www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Long-term
follow-up
of
tonsillectomy
efficacy
in
children
with
PFAPA
syndrome
夽
Ozturk
Aktas
a,
Hande
Gurbuz
Aytuluk
b,∗,
Sebla
Kumas
Caliskan
c,
Omer
Erdur
d,
Ahmet
Adnan
Cirik
eaKocaeliStateHospital,DepartmentofOtolaryngology,Kocaeli,Turkey
bKocaeliStateHospital,DepartmentofAnesthesiologyandReanimation,Kocaeli,Turkey cDerinceTrainingandResearchHospital,DepartmentofOtolaryngology,Kocaeli,Turkey dSelcukUniversity,DepartmentofOtolaryngology,Konya,Turkey
eUmraniyeTrainingandResearchHospital,DepartmentofOtolaryngology,Istanbul,Turkey
Received20September2017;accepted27October2017 Availableonline21November2017
KEYWORDS Fever; Lymphadenitis; Stomatitisaphthous; Pharyngitis; Tonsillectomy Abstract
Introduction:Theroleoftonsillectomyintheperiodicfever,aphthousstomatitis,pharyngitis,
andadenitissyndrome,iscontroversial.Althoughsomestudiesreportedhighsuccessrateswith tonsillectomy,furtherinvestigationsareneededwithlargernumbersofpatients.
Objective:Toseekthelong-termoutcomesoftonsillectomyinperiodicfever,aphthous
stoma-titis,pharyngitis,andadenitissyndrome.
Methods:Caseseries;multi-centerstudy.Thestudycomprised23patientswithperiodicfever,
aphthousstomatitis,pharyngitis,andadenitissyndromewhounderwentsurgery(tonsillectomy withorwithoutadenoidectomy)betweenJanuary2009andNovember2014.
Results:21(91%)of23patientshadcompleteresolutionimmediatelyaftersurgery.Onepatient
hadanattack24haftersurgery,buthashadnofurtherattacks.Onepatienthadthreeattacks withvariousintervals,andcompleteremissionwasobservedafter3months.
Conclusions:Tonsillectomyisagoodoptionforthetreatmentofperiodicfever,aphthous
sto-matitis,pharyngitis,andadenitissyndrome.
© 2017 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
夽 Pleasecitethisarticleas:AktasO,AytulukHG,CaliskanSK,ErdurO,CirikAA.Long-termfollow-upoftonsillectomyefficacyinchildren withPFAPAsyndrome.BrazJOtorhinolaryngol.2019;85:78---82.
∗Correspondingauthor.
E-mail:[email protected](H.G.Aytuluk).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial. https://doi.org/10.1016/j.bjorl.2017.10.012
1808-8694/©2017Associac¸˜aoBrasileiradeOtorrinolaringologiaeCirurgiaC´ervico-Facial.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(http://creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE Febre; Linfadenite; Estomatiteaftosa; Faringite; Tonsilectomia
Acompanhamentoemlongoprazodaeficáciadatonsilectomiaemcrianc¸ascom síndromedePFAPA
Resumo
Introduc¸ão: Opapeldatonsilectomianasíndromedafebreperiódica,estomatiteaftosa,
farin-giteeadeniteécontroverso.Emboraalgunsestudostenhamrelatadoaltastaxasdesucesso comatonsilectomia,sãonecessáriasmaispesquisascomumnúmeromaiordepacientes.
Objetivo: Avaliarosresultadosemlongoprazodatonsilectomianasíndromedefebreperiódica,
estomatiteaftosa,faringiteeadenite.
Método: Sériedecasos;estudomulticêntrico. Oestudoavaliou23 pacientescomsíndrome
defebreperiódica,estomatiteaftosa,faringiteeadenitesubmetidosacirurgia(tonsilectomia comousemadenoidectomia)entrejaneirode2009enovembrode2014.
Resultados: Dos23pacientes,21(91%)apresentaramresoluc¸ãocompletaimediatamenteapós
acirurgia.Umpacienteapresentouumepisódio24horasapósacirurgia,massemrecorrência posterior. Umpaciente teve trêsepisódios comvários intervalos earemissão completafoi observadaapós3meses.
Conclusões: Atonsilectomiaéumaboaopc¸ãoparaotratamentodasíndromedefebre
per-iódica,estomatiteaftosa,faringiteeadenite.
© 2017 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
The Periodic Fever, Aphthous Stomatitis, Pharyngitis, and
CervicalAdenitis (PFAPA)syndrome wasfirstdescribed by
Marshalletal.in19871;however,itscauseisstillunknown.
Itusuallybegins beforetheage of5 years,and ends
pre-puberty. The main symptom of this syndrome is episodes
of feverthat lastfor 3---6 dayswithrecurrenceevery3---8
weeks. One or more of following symptoms can be seen
during an attack: aphthous stomatitis, pharyngitis, and
cervical adenopathy. Rarely, patients experience rashes,
headaches, abdominal pain or arthralgia. Patients are
asymptomatic between episodesand show normal growth
anddevelopment.
TheroleoftonsillectomyinPFAPAsyndromeis
controver-sial.Althoughsomestudiesreportedhighsuccessrateswith
tonsillectomy,furtherinvestigationsareneededwithlarger
numbersofpatients.Inthisstudy,wereporttheefficacyof
tonsillectomyinPFAPAsyndromein23children.
Material
and
methods
Twenty-threepatientswithPFAPAsyndromewhounderwent
surgery (tonsillectomywith or without adenoidectomy)at
three different hospitals (Kocaeli State Hospital, Golcuk
Government Hospital, and Derince Training and Research
Hospital) in Kocaeli, between January 2009 and
Novem-ber 2014, were identified. All patients were diagnosed
according to PFAPA criteria established by Thomas and
colleagues.2 Each patient had regularly recurring fevers
with an early age of onset (less than five years of age),
symptomsintheabsenceof upperrespiratorytract
infec-tion, with at least one of aphthous stomatitis, cervical
lymphadenitis, and pharyngitis, completely asymptomatic
intervalsbetweenepisodes,andnormalgrowthand
devel-opment. All of 23 patients were monitored during each
episodefor6monthsbeforesurgery,andfolloweduponce
amonth at least for 12months aftersurgery. Twenty-one
patients underwent adenotonsillectomy and two patients
underwenttonsillectomywithoutadenoidectomybecauseof
theabsenceofobstructivesymptomsandclinicalfindings.
Preoperativecompletebloodcellcountswereobtained
dur-ingall febrile episodesto exclude cyclic neutropenia.No
abnormalchangeswere observed inthe routine
biochem-istry analyses. All of the patients’ vitamin D levels were
withinnormalrange.Patientswerereferredtothepediatric
clinicbeforesurgery.
ThestudywasapprovedbytheKocaeliUniversityEthics
CommitteeofNoninvasive Investigations(26.04.2017;
pro-tocolno.2017/130;decreeno.2017/6.25)andtheparents
ofeachchildincludedinthestudywereinformedaboutthe
aimof thestudy andasked for written informedconsent
beforeinclusioninthestudy.
Results
Twenty-three patients (14 males, 9 females) with PFAPA
syndrome,aged between 36 months and84 months were
includedinthestudy.Theaverageageofsymptomonsetwas
27months(range,12---36months).Episodesrecurredevery
3---8weeks(mean:3.9weeks).Duringepisodes,fever was
observedfor a mean of 3.7days. Pharyngitis(18/23) was
the most common clinical manifestation. Cervical
adeni-tis (14/23) and aphthous stomatitis (10/23) were also
observed.Themeanage atthetimeofsurgery
(tonsillec-tomywithorwithoutadenoidectomy)was50months(range,
36---84months).Nomajorcomplicationswereobservedafter
surgery.Allpatientscompletedthestudy.Ofthe23patients,
21 had complete symptom resolution immediately after
surgery.Onlytwopatientsdidnothaveresolutionoffevers
aftersurgery.Onepatienthadanattack24haftersurgery,
Table1 Preoperativedemographicandclinical character-isticsofPFAPApatients.
Characteristic PFAPApatients(n=23) Male;n(%) 14(61%)
Female;n(%) 9(39%) Ageatonset;mean(range),
months
27(12---36) Recurrenceofepisodes;mean
(range),weeks
3.9(3---8) Durationoffever;mean
(range),days
3.7(3---5) Pharyngitis;n(%) 18(78%) Cervicaladenitis;n(%) 14(61%) Aphthousstomatitis;n(%) 10(43%) Ageatsurgery;mean(range),
months
50(36---84)
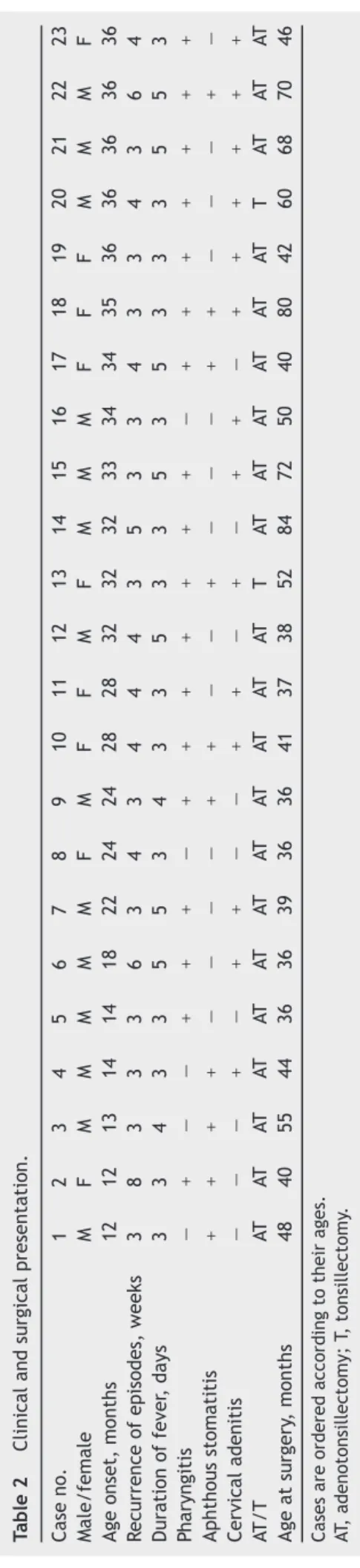
threeattackswithvariousintervals,andcompleteremission wasobservedafterthreemonths(case18).The demograph-icsandclinicalcharacteristicsofthepatientsarepresented inTables1and2.
Discussion
PFAPA syndrome can be diagnosed by the exclusion of
other causes of regular, repeated episodes of fever, such
ascyclicneutropenia,FamilialMediterraneanFever(FMF),
hyperglobulinemiaD syndrome, Behcet’sdisease, juvenile
rheumatoid arthritis, and autosomal dominant Hereditary
PeriodicFeversyndrome(HPF).2,3Webelievethatthemost
importantcriterionofstudiesabout PFAPAsyndromemust
bepatientselection.Accordingly,wepaidgreatattentionto
patientselectioninourstudy.Inmoststudies,weseethat
manypatientsdonotmeetallPFAPAsyndromecriteria.In
contrast,all diagnosesin thepresent studywere madein
accordancewiththePFAPAcriteriaestablishedbyThomas
etal.2Completebloodcellcountswereobtainedduringall
febrileepisodestoexcludecyclicneutropenia.Throat
cul-tureswerenegativeforallpatientsduringattacks.Patients
werereferredtothepediatricclinictoexcludeothercauses.
The unknown pathogenesis of PFAPA syndrome causes
uncertaintyin itstreatment. Therearefew studies about
thetreatmentofthissyndrome.Thesuggestedtreatments
consistofconservative(pharmacologic)therapiesand
sur-gicalintervention.Treatment withcorticosteroids appears
tobe the most effective nonsurgical therapy. Prednisone
(1---2mg/kg) or betamethasone(0.1---0.2mg/kg) are
effec-tiveagentsforabortingfeverattackswithinafewhours.4---6
However,othersymptomscantakelongertoresolve.No
sys-temictoxicityor adverseeffects relatedwiththesedoses
ofcorticosteroidshavebeenreported.Thedisadvantageof
corticosteroid therapy is that it does not prevent future
fever attacks and can evenshorten the interval between
attacks.4,7---10 Steroidresponsemaybeusefulin
distinguish-ingPFAPA episodesfromother differentialdiagnosessuch
asFMForHPF,5,11andcanbeusedforadditionaldiagnostic
criteria.12Despitethefactthatsteroidsarethemost
effec-tivedrugsforthetreatmentofsymptoms,wedonotbelieve
thattheyareagoodoptionforlong-termusebecausethey T
able 2 Clinical and surgical presentation. Case no. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 Male/female M F M M M M M F M F F M F M M M F F F M M M F Age onset, months 12 12 13 14 14 18 22 24 24 28 28 32 32 32 33 34 34 35 36 36 36 36 36 R ecurrence of episodes, weeks 3 8 3 3 3 6 3 4 3 4 4 4 3 5 3 3 4 3 3 4 3 6 4 Duration of fever , days 3 3 4 3 3 5 5 3 4 3 3 5 3 3 5 3 5 3 3 3 5 5 3 P haryngitis − + − − + + + − + + + + + + + − + + + + + + + Aphthous stomatitis + + + + − − − − + + − − + − − − + + − − − + − Cervical adenitis − − − + − + + − − + + − + − + + − + + + + + + A T/T AT AT AT AT AT AT AT AT AT AT AT AT T AT AT AT AT AT AT T AT AT AT Age at surgery , months 48 40 55 44 36 36 39 36 36 41 37 38 52 84 72 50 40 80 42 60 68 70 46 Cases are ordered according to their ages. AT , adenotonsillectomy; T, tonsillectomy .
donot solvethe rootof the problemor prolongintervals betweenfebrileepisodes.
Colchicine is a good drug for reducing inflammation. Oral colchicine 0.5---1mg per day may reduce fever fre-quency.Likesteroids,colchicinedoesnotprovidecomplete remission.13TherationalefortheuseofcolchicineinPFAPA
prophylaxis isbased onclinicalandlaboratory similarities
betweenFMFandPFAPA.Accordingly,ifcolchicineis
effec-tiveinapatientwithPFAPA,adifferentialdiagnosisofFMF
hastobeconsidered.4,13---15
Cimetidine has immune-modulating effects through
the inhibition of chemotaxis and T-cell activation. Oral
cimetidine 20---40mg/kg per day can also be used for
prophylaxis.2,16 However studies showed that cimetidine
therapydoesnotpromisemuchhope.5,13,17,18
Interleukin-1playsakeyrolein PFAPApathogenesis.In
a small sample, it wasshown that a single subcutaneous
injectionofanakinradramaticallyimprovedboththe
clini-calpicture andlaboratory parameters.6,19,20 Atthispoint,
further investigations are needed with larger numbers of
patients.
InadditiontothefindingsthatvitaminDlevelsare
asso-ciatedwithinflammatorydisorders,vitaminDisconsidered
to be a possible regulator of inflammation.21 Stagi et al.
andMahamidetal.foundasignificantcorrelationbetween
PFAPAandvitaminDdeficiencyintheirstudies;asignificant
reductioninthefrequencyoffebrileepisodeswasobserved
inpatientsaftervitaminDsupplementation.22,23Inspiteof
theselimiteddata,itisnotpossibletoconcludethatvitamin
DiseffectiveinPFAPAsyndrome.
The role of surgery in the treatment of PFAPA
syn-drome is still controversial. Although PFAPA syndrome
is a self-limiting disease, tonsillectomy with or without
adenoidectomy as a surgical procedure, seems to be a
goodoption for treating PFAPA.Several studies previously
reportedhighsuccess rates withtonsillectomy.Contrarily,
a long-term observational study that compares efficacy
of tonsillectomy and medical treatment (prednisone and
non-steroidal anti-inflammatory drugs) showed no
signifi-cantdifferencebetweenthetwomethods.24Unfortunately,
unpredictable but finite periods of recurrent episodes at
predictableintervalsrequiretimeoffschoolandbeing
pre-scribed regular medicationduring this periodcanbe very
traumaticforpatientsandparents.25
Abramson was the first author to report the efficacy
of tonsillectomy in four children withPFAPA in 1989.26 In
2000,a retrospectivestudy wasconductedbyDahn etal.
thatincludedfivepatientswhounderwenttonsillectomyand
nonehadanyattacksaftersurgery.27 Anotherstudy
includ-ing 15 patients by Galanakis et al. showed 100% success
after tonsillectomy.3 Afterwards, a randomizedcontrolled
trial that compared14 patients whounderwent
tonsillec-tomy and 12 non-surgical control patients was conducted
byRenkoetal.28Thesyndromeresolvedimmediatelyinall
14 patients whounderwent surgery; in contrast,the
syn-dromeresolvedspontaneouslywithin6monthsin6patients
who had no surgery. However, a weakness of their study
was that most patients did not actually fulfill the PFAPA
criteria.Inaretrospectiveanalysisof9patientswho
under-wenttonsillectomybyWongetal.,completeremissionwas
achievedimmediately in8 patients,andthe frequencyof
attacksweredecreasedinthepatientwhodidnotachieve
immediate remission.29 In Garavello et al.’s prospective
randomizedcontrolled trial, 39 patients withPFAPA were
included.30 Nineteen patients underwent
adenotonsillec-tomyand 20weretreated withmedicaltherapy.After18
months’post-surgicalfollow-up,theauthorsobserved
com-pleteresolutioninallpatientswhounderwentsurgery;only
onepatientinthecontrolgroupshowedspontaneous
reso-lution.Pignataroetal.performedarandomizedcontrolled
trial,31including18patientswithPFAPA,whoweredivided
into two groups; 9 surgical patients and 9 non-surgical
patients. All of the nine surgical patients showed
symp-tomaticimprovement,withcompleteclinicalrecoveryin5
patients,andasignificantreductionoffrequencyand
dura-tionoffeverepisodesintheremainingfour.Ofthe9patients
inthenon-surgerygroup,eighthadcontinuedrelapseand
remissionperiods,andoneofthesepatientswasscheduled
forsurgery.Theninthpatientwaslosttofollow-up.Licameli
etal. demonstratedcompletesymptom cessationin 26of
27patientsaftersurgeryinaprospectivestudyin2008;the
childwhocontinuedtohavefebrileepisodeshadtumultuous
intervals.8 Another prospective study by Licamelli et al.
evaluatedthe long-termefficacyof adenotonsillectomyin
102patients with a widerange of ages(18 months to18
years)in 2012.32 Ninety-ninepatients had complete
reso-lutionimmediatelyaftersurgery,andonepatientachieved
resolutionsix monthsafter surgery. Of theremaining two
patients,onecontinuedtohaveepisodesandtheotherwas
further investigated and diagnosed ashaving mevalonate
kinasedeficiency.
Wethinkthatourstudyshowsthatsurgeryis an
effec-tivetreatmentoptionforPFAPAsyndrome.Twenty-one(91%)
of23 patients hadcomplete resolutionimmediately after
surgery.Onepatienthad anattack 24h aftersurgery, but
hashadno furtherattacks.It ispossible that thepatient
underwentsurgeryattheoverlappingtimeofasubclinical
attack.Onepatienthadthreeattackswithvariousintervals,
butachievedacompleteremissionafter3months.Ourstudy
islimitedbynothavingacontrolgroupforcomparison.
Conclusion
PFAPAresolvesspontaneouslyandtreatmentcanbe
admin-isteredtotrytoreducetheseverityofindividualepisodes.
Pharmacological therapies reduce attack duration but do
notpreventfuturefeverattacks.Asecondoptionis
tonsil-lectomy.Tonsillectomyis, however,an invasive treatment
and the child’s parents must weigh the risks and
conse-quencesof surgery. The high success rateof future fever
attackpreventionshowsusthattonsillectomy(withor
with-outadenoidectomy)isagoodalternativeforthetreatment
ofPFAPA.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.MarshallGS, Edwards KM,ButlerJ,LawtonAR. Syndromeof periodicfever,pharyngitis,andaphthousstomatitis.JPediatr. 1987;110:43---6.
2.ThomasKT,FederHMJr,LawtonAR,EdwardsKM.Periodicfever syndromeinchildren.JPediatr.1999;135:15---21.
3.Galanakis E,PapadakisCE,Giannoussi E,KaratzanisAD, Bit-soriM,HelidonisES.PFAPAsyndromeinchildrenevaluatedfor tonsillectomy.ArchDisChild.2002;86:434---5.
4.Padeh S, Brezniak N, Zemer D, Pras E, Livneh A, Langevitz P,et al. Periodic fever,aphthousstomatitis,pharyngitis and adenopathysyndrome:clinicalcharacteristicsandoutcome.J Pediatr.1999;135:98---101.
5.Feder HM, Salazar JC. A clinical review of 105 patients with PFAPA (a periodic fever syndrome). Acta Paediatr. 2010;99:178---84.
6.StojanovS,LapidusS,ChitkaraP,FederH,SalazarJC,Fleisher TA,etal.Periodicfever,aphthousstomatitis,pharyngitis,and adenitis(PFAPA)isadisorderofinnateimmunityandTh1 acti-vation responsive to IL-1 blockade. Proc Natl AcadSci USA. 2011;108:7148---53.
7.Tasher D, Somekh E, Dalal I. PFAPA syndrome: new clinical aspectsdisclosed.ArchDisChild.2006;91:981---4.
8.LicameliG,JeffreyJ,LuzJ,JonesD,KennaM.Effectof adeno-tonsillectomyinPFAPAsyndrome.ArchOtolaryngolHeadNeck Surg.2008;134:136---40.
9.PeridisS,PilgrimG,KoudoumnakisE,AthanasopoulosI,Houlakis M,ParpounasK.PFAPAsyndromeinchildren:ameta-analysison surgicalversusmedicaltreatment.IntJPediatr Otorhinolaryn-gol.2010;74:1203---8.
10.Forsvoll J, Kristoffersen EK, Oymar K. Incidence, clinical characteristicsandoutcomeinNorwegianchildrenwith peri-odic fever, aphthous stomatitis, pharyngitis and cervical adenitis syndrome: a population-based study. Acta Paediatr. 2013;102:187---92.
11.Padeh S, Stoffman N, Berkun Y. Periodic fever accompanied byaphthousstomatitis pharyngitisand cervical adenitis syn-drome(PFAPAsyndrome)inadults.IsrMedAssocJ.2008;10: 358---60.
12.Hofer M, Pillet P, Cochard MM, Berg S, Krol P, Kone-Paut I, et al. International periodic fever, aphthous stomatitis, pharyngitis,cervicaladenitissyndromecohort:descriptionof distinct phenotypes in301 patients. Rheumatology(Oxford). 2014;53:1125---9.
13.TasherD,SteinM,DalalI,SomekhE.Colchicineprophylaxisfor frequentperiodicfever,aphthousstomatitis,pharyngitisand adenitisepisodes.ActaPaediatr.2008;97:1090---2.
14.ButbulAvielY,TatourS,GershoniBaruchR,BrikR.Colchicine asatherapeuticoptioninperiodicfever,aphthousstomatitis, pharyngitis,cervicaladenitis(PFAPA)syndrome.SeminArthritis Rheum.2016;45:471---4.
15.Dusser P,Hengten V,Neven B, Koné-Paut I. Is colchicinean effective treatment in periodic fever, aphthous stomatitis, pharyngitisandcervicaladenitis(PFAPA)syndrome?JointBone Spine.2016;83:406---11.
16.FederHM.Cimetidinetreatmentforperiodicfeverassociated with aphthous stomatitis, pharyngitis and cervical adenitis. PediatrInfectDis.1992;11:318---21.
17.WursterVM,Carlucci JC, FederHM,Edwards KM. Long-term follow-up of children with periodic fever, aphthous stoma-titis, pharyngitis and cervical adenitis syndrome. J Pediatr. 2011;159:958---64.
18.TerHaarN,LachmannH,ÖzenS,WooP,UzielY,ModestoC, et al. Treatmentof autoinflammatory diseases: resultsfrom theEurofeverRegistryandaliteraturereview.AnnRheumDis. 2013;72:678---85.
19.Stojanov S, Hoffmann F,Kéry A, Renner ED, Hartl D,Lohse P,etal.CytokineprofileinPFAPAsyndromesuggests continu-ousinflammationandreducedanti-inflammatoryresponse.Eur CytokineNetw.2006;17:90---7.
20.FredianaB,CantariniL,VitaleA,GaleazziM.Acaseofresistant adult-onsetperiodicfever,aphthousstomatitis,pharyngitisand cervicaladenitis(PFAPA)syndromeresponsivetoanakinra.Clin ExpRheumatol.2012;30:593.
21.ManginM,SinhaR,FincherK.InflammationandvitaminD:the infectionconnection.InflammRes.2014;63:803---19.
22.MahamidM,AgbariaK,MahamidA,NseirW.VitaminDlinkedto PFAPAsyndrome.IntJPediatrOtorhinolaryngol.2013;77:362---4. 23.StagiS, Bertini F,Rigante D,Falcini F.Vitamin D levelsand effectsofvitaminDreplacementinchildrenwithperiodicfever, aphthousstomatitis,pharyngitis,andcervicaladenitis(PFAPA) syndrome.IntJPediatrOtorhinolaryngol.2014;78:964---8. 24.VigoG,MartiniG,ZoppiS,VittadelloF,ZulianF.Tonsillectomy
efficacyinchildrenwithPFAPAsyndromeiscomparabletothe standardmedicaltreatment:along-termobservationalstudy. ClinExpRheumatol.2014;32:156---9.
25.BurtonMJ,Pollard AJ,RamsdenJD,ChongLY,VenekampRP. Tonsillectomyforperiodicfever,aphthousstomatitis, pharyngi-tisandcervicaladenitissyndrome(PFAPA).CochraneDatabase SystRev.2014;9:CD008669.
26.AbramsonJSTJ,GivnerLB.Possibleroleoftonsillectomyand adenoidectomy in children with recurrent fever and tonsil-lopharyngitis.PediatrInfectDis.1989;8:119---20.
27.DahnKA,GlodeMP,ChanKH.Periodicfeverandpharyngitisin youngchildren: anew diseasefor theotolaryngologist? Arch OtolaryngolHeadNeckSurg.2000;126:1146---9.
28.RenkoM,SaloE,Putto-LaurilaA,SaxenH,MattilaPS, Luoto-nenJ,et al.ARandomized,controlledtrialoftonsillectomy inperiodicfever,aphthousstomatitis,pharyngitis,andadenitis syndrome.JPediatr.2007;151:289---92.
29.WongKK,FinlayJC,MoxhamJP.RoleoftonsillectomyinPFAPA syndrome.ArchOtolaryngolHeadNeckSurg.2008;134:16---9. 30.GaravelloW,RomagnoliM,GainiRM.Effectivenessof
adenoton-sillectomyinPFAPAsyndrome:arandomizedstudy.JPediatr. 2009;155:250---3.
31.Pignataro L, Torretta S, Pietrogrande MC, Dellepiane RM, PavesiP,BossiA,etal.Outcomeoftonsillectomyinselected patients withPFAPA syndrome. Arch Otolaryngol Head Neck Surg.2009;135:548---53.
32.LicameliG,LawtonM,KennaM,DedeogluF.Long-term surgi-caloutcomesofadenotonsillectomyforPFAPAsyndrome.Arch OtolaryngolHeadNeckSurg.2012;138:902---6.