c
American Journal of Emergency Medicine 36 (2018) 1346–1349 Contents lists available at ScienceDirect
American Journal of Emergency Medicine
j o u r n a l h o m e p a g e : w w w . e l s e v i e r . c o m / l o c a t e / a j e m
Original Contribution
Evaluation of activated charcoal and lipid emulsion treatment in model of
acute rivaroxaban toxicity
Sinan Cem Uzunget, MD
a,⁎
, Togay Evrin, MD
a, Sezen Baglan Uzunget, MD
b, Zamir Kemal Ertürk, MD
a,
Egemen Ak
ıncıoğlu, MD
c, Saffet Özdemir, MD
a, Atila Korkmaz, MD
aa
Department of Emergency Medicine, Ufuk University Faculty of Medicine, Ankara, Turkey
b
Department of Cardiology, Ufuk University Faculty of Medicine, Ankara, Turkey Department of Pathology, Ufuk University Faculty of Medicine, Ankara, Turkey
a r t i c l e i n f o
Article history: Received 19 June 2017
Received in revised form 13 December 2017 Accepted 13 December 2017
a b s t r a c t
Aim: Reducing or reversing the toxicity effects of new oral anticoagulants is an important question.The purpose of the present study is to evaluate the effect of lipid emulsion (LE) and Activated Charcoal (AC) therapy on the in toxication of rivaroxaban, on mice.
Methods: Adult male Balb/c mice weighing approximately 30 g were used in the study. Seven groups were assigned, with six mice in each group. Groups were defined; given only rivaroxaban, given only LE, given only AC, after the administration of rivaroxaban LE applied group in the 1st hour, after the administration of rivaroxaban LE applied group in the 3rd hour, after the administration of rivaroxaban AC applied group in the1st hour, after the administration of rivaroxaban AC applied group in the 1st hour and LE applied group in the 3rd hour. PT and Anti-Factor Xa activity were measured in all blood samples from subjects.
Results: A statistically significant difference was found when all groups were compared in terms of mean PT values and Anti-FactorXa values. However, no statistically significant difference was found in the mean PT and Anti-FactorXa values when only rivaroxaban administrated group and after the administration of rivaroxaban LE and/or AC applied groups were compared one to one. No deaths occurred in groups during the observation. Conclusion: Although the administration of either AC or LE alone or in combination resulted in a decrease in the mean values of PT and anti-Factor Xa, in case of rivaroxaban toxicity, but one-to-one comparison of the groups was not statistically significant.
© 2017 Elsevier Inc. All rights reserved.
1. Introduction
Acute intoxications are a major public health problem across the world. There are numerous applications to hospitals due to suicide, ac cidental exposure, and overdose of drugs or other chemicals. Although many life-saving attempts have been made in poisonings, basic treat ment has been limited to evacuation of the stomach, supportive care and activated carbon treatment even, indications for these treatments have been significantly de-emphasized and are now uncommonly used or indicated [1].
Activated charcoal (AC) is an effective adsorbent for many drugs and toxic substances [2]. But in recent years, its use has decreased substan tially [3].
⁎ Corresponding author at: Department of Emergency Medicine, Ufuk University Faculty of Medicine, Mevlana Bulvarı No:86-88, 06520 Balgat, Ankara, Turkey.
E-mail addresses: [email protected] (S.C. Uzunget),
[email protected] (A. Korkmaz).
https://doi.org/10.1016/j.ajem.2017.12.039
0735-6757/© 2017 Elsevier Inc. All rights reserved.
Lipid emulsions (LE), produced solutions used for total parenteral nutrition as a source of calories in the malnutrition, have been used in recent years as an effective antidote in lipophilic drug intoxica tions, primarily local anesthetic toxicity [4], and in the resuscitation of the hemodynamically unstable patients. Currently, it is suggested that lipid emulsions should be given to patients in drug poisonings that cannot be treated with the standard resuscitation approaches (5).
New oral anticoagulants are increasingly replacing vitamin K antag onists because they have advantages such as short half-lives, less drug interaction, no need for monitoring, and better pharmacokinetic profile
[6,7]. Rivaroxaban, one of these drugs, is lipophilic and also is an oxazolidinone derivative that selectively binds to factor Xa and acts as an inhibitor [8]. In case of rivaroxaban toxicity or side effects, preventing the absorption of rivaroxaban and increasing its elimination can reduce the toxic effects and mortality of this agent.
In this study, the effects of activated charcoal and lipid emulsion treatment in the treatment of acute rivaroxaban toxicity were evaluated.
1347 S.C. Uzunget et al. / American Journal of Emergency Medicine 36 (2018) 1346–1349
2. Materials and methods
This experimental study was carried out in Gazi University Laborato ry Animal Breeding and Experimental Research Center in November 2016. The study was approved by Gazi University Experimental Animal Ethics Committee. A total of 42 adult male Balb/c mice weighing 30 g were used in the study. Experimental animals were maintained in a 12 h light/12 h dark cycle at room temperature (24 ± 2 °C). They were allowed to reach the standard mouse diet and the water without restriction. 6 mice were placed in one cage.
2.1. Experimental groups
The mice were randomly divided into 7 groups (n = 6):
Group 1: Rivaroxaban (Vega Pharma Limited, Zhejiang, China) was orally administered at 300 mg/kg.
Group 2: 20% LE (Intralipid™ 20% Fresenius Kabi AB, Uppsala, Sweden) was administered intraperitoneally at 15 ml/kg.
Group 3: AC (Aqua-Carbo® 50 g/240 ml, Avicenna Farma, Istanbul, Turkey) was orally administered at 1 g/kg.
Group 4: Rivaroxaban was orally administered at 300 mg/kg, and then 20% LE was administered intraperitoneally at 1st hour.
Group 5: Rivaroxaban was orally administered at 300 mg/kg, and then 20% LE was administered intraperitoneally at 3rd hour.
Group 6: Rivaroxaban was orally administered at 300 mg/kg, and then AC was orally administered at 1 g/kg at 1st hour.
Group 7: Rivaroxaban was orally administered at 300 mg/kg, and then AC was orally administered at 1 g/kg at 1st hour and 20% LE was administered intraperitoneally at 3rd hour.
While rivaroxaban and AC were given with orogastric tube, LE was administered intraperitoneally. 300 mg/kg rivaroxaban was adminis tered according to previously defined LD 50 dose in mice [9]. One study conducted by Perez et al. demonstrated that survival rose after 18,6 ml/kg LE in rodents [10] but because of poor solubility and lower blood volume in mice, we applied 15 ml/kg LE and 300 mg/kg rivoraxaban each mouse.
No deaths were observed in the groups during the experiment. All experimental animals were anesthetized with 50 mg/kg IM ketamine (Ketamine hydrochloride, Ketalar®, Pfizer, Istanbul, Turkey) 5 h after first drug administration. They were sacrificed by the cardiac puncture blood collection method.
The brain(cerebrum and cerebellum), stomach, small and large bowel tissues were appropriately obtained from the sacrificed subjects for pathological examination. The samples was examined by the same pathologist who was blinded to the groups of samples. Specimens were fixed in 10% of formalin solution. After obtaining slices of 4 to 5 mm of thickness from the paraffin embedded specimen, they were stained with hematoxylin and eosin. The samples were evaluated for hemorrhage under light microscope. The criteria for the minor hemor rhage in the gastrointestinal tract (stomach, small intestine and large bowel) was extravasation of blood into the mucosa, muscularis mucosa, submucosa, muscularis propria and serosa. Also the criteria for intrace rebral hemorrhage was extravasation of blood into the brain parenchyma.
The blood samples from mice were transferred to 3.2% (109 mmol/l) sodium citrate tubes at an appropriate dose. Prothrombin time (PT) and anti-factor Xa (Anti-FXa) activity were examined.
2.2. Statistical method
Statistical analyzes were performed with the SPSS for Windows Ver sion 20.0 package program. Numerical variables were expressed as mean ± standard deviation and median [minimum-maximum] values. The Kruskal-Wallis test was used whether there was a difference be tween the groups in terms of PT and Anti-FXa activity. P b 0.05 was
considered statistically significant. Power analyze was performed and 6 animals for each group were determined.
3. Results
PT and Anti-FXa values of the groups not receiving rivaroxaban (Groups 2 and 3) were compared with those of the rivaroxaban group and the rivaroxaban + treatment groups. The group receiving only AC was defined as the control group (Tables 1, 2).
Although there were some small decreases in mean PT and Anti-FXa levels as the control group and four rivaroxaban + treatment groups (groups 4,5,6,7) were compared, these results were statistically insignif icant. (Group 4 PT:32.07 ± 9.31 Anti-FXa: 1320.33 ± 275.61, Group 5 PT:31.25 ± 12.15 Anti-FXa 1708.67 ± 482,20, Group 6 PT 26.13 ± 7.60 Anti-FXa 1237.67 ± 344.95, Group 7 PT:22.33 ± 7.95 Anti FXa:760.33 ± 166.95). (Figs. 1,2).
Also, the statistical analyze showed that there were no discrimina tion in mean PT and Anti-FXa levels between given LE in the first hour and in the third hour.
3.1. Pathological examination
There was no macroscopic and microscopic hemorrhage in all sam ples of groups.
4. Discussion
The use of rivaroxaban at very high doses leads to deterioration in coagulation tests. It is known that particularly a massive rivaroxaban overdose prolongs the PT. The concentration of rivaroxaban cannot be assessed by routine coagulation tests, but it is known that an increase in rivaroxaban concentration prolongs the PT and aPTT [7,8,11,12]. In a study conducted on healthy volunteers by Eerenberg et al. [13], they found that the PT was prolonged. Although it was reported that the PT was prolonged when rivaroxaban was used at high doses, its use is not rec ommended in clinical evaluation. The chromogenic anti-factor Xa assay is recommended as a routine monitoring method for factor Xa inhibitors [7, 11,12,14].
In our study, it was found that the mean PT was prolonged and anti-factor Xa activity increased in mice receiving rivaroxaban. When the rivaroxaban group was compared with the groups not receiving rivaroxaban, the PT was increased and there was a statistically signifi cant difference (p b 0.001).
Activated charcoal used to prevent drug absorption from the gastro intestinal tract after drug overdose may also be useful for overdose of factor Xa inhibitors [11]. In a study performed on healthy volunteers by Wang et al. [15], AC was given following administration of apixaban
Table 1
All groups descriptive values.
PT (second) Anti-Fxa (ng/ml) (Mean ± SD) (Mean ± SD) Group 1 38,93 ± 9,13 1929,83 ± 344,18 (Rivaroxaban) Group 2 10,50 ± 0,33 b25 (LE) Group 3 10,07 ± 0,40 b25 (AC) Group 4 32,07 ± 9,31 1320,33 ± 275,61 (Rivaroxaban + LE 1st hour) Group 5 31,25 ± 12,15 1708,67 ± 482,20 (Rivaroxaban + LE 3rd hour) Group 6 26,13 ± 7,60 1237,67 ± 344,95 (Rivaroxaban + AC) Group 7 22,33 ± 7,95 760,33 ± 166,95 (Rivaroxaban + AC + LE)
PT: Prothrombin time, SD: Standard deviation, Anti-FXa: Antifactor Xa, LE: Lipid emulsion, AC: Activated charcoal.
1348 S.C. Uzunget et al. / American Journal of Emergency Medicine 36 (2018) 1346–1349
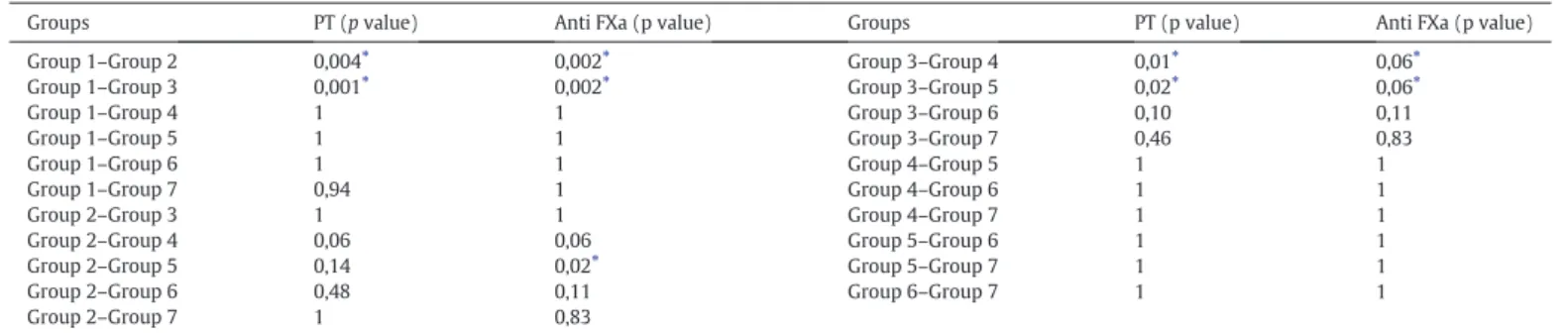
Table 2
P value comparison between groups
Groups PT (p value) Anti FXa (p value) Groups PT (p value) Anti FXa (p value)
Group 1–Group 2 Group 1–Group 3 Group 1–Group 4 Group 1–Group 5 Group 1–Group 6 Group 1–Group 7 Group 2–Group 3 Group 2–Group 4 Group 2–Group 5 Group 2–Group 6 Group 2–Group 7 0,004⁎ 0,001⁎ 1 1 1 0,94 1 0,06 0,14 0,48 1 0,002⁎ 0,002⁎ 1 1 1 1 1 0,06 0,02⁎ 0,11 0,83 Group 3–Group 4 Group 3–Group 5 Group 3–Group 6 Group 3–Group 7 Group 4–Group 5 Group 4–Group 6 Group 4–Group 7 Group 5–Group 6 Group 5–Group 7 Group 6–Group 7 0,01⁎ 0,02⁎ 0,10 0,46 1 1 1 1 1 1 0,06⁎ 0,06⁎ 0,11 0,83 1 1 1 1 1 1 Group 1: Rivaroxaban. Group 2: LE. Group 3: AC.
Group 4: Rivaroxaban + LE 1 st hour. Group 5: Rivaroxaban + LE 3 st hour. Group 6: Rivaroxaban + AC. Group 7: Rivaroxaban + AC + LE.
PT: Prothrombin Time, Anti-Fxa: Antifactor Xa, LE: Lipid Emulsion, AC: Activated Charcoal. ⁎ p b 0,05.
at toxic dose, and the concentration of apixaban was found to be de creased. Except for a case report who used rivaroxaban due to pulmo nary thromboembolism and received a high dose of rivaroxaban due to wrong order and then was treated with AC [16]. The idea that lipid emulsions are used as lipophilic drug during intoxication has existed for a long time. It was studied on gluthemid for lipid emulsions to be used as di alysate in lipophilic drug toxication [17]. In an animal experiment, intrave nous fat emulsion was used to reduce the effect of chlorpromazine [18]. A study conducted in 1998 found that lipid therapy is a useful treatment for local anesthetic systemic toxicity [19]. Scientists who have been studying in this regard have thought that intravenous lipid emulsion therapy may be beneficial in lipophilic drugs and have achieved various results. There are studies about its use in the toxicity of many lipophilic substances, primarily the toxicity of local anesthetics such as bupivacaine [20], lidocaine [21], and ropivacaine [22]. Currently, the use of lipid emulsion therapy in resuscitation attempts after local anes thetic toxicity and in situations where drug toxicity cannot be resolved with the standard resuscitation approaches is recommended in 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care [5].
In the literature, there is no study on the use of lipid emulsion and/or activated charcoal in rivaroxaban toxicity.
In our study, the control group and the rivaroxaban + treatment groups were compared in terms of PT and anti-factor Xa levels, it was seen that the mean PT and anti-factor Xa levels increased in the groups receiving rivaroxaban + LE at 1 h, rivaroxaban + LE at 3 h, rivaroxaban + activated charcoal at 1 h and rivaroxaban + activated charcoal at 1 h + LE at 3 h. However, there was no statistically significant difference be tween these groups (respectively, p = 1.00, p = 0.06; p = 1.00, p = 0.20; p = 1.00, p = 0.11 and p = 0.95, p = 0.83).
In our experimental study, the intraperitoneal route was preferred because LE should be given in the amount that we cannot give intrave nously to mice. LE was given intraperitoneally in some previous studies, and it is known that intraperitoneal absorption occurs from the first hour [23,24]. However, in our study, it is considered that LE did not completely pass into the systemic circulation because it was planned to see its effect within the first 6 h and that the optimal LE levels in the plasma could not be reached because no a further infusion of LE was given. However, the decrease in PT value is thought to be clinically important.
The general approach in acute drug intoxications is decontamination of the substance and supportive care [25,26]. Moreover, the use of the antidote can be a solution. Therefore, it is thought that new and more ef fective medical treatment methods for detoxification are needed [27].
1349 S.C. Uzunget et al. / American Journal of Emergency Medicine 36 (2018) 1346–1349
New treatments in toxicology are being investigated with original methods such as radioligand binding, use of nanobodies, protein-protein interaction inhibitors, aptamers, antisense oligonucleotides, and protein-selective small molecules [1,28-33]. However, considering the factors such as cost and accessibility, a general antidote application would be cheaper and accessible rather than a special antidote to each poison. There was a 61% decrease in the mean Anti-FXa levels in the group receiving AC at 1st hour and LE at 3rd hour after rivaroxaban compared to the rivaroxaban group that the use of AC and LE would be beneficial in the early period of rivaroxaban toxicity in clinic, further studies are required to recommend its routine use.
Spiller et al. [11] reported that no bleeding was observed in acute rivaroxaban toxicity and that bleeding was more associated with long-term treatment. Replinger et al. [34] reported that there was no bleed ing after acute rivaroxaban overdose. No bleeding was observed in a case receiving 1960 mg rivaroxaban who was reported by Lehman et al. [35] and in a case receiving 1400 mg rivaroxaban who was report ed by Linkins et al. [36]. The fact that being no macroscopic or micro scopic hemorrhage in any of 30 mice given a massive dose of rivaroxaban in our study supports this finding.
4.1. Limitations of the study
The toxic effect of rivaroxaban is observed mostly in chronic use. In our experiment, the subjects were sacrificed at the 5th hour following a high dose of rivaroxaban. There was no bleeding or death in the group receiving only a high dose of rivaroxaban. Therefore, the effects of AC and LE at these outcome points could not be assessed. LE could not be applied optimally in experimental animals. Since intravenous ad ministration is not possible in mice, intraperitoneal administration was performed, and no intravenous infusion was given after bolus adminis tration. Lipid emulsion was observed in the peritoneum after sacrification in all experimental animals given LE. It is thought that LE might have not been given at effective doses and therefore sufficient ef fect could might have not been achieved. Also, the number of animals were smallrestricted with 42 subjects in order not to increase animal sacrifice.
Competing interests
The authors declared that they have no competing interests. Acknowledgements
This study received funding from Ufuk University research funds. References
[1] Leroux JC. Injectable nanocarriers for biodetoxification. Nat Nanotechnol 2007; 2(11):679–84.
[2] Levy G. Gastrointestinal clearance of drugs with activated charcoal. N Engl J Med 1982;307(11):676–8.
[3] Juurlink DN. Activated charcoal for acute overdose: a reappraisal. Br J Clin Pharmacol 2016;81(3):482–7.
[4] Damitz R, Chauhan A. Parenteral emulsions and liposomes to treat drug overdose. Adv Drug Deliv Rev 2015;90:12–23.
[5] Lavonas EJ, et al. Part 10: Special Circumstances of Resuscitation: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emer gency Cardiovascular Care. Circulation 2015;132(18 Suppl 2):S501–18.
[6] Ramos-Esquivel A. Monitoring anticoagulant therapy with new oral agents. World J Methodol 2015;5(4):212–5.
[7] Siegal DM, Crowther MA. Acute management of bleeding in patients on novel oral anticoagulants. Eur Heart J 2013;34(7):489–498b.
[8] Roehrig S, et al. Discovery of the novel antithrombotic agent 5-chloro-N- ({ (5S)-2 oxo-3- [4- (3-oxomorpholin-4-yl)phenyl]-1,3-oxazolidin-5-yl}methyl)thiophene 2-carboxamide (BAY 59-7939): an oral, direct factor Xa inhibitor. J Med Chem 2005;48(19):5900–8.
[9] Clearsynth MSDS data sheet. https://s3-us-west-2.amazonaws.com/drugbank/ msds/DB06228.pdf?1368942453.
[10] Perez E, Bania TC, Medlej K, Chu J. Determining the optimal dose of intravenous fat emulsion for the treatment of severe verapamil toxicity in a rodent model. Acad Emerg Med Dec 2008;15(12):1284–9.
[11] Spiller HA, et al. An Observational Study of the Factor Xa Inhibitors Rivaroxaban and Apixaban as Reported to Eight Poison Centers. Ann Emerg Med 2016;67(2):189–95.
[12] Salmela B, et al. Active online assessment of patients using new oral anticoagulants: bleeding risk, compliance, and coagulation analysis. Semin Thromb Hemost 2012; 38(1):23–30.
[13] Eerenberg ES, et al. Reversal of rivaroxaban and dabigatran by prothrombin complex concentrate: a randomized, placebo-controlled, crossover study in healthy subjects. Circulation 2011;124(14):1573–9.
[14] Douxfils J, et al. Non-VKA Oral Anticoagulants: Accurate Measurement of Plasma Drug Concentrations. Biomed Res Int 2015;2015:345138.
[15] Wang X, et al. Effect of activated charcoal on apixaban pharmacokinetics in healthy subjects. Am J Cardiovasc Drugs 2014;14(2):147–54.
[16] Sajkov D, Gallus A. Accidental Rivaroxaban Overdose in a Patient with Pulmonary Embolism: Some Lessons for Managing New Oral Anticoagulants. Clin Med Insights Case Rep 2015;8:57–9.
[17] Shinaberger JH, et al. Dialysis for intoxication with lipid soluble drugs:enhancement of glutethimide extraction with lipid dialysate. Trans Am Soc Artif Intern Organs 1965;11:173–7.
[18] Krieglstein J, Meffert A, Niemeyer DH. Influence of emulsified fat on chlorpromazine availability in rabbit blood. Experientia 1974;30(8):924–6.
[19] Weinberg GL, et al. Pretreatment or resuscitation with a lipid infusion shifts the dose-response to bupivacaine-induced asystole in rats. Anesthesiology 1998; 88(4):1071–5.
[20] Weinberg G, et al. Lipid emulsion infusion rescues dogs from bupivacaine-induced cardiac toxicity. Reg Anesth Pain Med 2003;28(3):198–202.
[21] Dix SK, et al. Intractable cardiac arrest due to lidocaine toxicity successfully resusci tated with lipid emulsion. Crit Care Med 2011;39(4):872–4.
[22] Litz RJ, et al. Successful resuscitation of a patient with ropivacaine-induced asystole after axillary plexus block using lipid infusion. Anaesthesia 2006;61(8):800–1.
[23] Mahedero G, et al. Absorption of Intralipid and interferences from nutrients infused into the peritoneal cavity of the rat. Am J Surg 1992;164:45–50.
[24] Moran J, et al. Transperitoneal absorption of intralipid in rats: total serum fatty acids and triglyceride after absorption. JPEN J Parenter Enteral Nutr 1986;10(6):604–8.
[25] Ferner RE. Our poisoned patients. QJM 2001;94(3):117–20.
[26] Larsen LC, Cummings DM. Oral poisonings: guidelines for initial evaluation and treatment. Am Fam Physician 1998;57(1):85–92.
[27] Zhang L, Leroux JC. Current and forthcoming approaches for systemic detoxification. Adv Drug Deliv Rev 2015;90:1–2.
[28] Insel PA, et al. Introduction to the Theme "New Methods and Novel Therapeutic Ap proaches in Pharmacology and Toxicology". Annu Rev Pharmacol Toxicol 2017 Jan 6; 57:13–7.
[29] Bondeson DP, Crews CM. Targeted Protein Degradation by Small Molecules. Annu Rev Pharmacol Toxicol 2017 Jan 6;57:107–23.
[30] Forster V, Leroux JC. Nano-antidotes for drug overdose and poisoning. Sci Transl Med 2015;7(290):290ps14.
[31] Oney S, et al. Development of universal antidotes to control aptamer activity. Nat Med 2009;15(10):1224–8.
[32] Forster V, Luciani P, Leroux JC. Treatment of calcium channel blocker-induced car diovascular toxicity with drug scavenging liposomes. Biomaterials 2012;33(13): 3578–85.
[33] Zhu Y, et al. Engineering Factor Xa Inhibitor with Multiple Platelet-Binding Sites Fa cilitates its Platelet Targeting. Sci Rep 2016;6:29895.
[34] Repplinger DJ, et al. Lack of significant bleeding despite large acute rivaroxaban overdose confirmed with whole blood concentrations. Clin Toxicol (Phila) 2016; 54(8):647–9.
[35] Lehmann T, et al. Massive human rivaroxaban overdose. Thromb Haemost 2014; 112(4):834–6.
[36] Linkins LA, Moffat K. Monitoring the anticoagulant effect after a massive rivaroxaban overdose. J Thromb Haemost 2014;12(9):1570–1.