214
1 Assistant Professor of Urology, Dicle University School of Medicine, Department of Urology, Diyarbakir, Turkey 2 Assistant Professor of Pathology, Dicle University School of Medicine, Department of Pathology, Diyarbakir, Turkey
Yazışma Adresi /Correspondence: Mehmet Nuri Bodakci,
Dicle University School of Medicine, Department of Urology, 21280 Diyarbakir, Turkey Email: [email protected] Geliş Tarihi / Received: 25.09.2013, Kabul Tarihi / Accepted: 07.10.2013
Copyright © Dicle Tıp Dergisi 2014, Her hakkı saklıdır / All rights reserved
Dicle Tıp Dergisi / 2014; 41 (1): 214-216
Dicle Medical Journal doi: 10.5798/diclemedj.0921.2014.01.0402
CASE REPORT / OLGU SUNUMU
A case of a scrotal mesenteric cyst
Skrotal mezenterik kist olgusu
Mehmet Nuri Bodakçı1, Namık Kemal Hatipoğlu1, Uğur Fırat2, Necmettin Penbegül1, Murat Atar1 ÖZET
Mezenterik kistler oldukça nadir görülen intra abdominal kitleler olup, farklı klinik bulgular ve semptomlar ile ortaya çıkabilmektedirler. Mezenter içinde duodenumdan rektu-ma kadar ve retroperitonel olarak yerleşebilmektedirler. Bu vakada 6 yaşında erkek çocukta epididim kistini taklit eden, çok nadir görülen skrotum yerleşimli mesenterik kist olgusunu sunuyoruz. Ultrasonografide skrotumu dol-duran multiloküle kist tesbit edilen hastada, kist cerrahi olarak eksize edildi. Histopatolojik değerlendirmesi şilo-limfatik mesenterik kist olarak tanımlanan hastanın bir yıl-lık takibinde herhangi bir nüks tesbit edilmedi.
Anahtar kelimeler: Mezenterik kist, skrotal kitle,
şilolim-fatik kist
ABSTRACT
Mesenteric cysts are rarely seen intraabdominal mass le-sions which can manifest themselves with different clini-cal signs, and symptoms. They can locate in the mesen-terium from duodenum down to rectum, and also in the retroperitoneal space. Herein we present a very rare case of a scrotal mesenteric cyst which resembled an epididy-mal cyst in a 6-year-old boy. Ultrasonographic examina-tion revealed a multiloculated cyst completely filling the scrotal sac, and the cyst was excised surgically. Histo-pathological examination described the surgical speci-men as chylolymphatic mesenteric cyst, and during one year follow-up any recurrence was not observed.
Key words: mesenteric cyst, scrotal mass,
chylolym-phatic cyst
INTRODUCTION
Mesenteric cysts are rarely seen intraabdominal masses which demonstrate different clinical signs, and symptoms [1]. They are generally benign le-sions, and their incidence has been reported to be 1/100.000 in adults, and 1/20.000 in children [2]. Mesenteric cysts can be seen in the mesentery of bowel segments extending from duodenum, down to rectum. As cited in the literature, nearly half of the reported cases are localized in the small intes-tines, and generally near to the duodenum. However retroperitoneal and omental mesenteric cysts were also reported [3].
Mesenteric cysts are divided into 6 groups based on their histopathological features as [4] cysts originating from: 1. Lymphatic tissue (simple lymphatic cyst and lymphangioma) 2. Mesothelium (simple mesothelial cyst, benign or malign cystic mesothelioma) 3. Intestines (enteric cyst and enteric
duplication cyst) 4. Urogenital structures 5. Mature cystic teratoma (dermoid cysts) 6. Pseudocysts (in-fectious, and traumatic cysts). Among them, most frequently, cysts of lymphatic, and mesothelial ori-gin are encountered. Cysts can contain chylous, se-rous or even hemorrhagic material. In this paper, we aimed to report an isolated scrotal mesenteric cyst in a 6-year-old boy.
CASE REPORT
Family of a 6-year-old boy consulted to the outpa-tient clinics of urology because of a gradually in-creasing scrotal mass in their child within one year. His medical history did not reveal any previous scrotal trauma or surgery. On his physical examina-tion, a cystic mass filling the left side of the scrotum measuring nearly 6 x 7 cm was palpated. Left testis was located separately and inferior to the mass. His urine, and biochemical test results, and whole blood
M. N. Bodakçı et al. Scrotal mesenteric cyst 215
Dicle Tıp Derg / Dicle Med J www.diclemedj.org Cilt / Vol 41, No 1, 214-216
counts were within normal limits. On his scrotal sonographic examination, a septated, cystic mass located in the left side of the scrotum with dimen-sions of 6 x 7 cm was detected. Whole abdominal ultrasonographic examinations were unremarkable. Surgical exploration was planned with initial diag-nosis of epididymal cyst.
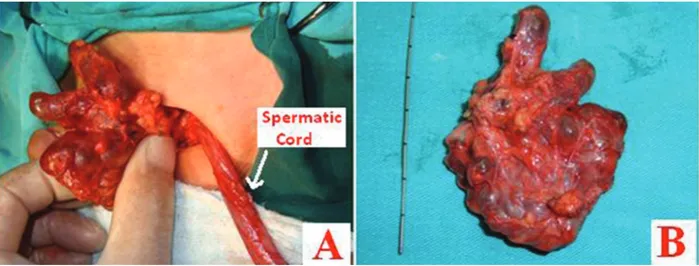
General anesthesia was preferred for surgical exploration. Through a left inguinal incision scrotal sac was entered. Cystic mass was separated from scrotum, and testis with blunt, and sharp dissection, and taken out. During the surgical excision, unusu-ally easy separation of the mass from surrounding structures with blunt dissection, lack of any
link-age with testis, and epididymis, and termination of the cyst in the upper inguinal region without any communication with any structure were noted as remarkable findings (Figure 1). A penrose drain was placed inside scrotum, and incised layers were closed with appropriate sutures, and then the surgi-cal procedure was terminated. On the postoperative first day, penrose drain of the patient was removed, and the patient was recovered without development of any complication. Histopathological evalua-tion disclosed a mesenteric cyst, resembling a thin walled chylous cyst with an endothelial lining (Fig-ure 2).
Figure 1. A: The cyst ends separately from the spermatic chord via inguinal incision. B: Multiloculated cyst
Figure 2. Mesenteric cyst resembling chylous cyst with a
thin wall and lined by endothelium (H&E stain, x100) DISCUSSION
Mesenteric cysts are seen in only 1 of 27.000-250.000 referrals to hospitals [4]. It was reported in all age groups, and encountered in 75 % of adult,
and 25 % of pediatric cases [2]. Some confounding factors involve in the definition, and classification of mesenteric cysts Omentum, mesentery, and all retroperitoneal membranes develop from the same embryologic origin. These anatomical structures which extend from posterior wall of the abdomen are formed of two layers which contain adipose, connective, and musculo-nervous tissue, and carry blood, and lymph vessels of the abdominal organs. Cysts which develop in these tissues are described as mesenteric cysts [5].
Mesenteric cysts are largely asymptomatic. Rarely, they can manifest themselves with signs of abdominal distension, pain or mass. On the other hand, they can confront us with many complications as torsion, intestinal obstruction, bleeding, infec-tion, rupture, and compression on adjacent organs [6].
M. N. Bodakçı et al. Scrotal mesenteric cyst 216
Dicle Tıp Derg / Dicle Med J www.diclemedj.org Cilt / Vol 41, No 1, 214-216
Rattan et al published a series of 8 cases aged between 18 months and 10 years whose cysts were defined histopathologically as chylolymphatic cysts. Abdominal swelling was detected in all these cases, and their physical examination revealed a palpable abdominal mass in 5 cases. Symptoms of acute intestinal obstruction (n=2), and abdominal pain (n=2) were prominent in 4 cases. They reported that all cases were laparotimized, and multiloculated cysts with diameters ranging between 8 mm, and 9 cm localized on the mesentery of the small intestine were detected [7]. Ghazimoghadam et al published a case report of a 19-year-old healthy male patient who had complained of an urgent urinary retention caused by a mesenteric cyst. Following resection of the mesenteric cyst, the patient had completely re-lieved of his urinary complaints [1]. Okur et al in their study including 10 pediatric cases, reported that their patients referred frequently with symp-toms of abdominal swelling, and pain at admission to the hospital, and they had detected a palpable ab-dominal mass in 4 patients [3]. They had performed laparotomy, and cyst excision in all cases, and de-tected intestinal mesenteric (n=6), retroperitoneal (n=2), omental (n=1), and mesosigmoidal (n=1) cysts. In our case a painless mass filling the left side of the scrotum was present which was diagnosed as multiloculated cyst on US.
Mesenteric cysts are managed by surgical ex-cision. Although successful cases of laparoscopic
cystectomy were reported in the literature, total cystectomy by open surgery is preferred more fre-quently [7]. Excluding operational risks, prognosis is relatively good with lower recurrence rates [3]. In our case, any evidence of recurrence was not ob-served in none of our patients during one year of follow-up period.
Rarely mesenteric cysts involve scrotum pri-marily, however this benign abnormality should be kept in mind in the evaluation and differential diag-nosis of scrotal masses encountered in the pediatric age group.
REFERENCES
1. Ghazimoghadam B, Rajaie S. Urinary retention due to mes-enteric cyst: An extremely unusual presentation of a rare complication. Indian J Nephrol 2008;18:24-25.
2. Kurtz RJ, Heimann TM, Holt J, et al. Mesenteric and retro-peritoneal cysts. Ann Surg 1986;203:109-112.
3. Okur H, Kucukaydin M, Ozokutan BH, et al. Mesenteric, omental, and retroperitoneal cysts in children. Eur J Surg 1997;163:673-677.
4. de Perrot M, Brundler M, Totsch M, et al. Mesenteric cysts. Toward less confusion? Dig Surg 2000;17:323-328. 5. Vanek VW, Phillips AK: Retroperitoneal, mesenteric, and
omental cysts. Arch Surg 1984;119:838-842.
6. Walker AR, Putnam TC: Omental, mesenteric, and retroperi-toneal cysts: a clinical study of 33 new cases. Ann Surg 1973;178:13-19.
7. Rattan KN, Nair VJ, Pathak M, et al. Pediatric chylolymphat-ic mesenterchylolymphat-ic cyst - a separate entity from cystchylolymphat-ic lymphan-gioma: a case series. J Med Case Rep 2009;3:111.