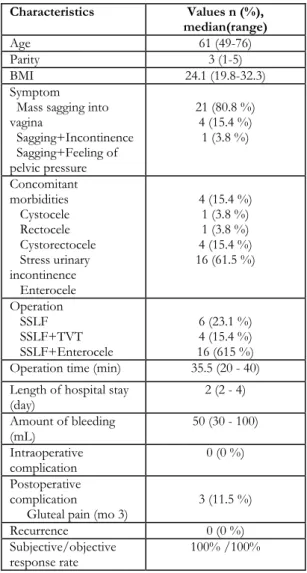
Outcome of sacrospinous ligament fixation with conventional instruments in the treatment of Stage 3-4 vaginal vault prolapse
Tam metin
Şekil
Benzer Belgeler
In order to improve the survival of elderly esophageal cancer patients, they scrutinized two points: postoperative critical care in order to prevent pulmonary complications
[11] reported that ten women in the ICU with severe COVID-19 were tested for SARS-CoV-2 in vaginal fluid by RT-PCR assay, and all samples were negative for the virus.. Their
The effect of adjuvant treatment modalities on survival outcomes in cytoreductive surgery performed patients with advanced stage uterine sarcomas Sitoredüktif cerrahi
In the second month, statistically significant improvements con- tinued in walking VAS scores (p=0.007), flexion of the knee VAS scores (p=0.001), WOMAC pain scores (p=0.001), WOMAC
The results of our study showed that short term maternal and neonatal complications of vacuum-assisted vaginal delivery and cesarean section during the second phase of labor
A high local control rate with no major toxicity was obtained by stereotactic ablative body radiotherapy in the patients with medically inoperable early-stage non-small cell
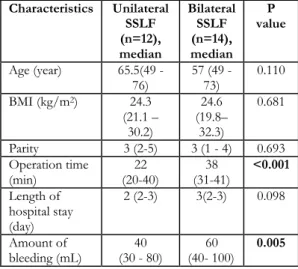
Both length of operation and hospital stay were significantly longer in the patients who underwent vaginal hysterectomy with sacrospinous ligament fixation (p<0.001);
Vaginal cuff dehiscence with bowel evisceration is a rare complication after hysterectomy, however, as laparoscopic and especially robotic surgery becomes widely performed around
