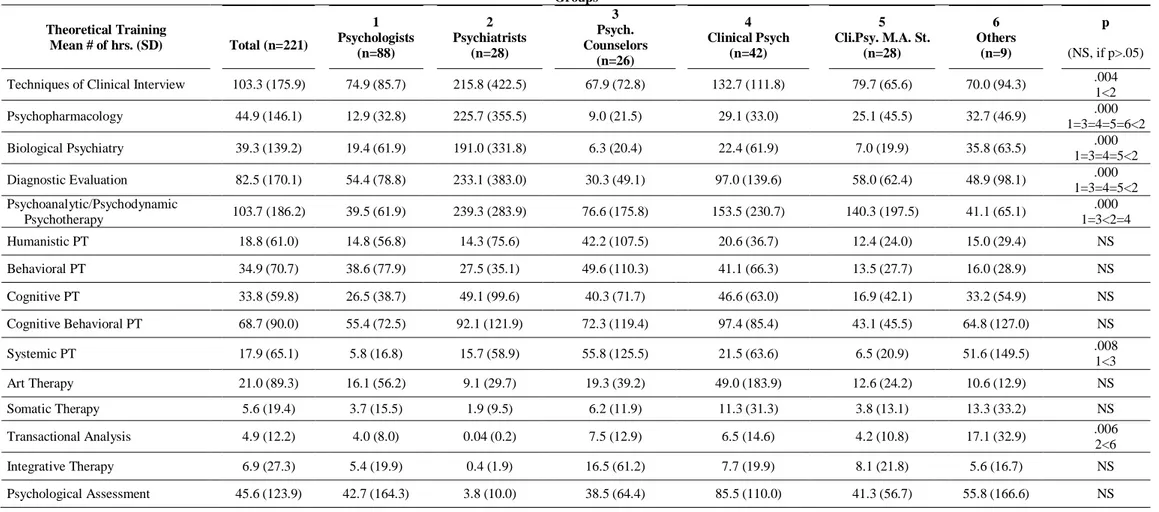
Table 6. Total number of hours in theoretical training based on clinical subfields………..49
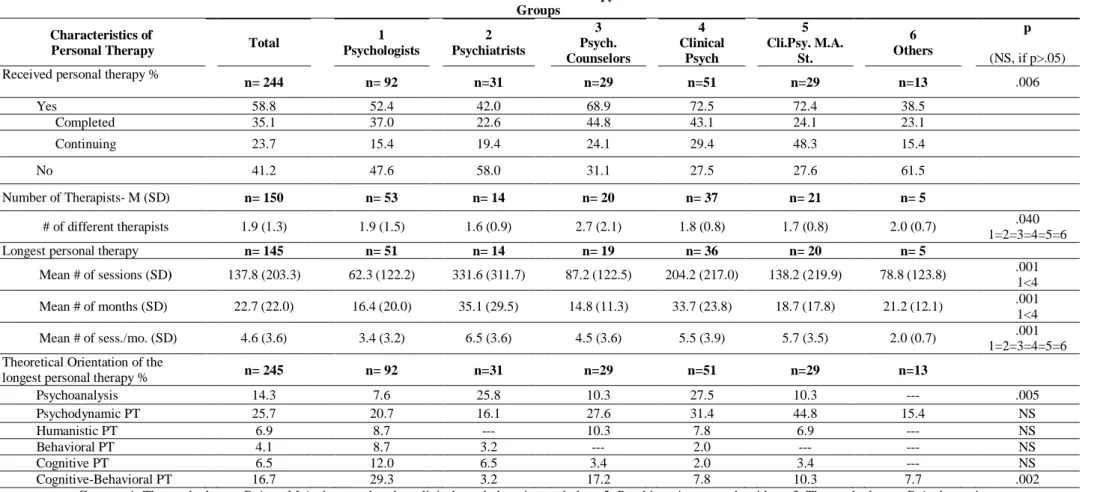
Table 7. Personal therapy………...52
Table 8. Type of materials read by the professionals……….54
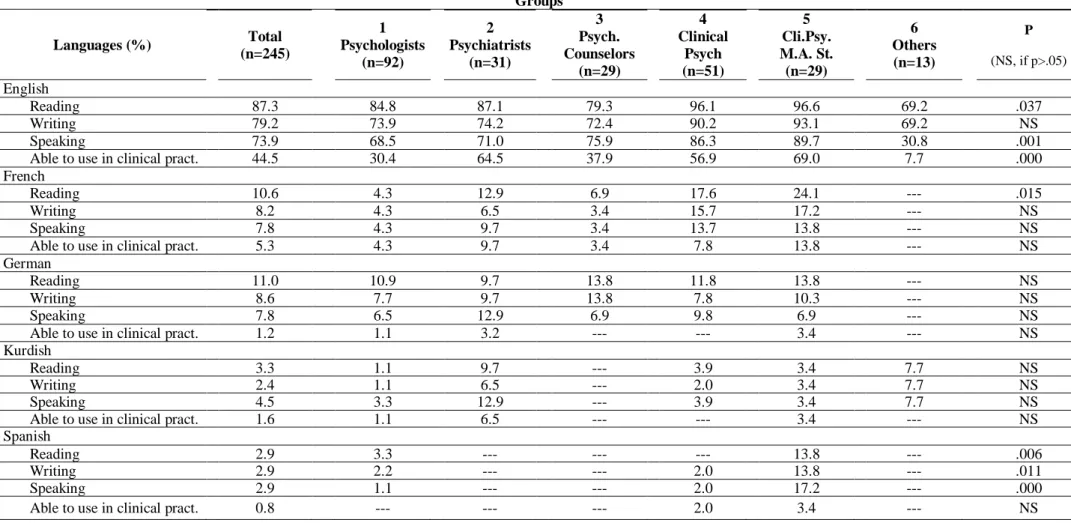
Table 9. Knowledge of second language other than Turkish………57
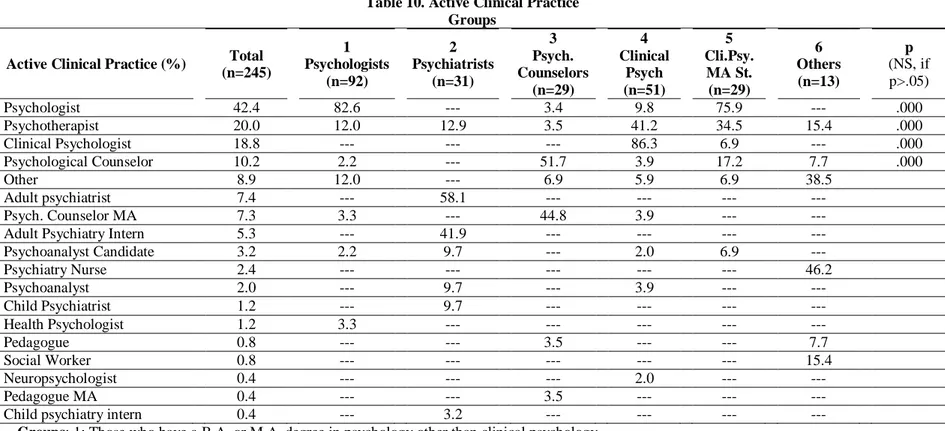
Table 10. Active clinical practice………...61
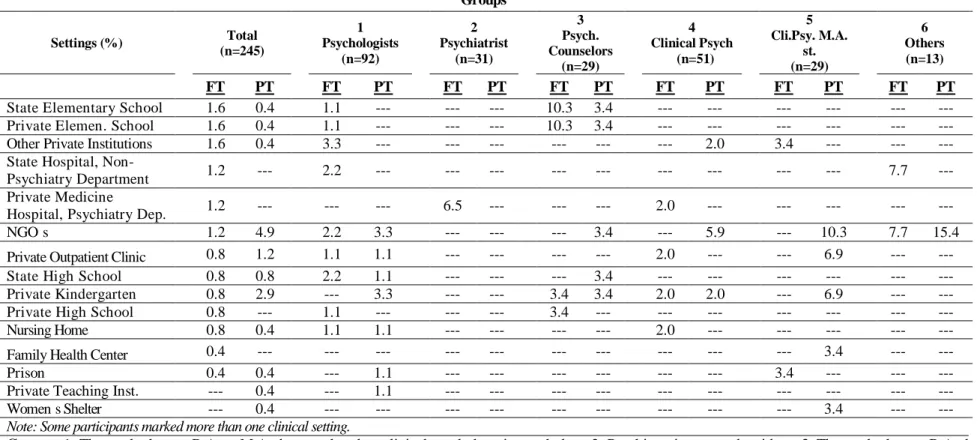
Table 11. Clinical Work Settings………63
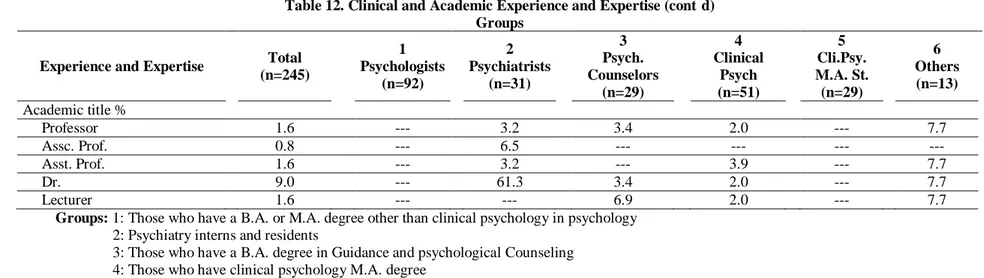
Table 12. Clinical and Academic Experience and Expertise…………..67
Table 13. Distribution of the type of clinical practice………71
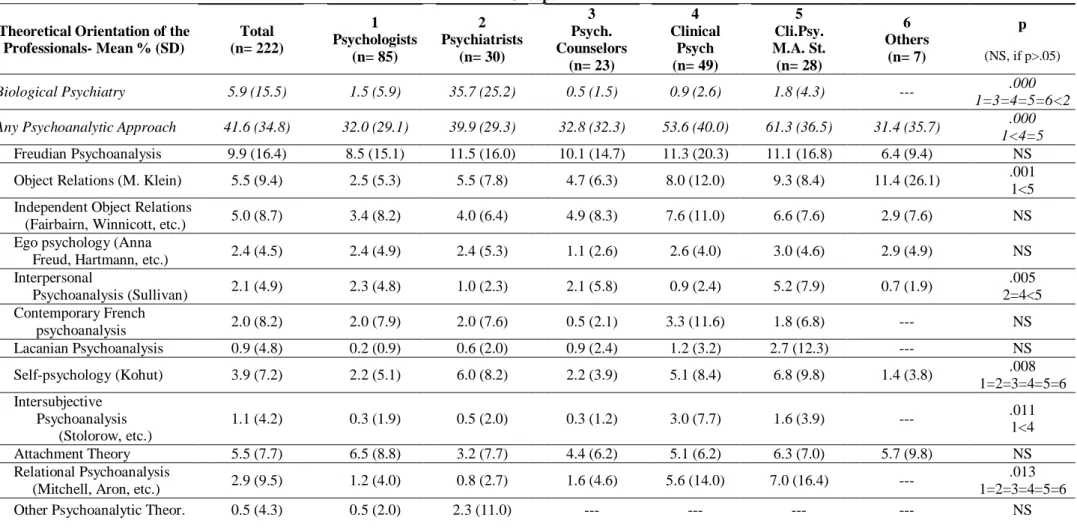
Table 14. Distribution of theoretical orientation of the professionals………...74
Table 15. Degrees of difficulty with different cases………...80
Table 16. Degrees of satisfaction in different professional dimensions………..83
Table 18. Drop-out rates……….89 Table 19. Reasons for drop-outs……….91 Table 20. Self-estimated degrees of healing due to clinical
interventions………...94 Table 21. Distribution of previous experience with
clinicians……….96 Table 22. Degrees of the factors achieving permanent therapeutic
development………..101 Table 23. Number of cases mental health professionals have attended to………...105 Table 24. Mental health professionals’ proposed types of primary interventions for the people who experience psychological difficulties in
Turkey………...108 Table 25. Mental health professionals’ proposed types of primary
clinical interventions for the people who experience psychological
difficulties in Turkey………110 Table 26. Mental health professionals’ proposed types of secondary clinical interventions for the people who experience psychological
difficulties in Turkey………112 Table 27. Mental health professionals’ proposed types of psychotherapy for the people who would benefit from psychotherapy………115 Table 28. Summary of stepwise multiple regression analysis for
Table 29. Summary of stepwise multiple regression analysis for variables predicting the percentage of clients completed the clinical service in appropriate time………118 Table 30. Summary of stepwise multiple regression analysis for
variables predicting the percentage of drop-outs mostly due to the
clinician……….119 Table 31. Summary of stepwise multiple regression analysis for
variables predicting the percentage of drop-outs due to the mismatch of theoretical orientation and client’s problems/needs……….119 Table 32. Summary of stepwise multiple regression analysis for
variables predicting the percentage of clients for whom professionals proposed getting help from a mental health professional for the people who experience psychological difficulties in Turkey as primary
intervention………...120
Table 33. Summary of stepwise multiple regression analysis for variables predicting the percentage of clients for whom professionals proposed psychotherapy as primary clinical intervention for the people who experience psychological difficulties in Turkey………...121 Table 34. Summary of stepwise multiple regression analysis for
variables predicting total level of difficulty mental health professionals experience in performing their clinical work………122
Appendices
Appendix A: The Questionnaire of the Study……….153 Appendix B: Table 4. Social identities of mental health
professionals………...172 Appendix C: Table 7. Personal therapy………..176 Appendix D: Table 9. Knowledge of second language other than Turkish………179
CHAPTER I. INTRODUCTION
The field of mental health has been given more importance in the last two decades by health sector professionals, such as medicine doctors, nurses and dieticians, and lay people in Turkey. The mental health is considered with the body health together. It is almost impossible to detach the body and mind pair. This couple is implied that human’s health is formed by being both “mentally hygiene” (Kraft, 2009), and also bodily.
Mental health is conceived of as a complete state in which
individuals are free of psychopathology and flourishing (Keyes, 2002) with high levels of emotional, psychological, and social well-being. The rising importance of mental health field brings the inquiry about the field in details. By whom this field is comprised of in Turkey, the specialties of these professionals will be the first step of defining the mental health field in Turkey.
Hence, in this study, the mental health workers will be described in terms of many characteristics, such as demographic information,
professional profiles, and socio-cultural profiles. By defining the descriptive features of mental health workers, the current picture of the field will be
seen. This will enable to learn who works as a mental health worker, in which setting one works, of which academic and professional educations one has, and etc.
In this research, mental health professional and socio cultural profiles of mental health workers in Turkey will be described. Who the mental health workers are, what kind of identifying variables they have, political, socio cultural views of professionals, which field of study they graduate, which educational programs they undergo, personal therapy for professionals, which theoretical orientation they are capable of and prefer to use are the main points of the study.
In addition to the description of the mental health sector in Turkey, this study presents the explorative statements about the mental health field in Turkey and the characteristics of the professionals. Therefore, the effective variables of the mental health field will be explored.
1.1. Literature Review 1.1.1. What is Health?
Health is the most crucial condition for every living thing, in order to exist and survive. For human beings’ health brings some other needs with itself. Physical needs are the formerly ones, which make human beings’ life more livable. Being sheltered, nourished with both food and water, having air are the indicators of the fact that human beings are provided physical needs to survive. Then, as Maslow (1987) mentions in the theory of needs of hierarchy feeling safe and secure is the second step to be provided, in
addition to physical needs. These needs are the first ones that form body health. Besides body fitness, health has one more important component enabling human beings live, which is mental health.
World Health Organization (WHO, 2006) defined health as being “a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity” (p. 1). Thus, one’s health cannot be
considered as only one part, like physically, but also mental health and social well being are the other complementary parts of health.
1.1.2. What is Mental Health?
One important component of health is mental health, which is a term used to describe either a level of emotional well being or an absence of a mental disorder as a psychopathology (Keyes, 2005). World Health Organization defines mental health as "a state of well-being in which the individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a
contribution to his or her community” (WHO, 2005, p. 1). Mental health includes perception, cognitive schemas, coping mechanisms, socially wellness, and emotions. These form all human beings mentally. As Keyes (2002) defines mental health which is a positive functioning constituted by the subjective wellness, including one’s perceptions, and one’s evaluations of life in terms of quality and the effectiveness. Thus, mental health has a role to determine one’s behaviors, cognition, social interactions, and etc.
As mentioned above, health can be considered neither without mental health nor without physical or psychosocially health. From a holistic perspective, they all interact with one another, and contribute to one’s daily life. If a human being feels disturbance in one’s body, one may immediately want to get help from a medicine doctor. In addition, if one becomes to have a problem with an acquaintance, one generally may get in contact with the other party to solve their problem. Yet, when a human being feels a
problem, one may not know how to overcome the problem, or get help from a professional being from a mental health service.
1.2. Mental Health Services in General 1.2.1. History of Mental Health Services in General
Mental health field stands for a variety of services. In general all around the world, this sector includes psychopharmacological treatment, psychotherapy, psychological counseling, pedagogical support,
rehabilitation works and etc. These all deal with the human beings’
psychological wellness, behaviors, hormone levels, and/or perceptions etc. In Europe, during the Middle Age period, mental health was
concerned with insanity, as a mental disorder, instead of one’s health as a whole. In England, a public hospital being the largest one in those years was built in 1744, in order to deal out with insanity (Jones, 1972). The hospital, named Bethlem, became the one of the most crucial parts of National Health Service in the year of 1948 (Jones, 1972). During those times, only the people with “impotent poor” (p. 18) condition, being not able to work and
provide one’s own physical needs, were treated, any other kinds of mental illness were not even taken into consideration.
In many other societies, spiritual or religious explanations dominated the methods within which people with mental disorders had been treated for decades. Then in the seventeenth century, the illness of madness was
explained as a physical state (Funk, Saraceno, & Pathare, 2003). A huge amount of “impotent poor” (Jones, 1972, p. 18) people had been confined in poorhouses, public prisons, workhouses or general hospitals in Europe and in the North America during 1600’s and 1700’s (Goodwin, 1997). These people were named as “subhuman” (Funk, Saraceno, & Pathare, 2003, p. 17) who were believed as incurable patients, and physically restrained in terms of confinement. During the eighteenth century, people being mentally disturbed were being used to check the living conditions whether they were poor or not.
With the improvement of humanitarian attitude, during the
eighteenth century, some reforms were needed to cure mentally disturbed people. In order to serve to this aim, many institutions developed more different treatment programs, being more moral (Breakey, 1996). This perspective of moral treatment programs led to the constructions of many other shelters both in the United States and European countries. Yet, there became also some other problematic in this model of treatment in the huge, public institutions. These were financial restrictions, and huge amount of people who applied to those institutions. Eventually, these public
institutions became the institutions providing only protection and care to mentally restricted human beings (Funk, Saraceno, & Pathare, 2003).
During the twentieth century, there became a change in custodial programs, emphasizing only protection and care services. More emphasis occurred in treatment of people being mentally restricted, which was a more humane perspective (Funk, Saraceno, & Pathare, 2003). By the end of World War II, human rights had been more evolved and these prospering movements focused more on the defeat one’s human rights. It was adduced that in the asylums, there were poor living conditions, caring and treatment programs were not enough and humanistic. Thus, human rights were violated in these institutions which were for the human beings, who were mentally restricted. In order to overcome this problem, the movement of deinstitutionalization had emerged (Anthony, 1993).
Deinstitutionalization stood for the processes of decreasing the number of chronically mentally restricted patients, who stayed in the state mental hospitals, minimizing and shutting down some amount of hospitals. Instead of these institutions, some other mental health services had been developed (Anthony, 1993). Since mental disorders might have some kinds of needs and demands, in terms of vocation, residency, education, and social interactions, alternative community- based settings had been developed. Towards the mid 1970’s, in the States, the National Institute of Mental Health had promoted an idea of a system which was community supportive one (Turner & TenHoor, 1978). This community supportive system
restricted. In other words, these mentally ill people were assisted to meet their needs and enhance the potentialities without excluding from the community (Anthony, 1993).
In the European countries, such as in Italy, mental hospitals were also closed and instead of those, community-based services which were providing psychosocial rehabilitation, medical care and treatment for emergency circumstances (Funk, Saraceno, & Pathare, 2003). Moreover, these community-based services became more common in other countries and cities around the world such as Melbourne in Australia, Santos in Brazil, Lile in France, Madrid in Spain, and London in the United Kingdom (Funk, Saraceno, & Pathare, 2003).
Yet, then deinstitutionalization had been found inadequate, because this process was a complex one including implementations of the alternative supportive programs out of the mental hospitals (Funk, Saraceno, & Pathare, 2003). These alternative programs for the community health were believed cost effective, especially for the chronic patients who needed to stay in the hospitals. Then, it was realized that with the adequate budget and human resources service, community-based services might be established, without accompanying deinstitutionalization (Funk, Saraceno, & Pathare, 2003). In some developing countries, psychiatric hospital services which were the basic ones were improved and also some other psychiatric units were being established (Kilonzo & Simmons, 1998). In addition, there were some other hospitals which integrated the basic mental health services with the general
health services with the help of training the professionals to give the primary care in mental health (Kilonzo & Simmons, 1998).
With the coming of the 21st century, more significant improvements for the treatment of people who had mental disorders have been occurred. With the progress in social sciences, in treating the mental health,
psychological and psychosocial aspects have been taken into consideration (Funk, Saraceno, & Pathare, 2003). Eventually, mental health workers have the chance to reach more effective treatment programs for the people with mental disorders.
1.2.2. The Diversity of Mental Health Service in General
In 1980’s classification of the results of illnesses, World Health Organization has defined the services of mental health field such as
treatment, crisis intervention, case management, rehabilitation, enrichment, rights protection, basic support and self-help (Anthony, 1993). These are the service categories that help the people suffering from mental disorders.
Treatment was effective to reducing the intensity of symptoms in order to relieve from the symptoms which might make the human beings distressed. Crisis intervention was used for controlling and solving one’s problems which might be dangerous and/or critical. With this kind of help, people with mental health illness were intended to provide personal safety. The other type of mental health service was named as case management. It was the service that planned to obtain the important and necessary services for the people with mental illness, which were their needs and desires. The
outcome of this service was to access the care giving of the service (Anthony, 1993).
Rehabilitation was the other service category. The aim of this service was to develop skills of mentally restricted people and support them to achieve their goals in life. This eventually was expected to improve role functioning for those people. In order to provide self-development for the people suffering from mental illnesses, there was the service called as enrichment. It was planned to engage the patients in the activities which are suitable and satisfying for them. The other type of services was that rights protection. It was aimed to provide equal opportunity for the people being mentally restricted. Thus, the aim of this service was to advocate and upgrade one’s rights in this field.
In addition, there was the other basic support service type. This was planned to assure personal survival, by providing human beings places, and needs which are required for survival, such as shelter, food, and health care. The last type of mental health services was named as self-help. This kind aimed to provide empowerment for the people themselves. This occurred with exercising a voice and choosing an alternative in one’s own life (Anthony, 1993).
In those years, 1980’s, mental health services for the people who needed special treatment program being suitable for one emphasized on not only mental impairments or relieving symptoms, but also functional
limitations which are significant in one’s life, disabilities, and handicaps for the one (Anthony, 1982). Thus, the treatment became effective in one’s
whole life, in terms of such as employment, social interactions, and self-determination.
In recent times, mental health field has been more dealing with the human beings as a whole as mentioned above. People who have some kinds of problems either about mentally or socially or emotionally, in whatever settings, they are helped by the professionals. The professional help may differ according to the needs and purposes of an individual, having a problem. Both the kind of service category and the settings may depend on the individuals and/or problems. The mental health services may be given by a psychiatrist, psychologist, counselor, consultant, doctor, school
counselor, and/or a member of a family. The settings may also be a hospital, school, and/or home.
1.2.3. The Importance and Functions of Mental Health Services in General
According to the number of publications in each year, it has been obvious that mental health services have become more common in the last two decades (Safran, Mays, Huang, McCuan, Pham, Fisher, McDuffie, & Trachtenberg, 2009). Around the world, mental health care systems have spread out largely. Since there have been different types of mental health services, the prevalence of utilization of service categories may differ according to the countries, or needs, wants of the people looking for a mental health service.
In the United States, mental health services have mostly taken place in terms of social variables, such as employment, housing, and income
(Safran et al., 2009). These kinds of circumstances for one’s life may be significant enough to define mental health. Eventually, in the field of mental health, human beings are aimed to provide the mental health service in terms of improving and/or exploring one’s social traits. Moreover, the mental health services may also be utilized in terms of psychometric assessments. Yet, it has been found out (Safran et al., 2009) that
psychometric values may depend on the racial and/or cultural differences. Thus, the values may be different in culture to culture, and this may not be valid for all the populations.
In the Far East, such in China, mental health issues have been seen within the family dynamics (Lim, Lim, Michael, Cai, & Schock, 2010). Since in China, collectivism has been the significant characteristic for the society, even the problems for one person has been dealing in a matter of collectivism. Eventually, resolving a problem or a situation for an individual has been seen with the family as a whole (Lim et al., 2010). In addition, individual psychotherapy is currently available, even though being limited. Individual psychotherapy from specialized professional is also very limited, being available in mostly the urban settings.
For those of the reasons, the professionals suggest to study in a different way, by both including the community as a whole and improving techniques for personal therapies. As soon as the works for the community would provide immediate resolving types in a society, and/or the ability to anticipate the possible problems, and behave in accordance with that. For these reasons, prevention studies are planned to study in the near future in
China (Lim et al., 2010). Moreover, in order to develop the effectiveness of personal psychotherapy, more sufficient and theoretical intervention
techniques are planned to involve in the mental health services (Lim et al., 2010).
In Europe, such in the United Kingdom, primary care in terms of mental health is conceived at schools. Since there has been a rise in the rate of school leaving in UK, especially in Wales for a few years, emotional health care has been the uprising point of view in schools (Terry, 2006). Leaving a school may point or stand for an intensive feeling, as a result of an experience that the student has lived at home, or school, or etc. Yet, the contribution place of those feelings has become the schools. The reasons for this may be being illiterate in terms of emotions, or having a limited
emotional repertoire to express oneself. Eventually, mental health services are believed to become widespread especially in schools, where is the best community place to reach large amounts of people, at school ages (Terry, 2006).
In Canada, mental health services have been mostly given by the psychiatrists. They have been giving people, who needed mental health service, mostly medical treatment, by utilizing psychiatric medication (Kolodny, 2007). In addition to higher prevalence of medication by the psychiatrists in Canada than the other mental health care systems,
psychiatrists have also played an administrator role for the well being of the society, as a whole. They are given both the role of a doctor, and also the
role of the administrator, who organizes and/or modifies mental health policies, and supplies indirect commune services (Kolodny, 2007).
1.3. Mental Health Service in Turkey 1.3.1. History of Evolution of Mental Health in Turkey
The mental health has been given importance since the Seljuk and Ottoman periods (Gökalp & Aküzüm, 2007). In the East part, psychotic people were thought to be sinless, and assumed to be closer to God. With that reason, for those individuals with psychosis were given much more respect. By the era of healing, new buildings had also constructed in case the individuals diagnosed with mental illness were able to be cured, in the teaching hospitals (Gökalp & Aküzüm, 2007). Then, asylums were built for those mentally ill people to treat them with music and flower-scented baths (Bayülkem, 2002).
The financial support for these developments had been taken by agricultural, artisan, craftsman works till the Ottoman Empire (Gökalp & Aküzüm, 2007). These artisans’ works had played important roles in terms of social security organizations, so that the members of the organizations could have given financial support. With these support, asylums were built in the country for the individuals diagnosed with any kind of mental health problem.
In 1935, legislation period had started preparing. After a decade, in 1945, the Social Security Institution was constituted in order to provide health needs of working class, being included in the social security system
(Dilik, 1971). Then, with the period of socialization and decentralization of health care in 1960s, preventive mental health implementations had been increased, especially in rural areas. This service had also been free of charge for the large populations in those areas (Gökalp & Aküzüm, 2007).
There had been also reforms in the mental health houses, and/or asylums in years. In the beginning of the twentieth century, asylums were reformed firstly, where were the favorite place in order mental illness to be cured. Then the first mental health hospital was founded in Elazig in the east part, and in Manisa in the west part of Turkey (Gökalp & Aküzüm, 2007). In psychiatry and neurology the first teaching hospital was founded in Bakirkoy, Istanbul in 1927.
During 1940s, individuals diagnosed with a mental illness had stayed in the hospital and were employed in the hospital in cooking, laundry, agricultural works, gardening and some other different jobs with a few salaries. Yet, because of the financial problems and limited resources, the system could not have continued (Gökalp & Aküzüm, 2007). By the support of psychiatry departments in Ankara and Kocaeli universities, new mental health hospitals were founded. New rehabilitation centers have also been constituted for a few years, within which both inpatients and outpatients have been given treatment. The families of the patients have also been given psychological support (Gökalp & Aküzüm, 2007).
1.3.2. Demographic Information of Mental Health Workers
Mental health workers have mostly meant psychiatrists in the past years, especially because of the mental health hospitals. Yet, in the last decades, mental health services in all countries, including Turkey have been expanded in range. In Turkey, mental health professionals have been
working in different jobs in the mental health sector, including psychiatrists, clinical psychologists, psychologist with any other specialization field of psychology, neuro-psychiatrists, psychological counselors, social workers and/or psychotherapists.
With a start of definition of “psychotherapist”, Hill, Nutt, & Jackson (1994, p. 365) defined it as “one who has been specifically trained as a professional therapist (e.g. counseling or clinical psychologists,
psychiatrists, counselors, or social workers) or one who has been in training (e.g. prepracticum student, practicum student, and intern)”. Thus,
psychotherapist might be the adjective which defines the implementation of any kind of mental health worker. All the mental health workers have a possibility to be a psychotherapist, until they reach the requirements for that profession.
Psychotherapists may come from various areas of mental health sector. Guinee (2000) mentioned a brief report of the therapist sample. In his research, he had searched for the articles that were published in the Journal of Counseling Psychology between the years of 1988-1997. He questioned the characteristics of the therapists, and how consistently they reflected their traits on the researches. He mentioned about the
characteristics such as number of the sample, age, gender, race/ethnicity, professional status, setting, academic training, level of experience, theoretical orientation.
According to the results of Guinee’s study (2000), the number of the therapist sample is ranged from 1 to 320, with a mean of 30.4 (SD=49.23). Age range is from 22.5 to 51.5 with a mean of 36.2 (SD=7.5). 59% of the participants are female, 42% are male. The race/ethnicity of European Americans constitutes 86% of the samples. In terms of professional status, 52% of them are graduate students, 48% of them are professional therapists. In the present study, it is aimed to describe these variables mentioned above in Guinee’s study (2000), in the Turkish population among people who are dealing with the mental and psychological health sector. The gender distribution, age interval, professional statuses are intended to be described as the demographic information of the sample. In addition, working settings of the mental health workers are planned to be defined, mostly where the mental health professionals do work in Turkey. These work settings may be in a range, including private or state hospitals, private clinics, private or state schools, private or state universities, and etc.
1.3.3. Occupational Features of Mental Health Workers
1.3.3.1. Work Settings
In addition, work setting plays an important role for the
implementation of the treatment program. In the study (Guinee, 2000) it is found out that 25% of the therapist sample work in the university counseling
centers, 9% of them work in both counseling center and hospital clinic, 8% of them work in academic departments, and 4% of them work in the mental health centers. 23% of the samples have the clinical psychology or
counseling psychology training.
1.3.3.2. Experience years
There are various occupational features of mental health field, especially in terms of the professional characteristics. One of them which may play an important role for the treatment programs is experience year. It might be believed that the more experienced of a mental health worker, the better results may be taken from treatment. Yet in Guinee’s study (2000) experience years are argued whether the number of the experience year is valid for better solutions of treatment, or the number of the experience year with supervision is more valid. In his study (Guinee, 2000) the level of the experience of the therapist classified in three groups, novice (less than 2 semesters supervised practicum), experienced (2 or more completed semesters supervised practicum), experienced (postdoctoral psychologist).
1.3.3.3. Theoretical orientation
In addition to experience years, theoretical orientation of a mental health professional is the other important factor that may lead to various effects. Orientation of a mental health worker may influence the
psychological process of a patient in terms of time, money, point of view, and etc. Since there are a variety of orientations, the chosen and
implemented ones may be effective for both the professional’s opportunities and personal characteristics and the patient’s daily life.
In order to determine the theoretical orientation of the professionals, in Guinee’ study (1994), participants are asked to list the most useful orientation they feel for themselves. In addition, Vasco and Dryden (1994) mentioned that while the therapists are selecting their theoretical orientation, they attend to different kinds of issues. The theoretical orientations are classified as humanistic and psychodynamic, systemic, cognitive, behavior, and eclectic. Thus, the points, that the therapists value, are different from each other.
A therapist who chooses to work with a humanistic or
psychodynamic approach, he emphasized that orientation of his own therapist influenced his selection of his own orientation as a therapist. A systemic therapist is influenced by family experiences and type of patients they work with. These two groups of people are not influenced by the research results.
On the other hand, cognitive psychotherapists are seemed to be influenced by the research results, but not the orientation of own therapist. Behaviorstic psychotherapists are influenced by the research results, but without the effect of personal philosophy and values, and ability to help one understand oneself. Finally, therapists who choose eclectic approach, are also influenced by research results, and thinking of the ability to help one understand oneself, but without emphasizing the personal philosophy and values, and accidental circumstances (Vasco & Dryden, 1994).
The preference of the theoretical orientation is also found related with the values of the psychotherapists (Rubinstein, 1994). It is mentioned that the therapists’ values are significant for choosing the theoretical orientation, and in addition the attitudes toward the patients are associated with the values of the therapists. In another study (Norcross & Wogan, 1987), it is emphasized that 89% of the sample agree on personal values of psychotherapists have direct influence on the psychotherapy outcome. In addition, 43% of the sample agrees that therapy should be influenced by the therapists’ values, and 37% of the sample disagree on this. Moreover, therapists prefer behaviorist and humanistic approaches seem to agree more on the influence of the values, rather than the professionals of
psychoanalytic approach.
In some other studies (Garfield & Kurtz, 1976; Vasco & Dryden, 1994) many other issues have been suggested in choosing the proper theoretical orientation for the professional.
In one of these studies (Garfield & Kurtz, 1976), it is found that most of the (55%) clinical psychologists prefer to work with eclectic approach in their practical field of profession. The second preferred theoretical
orientation among the sample is psychoanalytic approach (11%).
In the other research (Vasco & Dryden, 1994), it is also discussed about the changes in the initial theoretical orientation. It is believed that the clinical experience of the therapist is the most fundamental factor that influences the changing the first orientation of the therapists. Yet, of course this change may not be occurred, unless the therapists are flexible enough.
In the present research, one of the important points is to see the prevalence of these theories in terms of being used by the psychotherapists, clinicians, psychiatrists, social workers, school counselors and etc in Turkey. Moreover, whether the theory they use are related with their previous experiences in their self-psychotherapy period. Hence, this study also tries to investigate whether the people working in psychological health field take psychotherapy for themselves, before or during their profession, or not.
1.3.3.4. The professional and academic profiles of mental health
workers
In the study (Garfield & Kurtz, 1976), the professional and academic profiles of the clinical psychologists in the United States in the 1970s have been identified. The majority of sample of the study have a doctoral degree, with the percentage of 95. The level experience of the clinicians is different. It is less than one third of the sample, that their experience is less than 10 years. Besides, less than one third of the sample has the experience level of 20 or more years. The majority of the sample (%59) indicates that they view themselves as clinical practitioners, and secondly they view themselves as academicians with 20% (Garfield & Kurtz, 1976).
In another study (Affleck & Garfield, 1960), it is mentioned that experience is related with the congruent views of the patients about the psychotherapy process. This stands for the fact that the more the therapist is experienced, the more congruent idea he/she has about what the patient is
thinking about his/her own psychotherapy period. On the other hand, social workers of the study (Affleck & Garfield, 1960), show high reliability in the ratings of intelligence. Yet it is also mentioned that they show less
agreement than experienced clinical psychologists about the psychotherapeutic outcomes or aspects.
1.3.3.5. Personal psychotherapy for the Mental Health Workers
Years of experience, working as a clinical psychologist, or
psychiatrist, or social worker or school counselor, having personal therapy for the psychotherapists are also found indicative for the outcomes of the psychotherapy process of a patient. Thus, for a clinician working with different kinds of patients having personal therapy is very indicative
(Garfield & Kurtz, 1976) in terms of being effective as a professional in that period. In this study, the sample contains 855 professionals, and 63% of the sample size has been taken their personal therapies. It is mentioned most of the professionals being undergone psychotherapeutic support are female. Moreover, one of the questions asked in the questionnaire of the study is whether every clinical psychologist must experience personal therapy process, or not. The answers are mostly “yes” (45%) and “no” answers are not so few (38%). 17% of the sample is undecided for this question.
Another question being asked in the study (Garfield & Kurtz, 1976) is in what degree personal therapy for the psychotherapists is prerequisite in terms of being effective in the clinical performance of therapists. 36% of the sample mentioned that personal therapy is very important. 26% of the
sample agreed that personal therapy is moderately important. 22% of the sample is undecided about the importance of personal therapy. 15.5% of the sample mentions that it is unimportant.
In the present study, one of the aims is to find out whether professions dealing with psychological health issues spend much
importance to take personal therapy, during or before they start performing in the field. Moreover, this study tries to mention whether there is an association between the theoretical orientation of personal therapy and the contents of the theoretical education of the psychotherapists, with
explaining what kinds of educational programs psychotherapists undergo.
1.3.3.6. Political and Religious Views of the Mental Health Workers
Political views and religion are also important in terms of identifying professionals of psychological health field (Rubinstein, 1994). In this study, political views and the religious beliefs of the therapists in Israel are
investigated. The sample size of the study is 624, and most of the
practitioner participants (46.7%) define themselves from the left wing. This does not stand for Socialist view, yet traditional distinction between right and left wings in terms of socioeconomic system. Moreover, majority of the practitioner sample (76.5%) of the study (Rubinstein, 1994) defined
themselves as secular in the scale of secular, traditional, orthodox, and ultraorthodox. 13.1% of the other practitioner sample defined themselves as traditional, 9.7% as orthodox, and lower than 1 % as ultraorthodox.
1.4. Research Questions and Explorations 1.4.1. Research Questions
The current study presented the variables that identified the mental health workers in Turkey in four different aspects. The first of them was socio-demographic characteristics. Secondly, educational backgrounds of the mental health workers were described. Thirdly, the professional details of the professionals in the mental health field were investigated. And lastly, political and religious related social identities of the mental health
professionals in Turkey were described. In terms of these different four aspects, how the mental health workers were distributed in the field was the topic mentioned in the study.
1.4.2. Explorations
For the explorative analyses of the study, possible predictors of following dependent variables were explored: 1) Mental health workers’ perceived level of healing in their clients. 2) The percentage of clients who completed the clinical service that was suggested by the professionals in appropriate time. 3) The drop out reason that difficulties were experienced in the clinical relationship, mostly due to the clinician. 4) The drop out reason that difficulties that were experienced in terms of theoretical
orientation. That is, the theoretical orientation that the professional endorsed did not match with the client’s needs or problems. 5) The primary
the people who experienced psychological difficulties in Turkey. 6) Psychotherapy as the proposed type of primary clinical intervention by the mental health workers for the people who experienced psychological difficulties in Turkey. 7) Total degrees of difficulty that the mental health workers experienced with different cases.
CHAPTER II. METHOD
2.1. Participants
The sample of the study was the professionals who work in the mental health service actively. The professionals who did not work with the clients actively excluded from the sample. The participants, the details of which could be seen in Table 1 named as socio-demographic characteristics, were described in terms of gender, age, marital status, birth place and city of residence.
Distribution of the socio-demographic characteristics was presented in Table 1 according to frequency and percentage distributions. As can be seen from the table, the sample consisted of 245 individuals. There were 195 females (79.6%), and 50 males (20.4%) in the sample.
Age of the participants had a mean of 32 (n= 244; SD= 8.1). The most prevalent age group was found to be 26 to 30 with 34.8%, followed by the age group of 22 to 25 with 21.7%.
In terms of marital status, the participants of the study were divided into two groups. The first group was the singles (58.4%), and the second
Characteristics N % Gender Female 195 79.6 Male 50 20.4 Age groups 22-25 53 21.7 26-30 85 34.8 31-35 46 18.9 36-40 25 10.2 40+ 35 14.3 Marital Status Single 143 58.4 Married/ Living Together 102 41.6 Birth Place Village/ District 18 7.3 Town 31 12.7 City 64 26.1 Metropolis 132 53.9 City of Residence İstanbul 177 72.2 Ankara 22 9.0 İzmir 12 4.9 Bursa 6 2.4 Others 28 11.4
Note: n= 244 for Age groups and n= 245 for the others.
group was formed by the people who were married or living together with a partner (41.6%).
With regard to the birth places of the participants, the majority (53.9%) was born in metropolitan cities, followed by cities (26.1%), towns ((12.7%), and villages or districts (7.3%).
The current cities of residence of the participants were also described in Table 1. Since there are eighty one cities in Turkey, the most common ones were presented, and the other ones with the lower frequencies were named as others. The highest percentage of the sample resided in İstanbul
(72.2%), followed by Ankara (9%), İzmir (4.9%), and Bursa (2.4%). 11.4% of the sample resided in the other cities of Turkey.
Table 2 contained the self reports of university degrees, and/or master, and/or doctorate, and/or post-doc degrees, self- description of occupation, and work setting.
The sample has a variety of occupation in the mental health field. The distribution of the occupations was presented in Table 2. The
participants named their occupations by self report. They might define their occupations not only in one profession, but also more than one. The most percentage of the sample was formed by the individuals who work as a “psychologist”, with the highest percentage of 42.4.
The second popular occupation in the sample was “clinical psychologist” group (18.8%). With the percentage of 20, the other group was the “psychotherapist” group. The fourth occupation group was
“psychological counselors” (10.2%). The following self reported occupation
group was “adult psychiatrist” (7.4%).
The other occupation group identified by the participants was the “psychological counselor MA” group (7.3%). The following group was
constituted by the “adult psychiatrist intern” group (5.3%). The other one was the “psychoanalyst candidate” group (3.2%). The following group of occupation was “child and adolescent psychiatrist” group (1.2%).
Table 2. Characteristics of occupation, educational level, and work setting (n= 245) n % Occupation Psychologist 103 42.4 Clinical psychologist 48 18.8 Psychotherapist 48 20.0 Psychological counselor 25 10.2 Adult psychiatrist 19 7.4 Psychological Counselor, MA 18 7.3
Adult psychiatrist intern 14 5.3
Psychoanalyst candidate 8 3.2
Child & Adolescent psychiatrist 7 1.2
Psychoanalyst 5 2.0 Psychiatry nurse 5 2.4 Others 33 12.9 Education level Undergraduate degree 148 60.4 Master degree 73 29.8 Doctorate degree 22 9.0 Work setting
Private psychological counseling
center 41 16.7
Private psychotherapy center 35 14.2
State hospital 23 9.4
State psychiatry hospital 23 9.4
Rehabilitation center 18 7.4
Private university 18 7.4
Private office 17 6.9
State mental health hospital 16 6.5
Private hospital 15 6.1
NGO 15 6.1
Others 101 40.8
The following two groups were identified by “psychoanalyst” (2%) and “psychiatry nurse” (2.4%). The last group of occupation was defined as “others” which stood for the other types of occupations defined by the
participants except the ones defined above (12.9%).
The individuals in the sample are reported their university degrees, in terms of undergraduate, graduate, doctorate levels. In table 2, the distribution of the university degrees was also presented. There were only two people who did not mention their degrees. Thus, there are only two missings in the sample. The highest percentage of the degrees was held by the participants (60.4%), who had only undergraduate level in their own field. The second group was formed by the individuals, who held only master’s degree (29.8%), after their undergraduate level. In the last group, there were the participants who reported that they had doctorate level (9%), after their undergraduate and master’s degrees.
The participants were also reported their work settings. The
distribution of the settings was presented in table 2. The most common work setting of the sample was private psychological counseling center (16.7%). The following working setting of the sample was private psychotherapy centers (14.2%). The third common work place of the individuals in the study was state hospitals (9.4%). With the same percentage, the other work setting being reported by the sample was state psychiatry hospitals. The following two places at which the professionals work were the rehabilitation center and private universities (7.4% each). The next common working setting mentioned by the sample was the private offices of the mental health
workers (6.9%). The other place was the state mental health hospitals (6.5%). The next two working setting were private hospitals and
non-governmental organizations (6.1% each). And the last group of work setting was named as “others” (40.8%) which included the other mental health working settings reported by the participants. It included the ones who did not work in the settings mentioned above, but in different ones. 40.8% of the sample was formed by this group.
2.2. Instruments 2.2.1. Questionnaire for the mental health workers
This study was a part of a larger study. The questionnaire of the larger study was developed by the research team (Murat Paker, Sevilay Sitrava-Günenç, and Ezgi Soncu) and was consisted of five modules. The modules were: 1) socio-demographic information, 2) educational
background, 3) professional information, 4) self-definitions in terms of political and religious views, 5) clinical scales. The current study was based on only the first four modules of this larger study. These four modules of the questionnaire can be seen in Appendix 1.
In the first module, as demographic variables age, gender, marital status, hometown, and current town of the participants were asked.
The second module was named as education. In this module, the educational degrees were mentioned, whether the professionals had a
bachelor’s, master’s, doctoral and post-doctoral degrees, or not. If there was, it was expected to see from which field of study specifically the participants
had a bachelor’s degree, and masters, and doctoral degree. These were asked in a “Yes/No” question format, if the answer was “Yes” then the
participants were expected to write down whether it was abroad, or not, with the graduation year.
In the third module, professional profiles of the participants were expected to figure out. In this part, how the participants named themselves as a person performing clinical practice actively in the field was mentioned. In which settings, the professionals were working in terms of clinics, whether the participants were also working as an academician or not, whether the professionals provided clinical supervision to colleagues or not, the experience years of the participants were all asked in this module. This information was considered to report by the participants, by choosing multiple choices which best fit for themselves.
In addition, theoretical orientation of the clinical professionals, their theoretical education, and personal therapy for the clinicians and personal clinical supervision for the professionals were the important parts of the module.
Moreover, foreign languages the participants were capable of reading, and/or writing, and/or speaking, and/or being able to use them during the clinical practice was also asked in this module. The profiles of the patients/counselees applying for any kind of psychological help were intended to figure out. The progresses of these patients/counselees during any kind of psychological support, what the first and the second
considered to define. Among these patients/counselees, with what kind of problems the professionals might be coerced was the other part of the module.
In the last module, the political, religious, and ethnic profiles of the participants were asked. The listed adjectives were asked in a likert scale format. The participants were expected to give answers in the five point scale, in which “0” stood for “never define oneself”, and “4” stood for “completely define oneself”.
2.3. Procedure
The data of the current study was first collected through a web-based survey program called Webropol. The questionnaire of the study designed by the research team was set on the web site; and the link of the
questionnaire was sent to the email groups of the professionals, in which psychologists, psychiatrists, psychological counselors, social workers, and other mental health workers were the members. With emails, e-invitations of the study were sent to people in the field. The ones, who accepted the e-invitation, could participate in the study. It was possible for the participants to go back to the questionnaire whenever they preferred to continue. It took approximately 30-40 minutes to fill in the questionnaire.
Via web link, between August 2009 and December 2009, there were 204 people being reached through Internet. Yet, it was thought limited for the purposes of the study, and then another process was added into the procedure. Then, in January 2010, hard copy of the questionnaire was
prepared and distributed to the mental health work settings by the research team. Those places were the ones which were the prominent psychiatry departments, mental health hospitals, psychotherapy centers, psychological counseling centers located in Istanbul. 264 questionnaires were sent to the mental health centers. 41 of them had returned. The return rate of the questionnaires was 15.5%. This sampling lasted three more months, beginning in January 2010 and lasting in April 2010.
In the sample, there were totally 245 participants. 204 (83.3%) were participated via e-invitations and 41 (16.7%) through hard copy invitations.
2.4. Data Analysis
In this study, identifying information of mental health workers working in the field of psychological health in different cities of Turkey was considered to figure out. The socio-demographic information, educational and professional characteristics were intended to describe. These variables were computed with the frequencies and percentage levels among the Turkish population of professionals working in mental health sector.
These professionals were divided into six different groups, according to the professions. The first group was the psychologists with BA degree and/or with a MA degree rather than clinical psychology (n=92). The second was formed by the psychiatrists, both the interns and the residents (n=31). The third group was defined by the psychological counselors who have a bachelor’s degree in the field of guidance and psychological counseling (n=29). In the fourth group, clinical psychologists who have a
master’s degree in the field of clinical psychology were included (n=51). The fifth group was formed by the clinical psychology MA students (n=29), and the last group was named as “others” who did not match the previous groups, but others, such as social workers, psychiatry nurses and etc (n=13).
The relationships of the categorical variables among the six groups above were computed by Chi-Square. In addition, the relationships of the continuous variables among the six groups were computed by One-Way Analysis of Variance (ANOVA). The relationships among the groups were analyzed by Post hoc Scheffe results. Moreover, multiple regression analyses were performed for the explorative statements of the study.
CHAPTER III. RESULTS
3.1. Descriptive Analyses of the Study
In order to describe the characteristics of the mental health
professionals, the results were classified into five groups, according to their contents. These are; socio-demographic information, education and training, experience related factors, client-related factors, and proposed interventions.
3.1.1. Socio-demographic Characteristics of the Sample
There were a total of 245 participants who completed the
questionnaire of the study and included in the analyses. The mean age of the overall sample was 32. The sample of the study was mostly between the ages of 26 and 30, this age interval constituted 34.8% of the sample. Minimum age of the sample was 21, maximum was 61. The psychologists (M= 29.5) and the clinical psychology MA students (M= 27.3) were significantly younger than the other four groups.
Table 3 shows the socio-demographic characteristics of the whole sample and each professional group. The results showed that the mental health professionals were mostly female (79.6%). One fifth of the sample
was male. Psychiatrists were the only group in the sample with a majority of males (61.3%). More than half of the sample was single (58.4%). Almost half of the sample (44.5%) got divorced once. The highest percentages of getting divorced once belonged to psychologists and clinical psychology MA students, unexpectedly.
In terms of birth place, psychologists, psychological counselors, clinical psychologists and clinical psychology MA students were mostly born in metropolises. Yet, psychiatrists were mostly born in cities, and other professional group was mostly born in towns. Currently, majority of the professionals (72.2%) resides in Istanbul as a metropolis.
Table 3. Socio-demographic Characteristics Groups Socio-demographic Characteristics Total (n=245) 1 Psychologists (n=92) 2 Psychiatrists (n=31) 3 Psych. Counselors (n=29) 4 Clinical Psych. (n=51) 5 Cli.Psy. MA St. (n=29) 6 Others (n=13) p (NS, if p>.05) Mean Age (SD) 32.0 (8.1) 29.5 (6.9) 37.0 (8.6) 34.2 (7.3) 33.6 (8.5) 27.3 (5.1) 37.8 (9.3) .000 1=5<2=3=4=6 Age Groups % .000 22-25 21.7 37.0 --- 6.9 --- 55.2 8.3 26-30 34.8 31.5 35.5 27.6 52.9 27.6 16.7 31-35 18.9 16.3 16.1 37.9 19.6 10.3 16.7 36-40 10.2 7.6 12.9 13.8 9.8 3.4 33.3 40+ 14.3 7.6 35.5 13.8 17.6 3.4 25.0 Gender % .000 Female 79.6 85.9 38.7 79.3 88.2 82.8 92.3 Male 20.4 14.1 61.3 20.7 11.8 17.2 7.7 Marital Status % .027
Married & Living Together 41.6 34.8 54.8 55.2 49.0 20.7 53.8
Single 58.4 65.2 45.2 44.8 51.0 79.3 46.2 Number of Children % NS 0 42.4 40.2 38.7 34.5 54.9 44.8 30.8 1 44.1 47.8 35.5 55.2 33.3 51.8 38.5 2 10.2 8.7 19.4 10.3 7.8 3.4 23.1 3 3.3 3.3 6.5 --- 3.9 --- 7.7 Number of Divorce % NS 0 52.7 45.7 54.8 65.5 53.8 48.3 61.5 1 44.5 54.3 35.5 31.0 42.5 51.7 38.5 2 2.9 --- 9.7 3.4 3.8 --- ---
Table 3. Socio-demographic Characteristics (cont’d) Groups Socio-demographic Characteristics Total (n=245) 1 Psychologists (n=92) 2 Psychiatrists (n=31) 3 Psych. Counselors (n=29) 4 Clinical Psych (n=51) 5 Cli.Psy. MA St. (n=29) 6 Others (n=13) p (NS, if p>.05) Birth Place % .000 Metropolis 53.9 55.4 32.3 55.2 68.6 65.5 7.7 City 26.1 22.8 48.4 20.7 21.6 27.6 23.1 Town 12.7 14.1 9.7 17.2 5.9 6.9 38.5 Village or District 7.3 7.6 9.7 6.9 3.9 --- 30.8 City of Residence % .009 Istanbul 72.2 59.8 80.6 82.8 74.5 89.7 69.2 Ankara 9.0 10.9 16.1 6.9 5.9 3.4 7.7 Izmir 4.9 4.3 --- 3.4 9.8 --- 15.4 Bursa 2.4 2.2 --- --- 5.9 3.4 --- Other 11.4 22.8 3.2 6.8 3.9 3.4 7.7
Groups: 1: Those who have a B.A. or M.A. degree other than clinical psychology in psychology
2: Psychiatry interns and residents
3: Those who have a B.A. degree in guidance and psychological counseling 4: Those who have clinical psychology M.A. degree
5: Clinical psychology M.A. students
Participants rated some characteristics in terms of the degree to which they define their social identity as presented in Table 4 (for detailed table see Appendix 2). The participants rated the social identities in a likert scale from 0: no identification to 4: totally identified. These characteristics were classified into five different groups, according to the concept that they are based on as geography-based, national/ethnic, religious, political and sexual identities.
In terms of geography based identities, mental health professionals believed that mostly being an Earth citizen (3.1) and being from Turkey (2.7) identified them; whereas geographical-region based definitions identified them least (e.g. Tharcian: 0.4).
Comparing the six groups regarding geography-based identities, there were significant differences. It was found that: 1) Being Anatolian identified psychiatrists (1.6) more significantly than and clinical psychology MA students (0.4).
2) Psychiatrists (1.4) were the most identified group significantly with being Middle Eastern; whereas clinical psychology MA students (0.6), psychological counselors (0.5), and others (0.3) identified themselves significantly least.
In terms of national/ethnic identities, the mental health professionals mostly believed that being Turkish (2.2) identified them mostly, in spite of at somewhat level. They believed that the other national/ethnic identities did not identify them.
Regarding religious identities, the mental health professionals believed that being Muslim (1.5) and Sunni (1.0) defined them, despite to a low degree. Clinical psychologists believed that religious identities defined them the least, whereas the other professionals defined themselves the most with religion.
Comparing the six groups, there were significant differences
regarding religious identities. It was found that: 1) Other professionals (2.5) identified themselves with being Muslim mostly (2.5); whereas psychiatrists (1.2) and clinical psychologists (1.0) defined themselves as Muslim the least.
2) Regarding being Sunni, others (1.8) defined themselves mostly, clinical psychology MA students (0.7), and clinical psychologists (0.5) were identified with being Sunni the least.
3) Other professionals defined themselves being Shiite the most, whereas psychiatrists (0.03) identified themselves with being Shiite the least.
The mental health professionals believed to be left-winger (1.4) mostly in terms of political identities. Among the groups, there were no significant results. In addition, regarding sexual identities, participants mostly defined them as heterosexual (2.5).
![Table 4. Social Identities of Mental Health Professionals Groups Social identities- Mean (SD) [0= no identification… 4= high identification] Total (n=244) 1 Psychologists (n= 92) 2 Psychiatrists (n=31) 3 Psych](https://thumb-eu.123doks.com/thumbv2/9libnet/4251790.67563/58.1262.89.1182.242.759/identities-mental-professionals-identities-identification-identification-psychologists-psychiatrists.webp)