Rectal resection for Schnitzler’s metastasis in a patient
presenting with severe rectal stenosis: case report and review
of the literature
Semra Doğan1 , Sezai Demirbaş1 , Elgun Samadov2 , Salih Erpulat Öziş1 , Hatim Yahya Uslu1 1Department of General Surgery, TOBB Economy and Technology University Hospital, Ankara, Turkey
2Department of General Surgery, Tibb Universiteti Nariman Narimanov Baku, Baku, Azerbaijan
ABSTRACT
Rectal metastasis resulting from the hematogenous spread of gastric cancer (Schnitzler’s disease) is rarely seen. We report a case of 53-year-old female with rectal metastasis from gastic cancer who presented with abdominal pain, tenesmus, and severe constipation. Digital rectal examination revealed a severe stenosis 5-6 cm from the dentate line. Sigmoidoscopy showed a narrowed lumen at 5 cm up from the dentate line. The evident radiologic finding was circumferential stenosis of the rectum located at the same level. Very low anterior resection and total mesorectal excision with coloanal anastomosis in addition to protective ileostomy were performed. Pathological examination revealed metastatic adenocarcinoma (Schnitzler’s metastasis). The patient
was discharged on the 9thpostoperative day with no adverse events. It should be kept in mind that rectal stenosis
could be metastasis from gastric carcinoma if consistent with the patient’s history.
Keywords: Schnitzler’s disease, gastric cancer, rectum metastasis
Address for correspondence: Semra Doğan, MD., TOBB Economy and Technology University, Department of General Surgery, Yaşam Cad. No:5,
Söğütözü, 06510 Ankara, Turkey
E-mail: [email protected], phone: +90 312 292 99 39, fax: +90 312 292 9910
Copyright © 2019 by The Association of Health Research & Strategy Available at http://dergipark.gov.tr/eurj
The European Research Journal2019;5(1):196-201
he known routes of distant metastasis after cur-ative gastrectomy include lymphatic spreading (Virchow’s node), peritoneal seeding (Krukenberg’s tumor or Plummer’s rectal shelf) or hematogenous spread (Schnitzler’s metastasis) [1-3]. We present a patient with rare Schnitzler’s metastasis who lived 42 months after curative treatment of gastic cancer.
CASE PRESENTATION
A 53-year-old woman presented with constipation, tenesmus, abdominal pain, and weight loss of 8-9 kg over a period of 2 months. Her past medical history
was significant for signet ring cell gastric adenocarcinoma (T2N0M0), for which she underwent total gastrectomy with D2 lymph node dissection 42 months earlier. Pathological examination at that time showed the surgical resection margins to be clear. Twenty-one lymph nodes were harvested, and were found to be tumor-free. In the follow-up period of 42 months after total gastrectomy, she was admitted to our General Surgery Clinic with constipation, tenesmus, and abdominal pain.
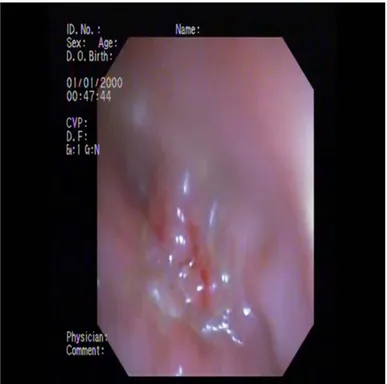
Digital rectal examination revealed severe stenosis 5-6 cm from the dentate line without any mucosal lesion. Blood test results and serum tumor markers were normal. Sigmoidoscopy showed a narrowed
T
CASE REPORT
e-ISSN: 2149-3189
DOI: 10.18621/eurj.378526
lumen at the 5th cm from the dentate line (Figure 1).
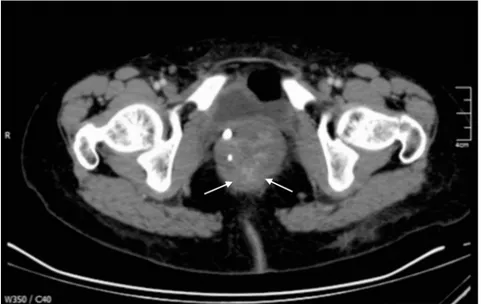
Histopathological examination of the rectal mucosal biopsy did not find any signs of tumoral involvement. Abdominal and pelvic computed tomography (CT) showed circumferential stenosis of the middle rectum (Figures 2 and 3). There were no signs of metastatic involvement in her pelvic area. At positron emission tomography-computed tomography (PET-CT), a high standardized uptake value (SUV) of 5.8
was detected at the upper-middle rectum (Figure 4). The rectal stenosis was defined as rectal fibrosis on the PET-CT scan. The patient’s past medical history and imaging features made us consider the lesion as metastasis of the rectum from gastric malignancy rather than fibrosis; this possibility was more likely than that of primary malignancy.
Informed consent has been taken from the patient. Very low anterior resection (VLAR) and total Figure 1.Sigmoidoscopy showing the narrowed lumen at 5th cm from the dentate line.
Eur Res J 2019;5(1):196-201 Doğan et al
mesorectal excision (TME) with pull-through coloanal anastomosis were performed (Figure 5). In addition, protective ileostomy was done. During the operation, frozen section revealed an unclear malignancy with glandular structure. Nevertheless, the entire abdominal exploration gave no evidence of malignant nodular involvement, either in the abdominal spaces or on the pelvic peritoneal surfaces.
Histopathological examination revealed metastatic adenocarcinoma with the lesion originating with histopathology similar to the gastric cancer, which occured most likely before spreading via the hematologic route.
The patient was discharged on the 9thday after
surgery without any complications. The patient returned home by flying internationally on Figure 3. Axial CT image showing circumferential stenosis of the distal rectum.
Figure 4. At fused PET-CT image, a high standardized uptake value (SUV) of 5.8 at the upper-middle part of rectum is demonstrated.
postoperative day 11. By that time, she had begun to pass her convalescent period. However, at the early stage of that period, she died. The reason has not been clarified to us by her local physician.
DISCUSSION
Gastric cancer is the fourth most commonly diagnosed malignancy and the second most common cause of cancer mortality worldwide [4]. The recurrence patterns after curative surgery for gastric cancer have been described as locoregional recurrence, peritoneal recurrence, and distant metastasis. Hematologic (Schnitzler’s metastasis) or lymphatic spread from gastric cancer to the rectum is quite rare. We found the lesion of the present patient located in the middle-lower part of the rectum adjacent to the muco-subserosal layer. During the operation we did not determine the presence of any serosal exposure of tumor, or peritoneal or pelvic dissemination, or ascites. These findings supported the idea that this patient’s metastatic rectal cancer was due to hematologic or lymphatic dissemination. Therefore, we are reporting this quite unusual case of rectal Schnitzler’s metastasis via a hematogenous route of
gastric adenocarcinoma.
Only ten cases, including the present case, have been reported in the English literature of Schnitzler’s metastasis to the rectum [5-13]. The mean age of the reported patients was 58.2 years. Seven of these patients were female. Schnitzler’s metastasis to the rectum has been encountered synchronously and/or metachronously. Three of these cases in the literature were synchronous and the others, including our case, were metacronous Schnitzler’s metastasis to the rectum. In our patient, metacronous Schnitzler’s metastasis occured 42 months after completion of treatment for gastric adenocarcinoma. In the reported cases, the median disease-free survival after gastrectomy was 38 months (range: 18-72 months) for metachronous metastases [5-12]. The disease-free survival of the present patient was 42 months. The cardinal symptoms of the previously reported cases were constipation, abdominal distension and tenesmus; and in the present case, the cardinal symptoms were severe constipation, abdominal distension and excessive weight loss. In these cases, the most prominent finding was stenosis of the rectum, which did not allow the passage of stool due to the metastatic stenosis, as in our case.
Sigmoidoscopy, colonoscopy and CT with Figure 5. Macroscopic appearance of the resected rectal segment.
Eur Res J 2019;5(1):196-201 Doğan et al
contrast is the most effective diagnostic strategy for reaching a true diagnosis of rectal metastasis. PET-CT can be used to determine whether the rectal lesion is malignant. In a case presented by Lim et al. [8], PET-CT showed hypermetabolic activity in the rectum. In the present case, high SUV 5.8 was detected in the upper-middle rectum, and the rectal stenosis was defined as rectal fibrosis.
The endoscopic appearance of luminal metastasis is variable, but the characteristic features are diffuse circumferential wall thickening and stiffness. Rectal biopsy is generally useful for determining metastatic cancer of the rectum. In our case, rectal biopsy did not give any sign of tumoral involvement.
An expandable metallic stent, lateral decompressive left colostomy, extended Hartmann’s procedure, low anterior resection, and chemotherapy were chosen as methods of treatment for the patients of the previous reports. For our patient, we decided to perform VLAR and TME with pull-through coloanal anastomosis to remove the rectum completely in accordance with the oncologic resection on evaluation of the findings of CT, pelvic MRI and PET-CT. Closure of the protective ileostomy was planned to be accomplished quite a long time later to allow a second look in the abdominal cavity. But the patient unfortunately died after several days in her convascelent time period after she returned to her home by an international flight.
CONCLUSION
Rectal metastasis presenting as rectal fibrosis from gastric cancer is very rare. When a patient with a history of gastric cancer presents with symptoms such as change of bowel habits (tenesmus or constipation) and/or rectal stenosis, even if biopsy results are negative for malignancy, it should be kept in mind that rectal stenosis can possibly originate from Schnitzler’s metastasis resulting from hematogenic spread of a gastric carcinoma in a patient with a relevant history.
Authorship declaration
All authors listed meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors, and all authors
are in agreement with the manuscript.
Informed consent
Written informed consent was obtained from the patients for publication of this case report and any accompanying images.
Conflict of interest
The authors declared that there are no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
REFERENCES
[1] Maehara Y, Hasuda S, Koga T, Tokunaga E, Kakeji Y, Sugimachi K. Postoperative outcome and sites of recurrence in patients following curative resection of gastric cancer. Br J Surg 2000;87:353-7.
[2] Roviello F, Marrelli D, de Manzoni G, Morgagni P, Di Leo A, Saragoni L, et al. Prospective study of peritoneal recurrence after curative surgery for gastric cancer. Br J Surg 2003;90:1113-9.
[3] Niinobu T, Nakagawa S, Itani Y, Nishikawa Y, Amano M, Higaki N, et al. [Rectal stenosis due to Schnitzler metastasis following surgery for gastric cancer -a case successfully treated with TS-1 and CDDP combination chemotherapy]. Gan To Kagaku Ryoho 2005;32:1761-4. [Article in Japanese]
[4] Kamangar F, Dores GM, Anderson WF. Patterns of cancer incidence, mortality and prevalence across five continets: defining priorities to reduce cancer disparities in different geographic regions of the world. J Clin Oncol 2006;24:2137-50. [5] Yamamato M, Matsuyama A, Kameyama T, Okamato M, Okazaki J,Utsunomiya T,.et al. [A case of advanced gastric cancer with Schnitzler’s metastases effectively treated by combination of paclitaxel and S-1]. Gan To Kagaku. Ryhoho 2008;35 829-31. [Article in Japanese]
[6] Olano C, De Simone F, Gonzalez F, Gonzalez N, Tchekmedyian A, Pose A, et al. Stomach cancer presenting with rectal stenosis: Schnitzler’s metastasis. Gastrointest Endosc 2009;70:809-10.
[7] Rausei S, Frattini F, Dionigi G, Boni L, Rovera F, Diurni M. Unusual rectal stenosis. J Surg Oncol 2010;102:713.
[8] Lim SW, Huh JW, Kim YJ, Kim HR. Laparoscopic low anterior resection for hematogenous rectal metastasis from gastric adenocarcinoma: a case report. World J Surg Oncol 2011;9:148. [9] Tural D, Selçukbiricik F, Erçalişkan A, Inanç B, Günver F, Büyükünal E. Metachronous rectum metastases from gastric adenocarcinoma: a case report. Case Rep Med 2012;2012:726841.
[10] Okugawa T, Oshima T, Ikeo K, Kondo T, Tomita T, Fukui H, et al. Successful self-expandable metallic stent placement for a case of distal rectal stenosis due to gastric cancer metastasis.
Case Rep Gastroenterol 2013;7:214-8.
[11] Derici Z.S, Sokmen S. Gastric carcinoma presenting with severe rectal stenosis: ‘Schnitzler’s metastasis’: case report and rewiew of the literature. Eur Surg 2016:48:246-9.
[12] Uemura N, Kurashige J, Kosumi K, Iwatsuki M, Yamashita K, Iwagami S, et al. Early gastric cancer metastazing to thr rectum, possibly via hematogenous route:a case report and review
of the literature. Surg Case Rep 2016:2:58.
[13] Matsutani T, Sasajima K, Amano H, Egami K, Kan H, Myashita M, et al. A case of expandable metallic stent placement for the stenosis in the sigmoid colon and rectum due to Schnitzler’s metastasis from gastric cancer. Gastroenterol Endosc 2005;47:343-7.
This is an open access article distributed under the terms of Creative Common Attribution-NonCommercial-NoDerivatives 4.0 International License.