BEYKENT UNIVERSITY
ARCHIVES OF HEALTH SCIENCE AND RESEARCH
Editors:
Prof. Dr. Derman KÜÇÜKALTAN
İzmir Kavram Vocational School Manager, İzmir
Assoc. Prof. Dr. Alper KARAGÖZ
Usak University, Molecular Biology and
Genetic Department, Microbiology, Usak
Prof. Dr. Ayşegül KAPTANOĞLU
Beykent University, Istanbul
U
Ş
A
K
U
N I V ER
S
IT
Y
BEYKENT UNIVERSITY
ARCHIVES OF HEALTH
SCIENCE AND
RESEARCH
Editor
Prof. Dr. Derman KÜÇÜKALTAN
İzmir Kavram MYO
Editors
Assoc. Prof. Dr. Alper KARAGÖZ
Usak University
Prof. Dr. Ayşegül KAPTANOĞLU
Organizing Committee Members
Aslı DURMUŞ
Usak University
Şule OLGUN
İzmir Kavram MYO
Okan Anıl AYDIN
Izmir Kavram Vocational School
E-ISBN : 978-975-6319-54-3
BEYKENT UNİVERSİTY PUBLİCATİONS,
PUBLİCATİON NUMBER : 153
USAK, 2020
PUBLICATION RIGHTS
All publishing rights of this book are reserved. It cannot be reproduced, published or
distributed without the permission of the publisher, except for short excerpts for promotional
PREFACE
Beykent University Archives of Health Science and Research book which was created
with great devotion, experiences and valuable works of academicians has been published. I
would like to thank our authors who contributed to the publication of this book, to
administration of Uşak University, Beykent University, and İzmir Kavram Vocational School
for their support, and of course to our students who will carry us to the future, as well as to
my wife Öznur Karagöz and my daughters Işıl and İnci for their support and encouragement.
Yours sincerely.
Assoc. Prof. Dr. Alper KARAGÖZ
Aralık, 2020
CONTENTS
THE CHANGING PROCESS OF THE HEALTH CARE DURING AND AFTER
PANDEMIC: ROLE OF FAMILY PHYSICIAN ...7
NOTIFIABLE PARASITIC DISEASES IN TURKEY ... 15
THE EVALUATION OF ADOPTION AND SUCCESS OF HEALTHCARE
INFORMATION SYSTEMS ... 26
SEXUALITY AND NURSING IN ONCOLOGICAL DISEASES ... 40
EVALUATION OF PSYCHOLOGICAL AND PHYSIOLOGICAL EFFECTS OF
ERGONOMICS ON OFFICE WORKERS: A PRACTICE ON ACADEMIC AND
ADMINISTRATIVE STAFF OF USAK UNIVERSITY ... 50
PARACETAMOL INDUCED HEPATOTOXICITY/NEPHROTOXICITY AND
OXIDATIVE STRESS ... 59
ARTIFICIAL INTELLIGENCE AND ROBOTIC TECHNOLOGIES IN BRAIN
SURGERY ... 64
THE USE OF THEORIES IN MODERN NURSING EDUCATION ... 69
THE MAIN FAULT SOURCE OF CLINICAL LABORATORIES: PREANALYTIC
PHASE ... 78
ANTIBIOTIC RESISTANCE AND BIOFILMS ... 84
EVIDENCE-BASED MEDICINE ... 92
HIP JOINT (ARTICULATIO COXAE = ARTICULAXIO COXAFEMORALIS)100
PROBIOTIC NUTRITIONS, HEALTH AND OBESITY ... 105
THE CHANGING PERCEPTION OF HEALTH WITH THE NEW CORONAVIRUS
(COVID-19) PANDEMIC ... 122
HEALTHCARE PROFESSIONALS' PERCEPTIONS OF ARTIFICIAL
INTELLIGENCE ... 137
VIEWS OF NURSING SCHOOL STUDENTS ON BEING A NURSE DURING THE
COVID-19 PANDEMIC ... 146
SCIATIC NERVE (NERVUS ISCHIADICUS) ... 158
MOLECULAR TYPING OF SALMONELLA STRAINS ... 162
THE USE OF VIRTUAL REALITY IN CONTROL OF PAIN AND ANXIETY DUE
TO INTERVENTIONAL PROCEDURES ... 171
BIOTECHNOLOGY AND BIOMATERIAL USE IN HEALTH ... 179
NEGATIVE EFFECTS OF OBESITY ON KIDNEYS... 182
BACTERIOLOGICAL MOLECULAR METHODS ... 188
IN-HOUSE COMMUNICATION PROCESSES AND COMMUNICATION
BARRIERS IN HOSPITALS ... 192
THE EFFECT OF NICOTINE ON CORONAVIRUS DISEASE 19 INFECTION206
GENERAL CHARACTERISTICS OF MAMUT GEESE AND ASSESMENT OF
YIELD PERFORMANCE ... 214
MECHANISMS OF ANTIMICROBIAL RESISTANCE IN BACTERIA ... 221
GENOTYPING OF URINARY TRACT INFECTION FACTOR ESBL (+) E.COLI
STRAİNS WITH PFGE ... 232
THE USE OF SOCIAL MEDIA IN THE HEALTHCARE SECTOR ... 238
COVID 19 DISEASE ... 254
AN ORGANIZATIONAL HEALTH PROBLEM: NEPOTISM ... 260
WHAT SHOULD BE OUR AIM IN BREAST CANCER? ... 270
WELLBEING IN INDIVIDUALS SIXED YEARS AND OVER: AN APPLICATION
... 274
THE CHANGING PROCESS OF THE HEALTH CARE DURING AND AFTER PANDEMIC: ROLE OF FAMILY PHYSICIAN
Ayşegül KAPTANOĞLU Abstract
Health services started to go digital. Intelligent technologies and machine learning are currently the assistant of physicians and nurses in healthcare. But in the near future, can unmanned air ambulances and health personnel with machine learning capabioxsility take our place?
Covid 19 pandemic will shift rapidly towards robotics in the next few years?
In which business areas the health personnel will develop in this situation. It is not difficult to predict the future anymore. Telehealth is used extensively. "Robot doctor" application first comes into play in hospitals. The future has come. It is time to survive the pandemic using these processes.
Technology can’t replace life time experience. Seeing a sick person directly, or at least via video conferencing, can be greatly important than having his or her biochemistry but still wearable technology and technological innovation in healthcare will have crucial function in the everyday life.
Key Words: Health Care, Pandemic, Change, Fildes' art, Technology Introduction
The medical profession is a very old and seriously multiple organization. Sir Luke Fildes' painting The Doctor is shown in figure 1. This painting is the long suffering image of the Victorian times (20 June 1837 until her death on 22 January 1901) family physician from 1887. It was called family physician in The United State of America, general practitioner in United Kingdom at this time. This painting is frequently used to portray the qualities of a good doctor of 19th century.
Figure 1. The doctor 1887. Sir Samuel Luke Fildes, (1843 - 1927) was an English painter and illustrator born at Liverpool and trained in the South Kensington and Royal Academy schools.
This image of the ideal, devoted physician has appeared in many and different milieu in 20th century. It could be found in almost any status in our modern culture when thinking the qualities or lack of the medical profession (Moore, 2008: 210).
This study shows at the status of Fildes' art and asks if it is an precise proposal of evolutionary actual world. This show to a importance of the status and symbol of a physician in modern civilization and what we may study about this from a labor of Fildes' drawing (Friedlaender and Friedlaender, 2015: 3355).
Over the years, the physician has found its way into new look as banner, advertisement and has come into view on postage stamps of the countries.
President Truman suggest a configuration of nationalized medical care in 1949 turn around by using physician in brochures and posters but physician did not accept all them by saying along with the slogan, “Keep Politics Out of this Picture.” (Verghese, 2008: 117).
Technology in health care became with excellence of the job. But if our intent is the whole patient, if we still believe the practice of medicine has some bond with the feeling Fildes’ painting bring to life of us as observers, then perhaps it is excellence of the life that we are after, or better still, perfection of the life and of the work, conducting both recovering and treating to the patient.
The image of the ideal in 21st century.
Nowadays, human being will have access to their care plan and transmissions from their healthcare professionals via their country health App, which will enable people to manage their own health needs or direct them to the suitable service. If needed, they will relate to their local services to get an assignment with an ımmediate operation center or be ordered medicine to be collected from their nearest drugstore.
Two years later, the whole country will be able to access their maternity records digitally. Additionally, a digital version of the ‘red book’ will help parents record and use information about their child, including immunization records and growth. This will help children start life with a digital Personal Health Record (PHR) that they can build on throughout their lives (Ventola, 2014: 356).
The technology will enhance specialist medical care
By 2021, technology will give physicians easy access to consultation pattern and ‘one click away’ specialist recommendation and guidance for GPs, which will stop many patients from calling for referral for an date. To examining problems in order to decide which ones are the most serious and must be dealt with first: some physician referrals will let some patients to have entirely virtual evaluation.
In 2024-2025, diagnostic imaging networks will enable the rapid transfer of clinical images from care settings close to the patient to the relevant specialist clinician. This will help develop timely image presenting, as well as the development of great clinical data banks to fuel research and change. (Thimbleby, 2013: e28).
Healthcare and nutrition plans will be personalized for the individual
By the end of 2024, data will be collected by your smart health monitoring apparatus either wearable or applicable to the body, and by analyzing your bowel bacteria. Future dieticians will be able to fit a diet plan that suits the unique DNA and metabolism. We will also one day make this method to a genome-customized physical activity procedure (Lifescience Industry News, 2020).
Blood samples will be taken at birth and analyzed to identify the health issues your DNA makes you make susceptible to. A personalized ‘healthcare roadmap’ will be done detailing the custom vaccines, gene therapies
and surgeries you will need over the next couple of decades to avoid critical health problems as shown in figure 2 (Appelboom et al., 2014: 28).
Figure 2. The future of healthcare https://www.lifescienceindustrynews.com/future-watch/the-digital-future-of-healthcare-id-medical/
Ten years later, this information will be gathered using inborn tools, that will be used to capture data that allow clinicians and reduces the administrative burden. Clinical, genomic and other data will be linked, to support the development of new treatments. Data will be made ensure through the practice of security, monitoring systems and staff education (Lifescience Industry News, 2020).
The advent of smart technologies such as smartphones, fit bits, smart watches, and heart rate monitors has created enormous changes in healthcare.
Wearable technologies that can monitor various biological factors including hand, neck as necklaces, pocket at any time of the day, are now indispensable parts of our lives as shown in figure 3. a piece of technology that can monitor several health data.
Figure 3. Such data and monitoring can be instantly tracked by healthcare physicians and healthcare professionals to anyone using this technology.
Portable technologies can take saliva, urine, respiratory, epidemic systems, skin samples and transfer information to hospitals and family physicians.
However, wearable healthcare equipment is not easy to develop and commercialize. Because the construction method of ordinary semiconductor equipment and its adaptation to the body is not easy.
Regardless, scientific advances, chemical analysis techniques, equipment design and advances in manifacturing production methods have establish the corporation for a completely diverse tailored technology that has hang over to the perpetual development of wearable systems over the years. Some important device is shown figure 4 (Lou et al., 2020: 100523).
Figure 4. Medical wearable technologies will greatly reduce the lines below by minimizing human life.
Another aspect of preventive medicine is to reduce the number of diseases that can occur instantly. If physicians can address a distress before it turns into illness and an emergency room visit or emergency surgery, then they will save valuable resources over time. It will also improve the quality of life for patients over time: if a person is kept alive without being sick, or the faster the patient is diagnosed and treated, the better it will be in the long term.
It is known that anxiety and stress have disease-causing effects on the human body. Therefore, if physicians can benefit from wearable technologies, the dependence of such service providers on pharmaceutical solutions for various physiological conditions can reduce the following diseases shown in figure 5.
Figure 5. If physicians can take benefit of wearable technology, it can decrease the number that should depend on pharmaceutical solutions for various functional terms such as the following.
Case Management about the telehealth care
Dr. Anwar was a general practitioner with a private practice in Arlington Heightsi Cook County, Chicago, Illınois.
His surgery was a small rural community about two hours by train to Chicago. There were no other colleagues around. Dr. Anwar was able to give health care for every patient who need health care. The citizen around mostly need for chronic and specialized health care.
Dr. Anwar always referred his patients only to one specific hospital due to his high volume of the prestige that is provided by the referral hospital.
Shortly after the last winter, Dr. Anwar began to notice a decline in the amount of patient with chronic conditions or needing physician help to specialized care referrals.
One day while he was visiting an old friend, he suddenly noticed that his patients are having access to specialist via telehealth of the nearby hospital.
A healthcare professional must understand that digital healthcare is the current world reality that no one can ignore. Digitalization can help make health systems susceptible and manageable over the next couple of years declared world health organization (WHO, 2019).
Who will win robots? Or is it Humans?
The vice president of the Adv Illinois Medical Center noticed that prostate surgery operation has declined over the last six months. President began to investigate what happened.
Head of hospital public relation department politely find out that most of the patient were going to the hospital where the prostate surgeries were performed by robotic method.
There is a one hospital 10 kilometers away. Urologic surgeon of this hospital was performing with robotic surgery in this hospital.
Patient paying great importance to the removal of cancerous tissue by robotic prostate cancer surgery, so that nearby structures are not damaged and no cancerous tissue is left behind.
The most important reason for the patients to choose the hospital in question was the protection of the nerves that ensure the continuation of sexual functions.
At the end vice president decided to buy the necessary devices to perform surgery with a surgical robot and closed method.
Conclusion
In addition to smart wearable devices, smart robotic and autonomous systems will always support patients, physicians, nurses and medical technicians both in and after the pandemic.
Nowadays, remotely controlled mobile medical robotic platforms can triage patients from a safe distance. In addition, they can significantly reduce the risk of disease transmission to healthcare workers on the front line. When this epidemic is over, machine intelligence, wearable technologies and paradigm changes will be permanent in the daily practice of health. Physicians now advocate a revolution in therapy by allowing patients to track themselves more accurately.
The fight against the pandemic cannot be achieved without the support of science and technology”. Given the exponential rate of development in technology, every human are bound to see more practical examples of technology that will help people to fight this Covid 19 global crisis.
Preparedness for an unknown future and crises during the pandemic is not easy. This kind of work is always expensive and difficult. It requires a great deal of effort for problems that may or may not happen within the somebody’ lifetimes. People always think that crises don’t occur, and progress will follow progress during their life. But history of the world shows us otherwise.
After all, money is needed for all health technologies. Issues such as cost, patient compliance, and data accuracy associated with an unproven approach are factors to consider.
References
APPELBOOM, G., CAMACHO, E., ABRAHAM, EM., et al. (2014), Smart Wearable Body Sensors for Patient Self-Assessment and Monitoring, Archives of Public Health, 72(1), 28.
FRIEDLAENDER, KL., FRIEDLAENDER EG. (2015), Art in Science: The Doctor by Luke Fildes: Putting the Patient First, Clinical Orthopaedics and Related Research, 473(11), 3355-3359.
LIFESCIENCE INDUSTRY NEWS. (2020), The Digital Future of Healthcare – ID Medical, Retrieved on November 12, 2020 from
https://www.lifescienceindustrynews.com/future-watch/the-digital-future-of-healthcare-id-medical/.
LOU, Z., WANG, L., JIANG, K., et al. (2020), Reviews of Wearable Healthcare Systems: Materials, Devices and System Integration, Materials Science and Engineering: R, 140, 100523.
MOORE, J. (2008), What Sir Luke Fildes' 1887 Painting The Doctor Can Teach Us About the Practice of Medicine Today, British Journal of General Practice, 58(548), 210-213.
THIMBLEBY, H. (2013), Technology and the Future of Healthcare, Journal of Public Health Research, 2(3), e28.
VENTOLA, LC. (2014), Mobile Devices and Apps for Health Care Professionals: Uses and Benefits, Pharmacy
and Therapeutics, 39(5), 356-364.
VERGHESE, A. (2008), The Gordon Wilson Lecture “The Doctor in Our Own Time”: Fildes’ Famous Painting and Perceptions of Physician Attentiveness, Transactions of The American Clinical and Climatological
Association, 119, 117-126.
WORLD HEALTH ORGANIZATION EUROPE. (2019), What You Need to Know About Digital Health
Systems, Retrieved on November 12, 2020 from
NOTIFIABLE PARASITIC DISEASES IN TURKEY Banu Çiçek YÜCESAN
Today parasitic diseases which is a major health problem in subtropical countries such as Turkey to continue to threat to public health. With the globalizing world, there is a rapid spread to different countries in parasitic diseases, as in many diseases. Therefore, some parasitic disease which has seen tropical and subtropical countries has been seen in Turkey. Notifiable diseases must be notified to the state authority when they detected. Thus, it enables state mechanisms to monitor the disease and provides early warning in possible epidemics. Notification of infectious diseases to legal authorities is important in planning prevention and control programs, ensuring appropriate medical treatment and detecting outbreaks (Roush, Birkhead, Koo, Cobb, & Fleming, 1999:164).
The notification of infectious diseases is regulated by the "Public Health Law" No. 1593 of 1930. While notification of 39 diseases was mandatory in 2003, a new list of 51 diseases in four different reporting form was prepared based on the World Health Organization(WHO) and Disease Control and Prevention Center (CDC) publications in 2004 in Tukey. "Infectious Disease Notification System Directive" entered into force on 2004 in Turkey. This law has been rearranged as of January 1, 2005 and started to be implemented (Official newspaper, 2004). Since 2005, from the health institutions determined by the Ministry of Health, the notifiable diseases are made with different notification slips as A, B, C, D groups. In the current notification system, case definitions and diagnostic criteria included in the "Regulation on the Amendment of the Communicable Diseases Surveillance and Control Principles Regulation" updated by the Ministry of Health on May 4, 2019 are used. Standards should be established for the diagnosis and reporting of diseases that cause epidemics. In this way, infectious diseases can be fought. Notifiable diseases are examined in four categories in Turkey.
First group, Group A (Infectious agents that need to be reported from all institutions and organizations are in this group.)
Second group, Group B (Those are requiring international notification), Third group, Group C (Those are requiring sentinel notification),
The fourth group, Group D (Those are notified from the laboratory infectious agents)
There are 10 parasitic diseases among the notifiable diseases. Malaria and Cutaneous Leishmaniasis are diseases in Group A, Echinococcosis, Visceral Leishmaniasis (Kalaazar), Schistosomiasis and Toxoplasmosis are diseases in Group C, Cryptosporidiosis, Giardiosis, Amoebiasis and Trichinosis are diseases in Group D. Malaria, Leishmaniasis (Visceral and Cutaneous), Toxoplasmosis, Cryptosporidiosis, Giardiosis and Amoebiasis are protozoon infections. Schistosomiasis is a trematode infections. Echinococcosis is a cestode infections. Trichinosis is a nematode infections. All of these diseases are also zoonotic parasitic diseases. Therefore, it should be taken into account in a single health context (Dhaliwal & Juyal, 2013; Ramasamy, 2014:123)
1. GROUP A 1.1. MALARIA
Malaria Sıtma, Plasmodium vivax, Plasmodium malaria, Plasmodium ovale, Plasmodium falciparum, Plasmodium knowlesi Bite of Anopheles
mosquitoes Human infectious reservoir 1.1.1 Epidemiology:
The most common parasitic infection in the world is malaria. World Health Organization (WHO) reported in the World Malaria Report published in 2019 that there were 228 million cases in 2018. Africa cases accounted for 94% of all malaria deaths, with an estimated 405,000 deaths from malaria in 2018. Most of those who die from malaria are children under 5 years old (Akbaş, Abacıoğlu, & Ötgün, 2015; World Health Organization [WHO ], 2020a). Malaria is a major public health problem in Turkey and has been serious fighted for the eradication this infection. Today, with effective control program in Turkey it has decreased the number of domestic cases.
Plasmodium vivax is the most malaria species in our country and P. falciparum is frequently encountered from
abroad. The most common region are Cukurova, Southeast Anatolia Region and south of Eastern Anatolia Region in Turkey (Özbilgin, Topluoğlu,Es, Islek, Mollahaliloglu & Erkoç, 2011:15).
1.1.2 Clinic:
Malaria is transmitted through the bites of female Anopheles mosquitoes carrying of the Plasmodium. The incubation period of malaria, which is an acute febrile illness, is two weeks. This period is longer in P. malaria and shorter in P. falciparum. While it initially gives flu-like symptoms, it is later seen with chills, tremor, fever and sweating, which are called malaria attacks. Malarial attacks occur every 36-48-72 hours or irregularly, depending on the species. If P. falciparum is not treated, it can have fatal consequences. Then, anemia and splenomegaly are added to the findings and serious complications may develop depending on the type of parasite (Garcia, 2010: 93)
1.1.3 Diagnosis:
1.1.3.1. Microscopic methods: Thick or thin blood smear (It must be stained with a Romanovsky stain (most often Giemsa)). The preparation should be examined microscopically with 100x immersion oil.
1.1.3.2. Antijen detection: Rapid Malaria Diagnostic Tests are immunochromatografic tests.
1.1.3.3. Serology: Enzyme-linked immunosorbent assay (ELISA) and indirect immunofluorescence (IFA) tests. 1.1.3.4. Molecular diagnosis: PCR
1.1.3.5. Drug Resistance Tests: Invitro tests and PCR (Zimmerman & Howes, 2015:446). 1.2. CUTANEOUS LEISHMANIASIS
Disease Synonyms Agent Vector Reservoir
Cutaneous Leishmaniasis Delhi sore, Oriental sore, Baghdad ulcer, Uta, Buba
Old world: Leishmania tropica complex (Leishmania tropica, Leishmania major,
Leishmania aethiopica)
New world: Leishmania mexicana complex,
Leishmania lainsoni, Leishmania naiffi, Leishmania lindenbergi
Some strains of Leishmania infantum
Bite of Sand flies (Phlebotomus, Lutzomyia) Dogs, rodents, edentates, marsupials, carnivores 1.2.1. Epidemiology:
World Health Organization reports that 83 countries are endemic to Cutaneous Leishmaniasis (CL) and 1 million new cases are reported annually in 2018. More than 1 billion people in the world live in endemic areas (WHO,
2020b). Sanliurfa, Osmaniye, Adana, Hatay, Aydin, Izmir, Istanbul, Mersin and Kahramanmaras provinces of Turkey are the most common (Gürel, Yeşilova, Ölgen, & Özbel, 2012:121)
1.2.2. Clinic:
Leishmaniasis is a disease transmitted by female sandflies (Phlebotomus) infected with parasites of the genus
Leishmania to humans while sucking blood. It can be observed asymptomatically in some people. Oriental sore
begins as an erythematous papule. It first becomes nodule and then ulcerated. It is a generally painless lesion with its crust tightly adhered to the base, with a crater in the center and induration. If left untreated, it will heal with an irregular scar (Reithinger, Dujardin, Louzir, Pirmez, Alexander & Brooker, 2007:581).
1.2.3. Diagnosis:
1.2.3.1. Microscopic methods: In smear preparations, Leishmania amastigotes can be stained with Giemsa and detected with immersion oil at 100x magnification under microscope.
1.2.3.2. Culture: The material planted in NNN medium is checked for growth for 4 weeks at 2-3 days intervals. 1.2.3.3. Molecular diagnosis: PCR
1.2.3.4. Montenegro test: .It is the skin test for Leishmania (Akbaş et al., 2015; Centers for Disease Control and Prevention [CDC], 2020a)
2. GROUP C
2.1. ECHINOCOCCOSIS
Disease Synonyms Agent İntermadiate
host
Definitive Host
Echinococcosis
Hydatidosis, dwarf dog tapeworm, hydatid disease, cystic Echinococcosis, alveolar Echinococcosis, neotropical Echinococcosis Echinococcus granulosus, Echinococcus multilocularis, Echinococcus oligarthrus, Echinococcus vogeli They are a variety of mammals, including humans Carnivores such as wolves and jackals, especially dogs. 2.1.1. Epidemiology:
Echinococcosis which has two most important form is zoonotic disease. More than 1 million people around the world are thought to suffer from this infection. Echinococcus granulosus, which causes cystic echinococcosis, is the most common among other Echinococcus species both in the world and in our country. This species is found in almost every region of the world. It is very common in Russia, China and South America in the world. It is more common especially in developing countries where animal husbandry is common. E. multilocularis, which
occurs in the northern hemisphere, causes alveolar echinococcosis and is becoming more common. E. vogeli and
E. oligarthrus have a limited distribution in Central and South America. They are called Neotropical
echinococcosis. While E. vogeli causes a polycystic form, E. oligarthrus causes an extremely rare monistic form. Cystic echinococcosis is seen in all regions of our country, mostly in the Eastern Anatolia region (Bulaşıcı Hastalıkların Saha Rehberi [BHSR], 2020; CDC, 2020b; WHO, 2020c).
2.1.2. Clinic:
Echinococcosis is usually silent in its initial period. Fluid-filled cysts often develop in the liver, less frequently in the lungs, and more rarely in all other organs (brain, kidney, spleen, pelvic organs, bone, eye, etc.). This disease gives symptoms according to the organs in which it is placed and pressure on neighboring organs. Right upper quadrant pain, hepatomegaly, dyspepsia, jaundice as a result of mechanical pressure on the biliary tract; Attacks
of cholangitis and pancreatitis as a result of opening to the biliary tract. If the patient has a lung infection, there may be weight loss, fever, cough, chest pain, hemoptysis (Eckert & Deplazes, 2004:107).
2.1.3. Diagnosis:
2.1.3.1. Imaging techniques: CT scans, ultrasonography, and MRIs, are used to detect cysts.
2.1.3.2. Microscopic methods: Observation of protoscolexes in the cyst fluid aspirated for diagnostic purposes is a microscopic evaluation method.
2.1.3.3. Serology: Serological tests used for screening purposes such as IHA (Indirect Hemagglutination Test), ELISA, and IFA are very useful in diagnosis. It is more useful than invasive methods. Care should be taken in terms of false positives or negativities. After the positivity in screening tests, the WB test should be used as a confirmatory. Serological tests are more reliable in the diagnosis of alveolar echinococcosis than cystic echinococcosis.
2.1.3.4. Molecular diagnosis: PCR. It is the definitive method of diagnosis (Thomas, Zwingelberg, Angele, Guba & Werner, 2017:32)
2.2. VISCERAL LEISHMANIASIS (KALA-AZAR)
Disease Synonyms Agent Transmission Reservoir
Visseral Leishmaniasis
Kala-azar, Black fever, dumdum fever, postkala-azar dermal Leishmaniasis.
Leishmania infantum, L. donovani, L.chagasi
Bite of Sand flies (Phlebotomu, Lutzomyia spp.) Dogs, rodents, edentates, marsupials, carnivores 2.2.1. Epidemiology:
Visceral leishmaniasis is essentially a zoonosis. The disease develops with the bite of infected female
Phlebotomus sandflies. Sandflies become infected when they suck blood from an infected human or animal. The
main reservoirs of the agent are domestic and wild canids (dog, fox, jackal etc.). Although the number of new cases was 400,000 or more annually, it has now fallen below 100,000. Visceral leishmaniasis is caused by
Leishmania infantum and L. donovani in old World. The most important reason is L. infantum in Turkey. In our
country, it is mostly seen sporadically in all regions including the Aegean, Mediterranean and Central Anatolia (CDC, 2020c; Akbaş et al., 2015).
2.2.2. Clinic:
Visceral leishmaniasis is a life-threatening infection which is affecting the spleen, liver, and bone marrow. This disease develops after a sand fly bite and its incubation period is between 3 weeks and 2 years. Fever, weight loss, hepatosplenomegaly, anemia, leukopenia, thrombocytopenia and hypergammaglobulinemia are observed in these patients. If the disease is not treated, it can result in death (Lagardere, Chevallier, & Cheriet, 1992:159)
2.2.3. Diagnosis:
2.2.3.1. Microscopic methods: A definitive diagnosis is made by microscopic observation of Leismania spp. amastigote forms in tissue biopsies, aspirates or 'buffy-coat' smears.
2.2.3.2. Culture: It is inoculated on NNN medium brought to room temperature. If there are agents in the transplanted samples, promastigotes are usually observed in 5-7 days.
2.2.3.3. Rapid Diagnostic Tests: A positive result with rapid tests supports the possibility of Kala-azar. 2.2.3.4. Serology: IFAT, ELISA.
2.3. SCHISTOSOMIASIS
Disease Synonyms Agent Transmission Reservoir
Schistosomiasis Bilharziasis, snail fever
Schistosoma haematobium (urinary
schistosomiasis),
S. mansoni, S. japonicum, S. mekongi, S. intercalatum and S. guineensis
(gastrointestinal and hepatosplenic schistosomiasis)
Snails act as the intermediate host for the parasite
Parasite has the ability to infect more than 40 wild and domestic animals, including humans 2.3.1. Epidemiology:
Parasite is common in tropical and subtropical areas and places where socioeconomic status is low. Around 240 million people worldwide suffer from Schistosomiasis (WHO, 2020d). In Turkey, the GAP (Southeastern Anatolia Project) become important with this parasite, it is endemic in regions close to our borders. The increase of Bulinus, which are intermediate hosts of this parasite, causes it to occur in this region (Akbaş et al., 2015).
2.3.2. Clinic:
The disease has two forms: the intestinal form and the urinary form. People become infected when they come into contact with fresh water infected with cercaria forms of these blood parasites. Abdominal pain, diarrhea, mucus and blood in the stool, nausea, weight loss are observed in the intestinal schistosomiasis. Portal hypertension and splenogema may occur in progressive cases. In urogenital schistosomiasis, dysuria, hematuria, bladder symptoms in chronic cases, infertility, etc. symptoms happen (Gryseels, 2012:383).
2.3.3. Diagnosis:
2.3.3.1. Microscopic methods: Searching for parasites with urine concentration method: Biopsy: The diagnosis is made when Schistosoma haematobium eggs are seen as a result of the pathological examination of the bladder tissue. Egg vitality test: It is shown that miracidiums hatch from eggs in urine or suspicious tissues.
2.3.3.2. Serology: IHA, IFAT, ELISA, WB. 2.3.3.3. Molecular diagnosis: PCR (WHO, 2020e)
2.4. TOXOPLASMOSIS
Disease Synonyms Agent Transmission Reservoir
Toxoplasmosis Congenital toxoplasmosis. Toxoplasma gondii.
Eating raw or undercooked contaminated mea, transplasental transmission, organ transplants. Cats are definitive host and shed oocysts with their faeces
Many intermediate hosts, e.g. sheep, goat, pig, cattle, etc., including man.
2.4.1. Epidemiology:
Toxoplasma gondii oocysts are more common in these areas as they can live in hot, humid climates and low
altitude regions of the world. It is one of the most common infections in the world. The world population is thought to be infected on average between 30% and 60%. High prevalences have been found in Latin America and tropical African countries. In studies of seropositivity rate in Turkey, it is seen to be between 57% and 27% (Akbaş et al., 2015).
2.4.2. Clinic:
Usually asymptomatic in healthy people. It is a zoonosis that can involve all vital organs in the human body and can be found in all liquid extracts such as blood, cerebrospinal fluid (CSF), semen, tears, saliva and urine
especially in the acute period, and causes permanent fetal destruction and miscarriage with transplacental transmission. It is severe in immunocompromised patients and results in death if not taken under control (Halonen & Weiss, 2013).
2.4.3. Diagnosis:
2.4.3.1. Microscopic methods: It can be detected by staining body fluids such as CSF, vitreous humor, pericardium and amniotic fluid with Giemsa.
2.4.3.2. Serology: Sabin Feldman Dye test, IHA, IFAT, ELISA, WB, Capture ELISA, ISAGA, IgG avidity 2.4.3.3. Culture: Isolation of T. gondii from blood, body fluids or tissues can be accomplished by cell culture or inoculation into mice.
2.4.3.4. Molecular diagnosis: PCR (Gangneux & Darde, 2012). 3. GROUP D
3.1. CRYPTOSPORIDIOSIS
Disease Synonyms Agent Transmission Reservoir
Cryptosporidiosis Crypto
Cryptosporidium parvum, C. homins, C. meleagridis, C.felis, C.canis, C.ubiquitum, C. cuniculus, C. viatorum, C.muris. Cryptosporidium spp.(26 species)
Occurs through the faecal oral route
Newborn calves, drinking water and recreational water are important for
contaminating humans. 3.1.1. Epidemiology:
Cryptosporidiosis is a protozoan infection that is common worldwide and is characterized by gastrointestinal diseases in many mammals. This disease is under investigation in one healthcare context and causes many waterborn outbreak. It is a disease that can lead to fatal consequences in many patients with suppressed immune systems such as AIDS. Cryptosporidiosis also plays an important role in childhood diarrhea too (Dillingham, Lima & Guerrant, 2002).
3.1.2. Clinic:
Cryptosporidiosis is characterized by diarrhea is characterized by watery stools, abdominal pain, fever, nausea-vomiting and weight loss. Symptoms start between 2 and 10 days. The infection lasts up to 2 weeks and in patients with suppressed immune system, the respiratory system is affected as well as the digestive system. Extraintestinal cryptosporidiosis has been observed in the pulmonary, biliary tract and rarely in the pancreas (CDC, 2020d).
3.1.3. Diagnosis:
3.1.3.1. Microscopic methods: Smear preparations prepared from fresh or consolidated stool samples are stained with modified Kinyoun acid-fast technique, and parasites are searched microscopically. In addition, the sample precipitate obtained by precipitation method is dyed with Auramin-rhodamine fluorescent dye and examined under fluorescence microscope by dropping immersion oil. parasite oocysts appear as round-oval cells with orange-yellow fluorescence under ultraviolet light (CDC, 2020d).
3.1.3.2. Direct Fluorescent Antibody (DFA) Test: this test is considered the gold standard. It is based on the principle that FITC-labeled Cryptosporidium monoclonal antibodies bind to the surface of oocysts in the patient sample and make it visible.
3.1.3.3. Serology: ELISA 3.1.3.4. Rapid Diagnostic Tests:
3.1.3.5. Molecular diagnosis: PCR (Abd-Ella, 2014). 3.2. GIARDIOSIS
Disease Synonyms Agent Transmission Reservoir
Giardiosis Giardia enteritis
Giardia duodenalis (syn. G. lamblia, G. intestinalis)
Infection takes place through faecal oral route
The main reservoir for humans are people. Cattle populations and water sources are sources of contamination. 3.2.1. Epidemiology:
Giardiosis is the most common intestinal parasitosis of worldwide. This disease is more common in places where people live together and in poor hygienic conditions. This is a parasitosis that spreads from contaminated water sources and can cause mass outbreaks (WHO, 2020f).
3.2.2. Clinic:
The disease is transmitted by ingestion of mature quad-core cysts of the protozoan parasite. Giardiosis can be asymptomatic or cause acute or chronic infection. It develops 1-14 days after the fecooral intake of the agent and lasts 1-3 weeks. In acute cases, severe oily diarrhea with abundant foul odor is observed. It may cause malabsorption in chronic cases. It can cause stopping of weight gain, malnutrition and growth retardation in children (Olszok & Kucharz 1996:576)
3.2.3. Diagnosis:
3.2.3.1. Microscopic methods: Prepares native-lugol preparation from fresh stool or sample with concentration method. Giardia trophozoites can be seen here.
3.2.3.2. Direct Fluorescent Antibody (DFA) Test: It can be made with the same kit as Cryptosporidium. 3.2.3.3. Rapid Diagnostic Tests:
3.2.3.4. Molecular diagnosis: PCR (Leung AKC, Leung AAM, Wong, Sergi & Kam, 2019:134) 3.3. AMOEBIASIS
Disease Synonyms Agent Transmission Reservoir
Amoebiasis Amoebiasis, amoebic dysentery, entamoebiasis. Entamoeba histolytica, E. dispar, E. Polecki
Occurs through the faecal oral route. Flies can carry cysts as vectors.
Human is main reservoir 3.3.1. Epidemiology:
Amoebiasis, occurs worldwide. The disease is widespread in tropical areas and inadequate health services areas. It ranks third after malaria and schistosomiasis among parasitic diseases. Approximately 50 million individuals are affected each year in the world; 100,000 deaths are seen every year due to complications from invasive amoebiasis (Akbaş et al., 2015).
3.3.2. Clinic:
Intestinal amoebiasis is 90% asymptomatic and these are associated with Entamoeba dispar. E. histolytica is the causative agent of amoebic dysentery and can cause dysentery, colitis and rarely ameboma. Extraintestinal forms may develop with the settlement of trophozoites in the liver, lungs, brain and pericardium. Depending on organ involvement, hepatomegaly, pain, fever, weakness, weight loss, cough and sweating can also be seen. Abscess can spread into peritoneum and skin (WHO, 2020g).
3.3.3.1. Microscopic methods: Microscopic examination is performed with nativ-lugol and trichrome staining method.
3.3.3.2. Serology: ELISA, IHA,
3.3.3.3. Searching for parasite antigens: E. histolytica Ag ELISA or E. histolytica/E.dispar Ag ELISA. 3.3.3.4. Culture: Robinson medium is used for culture.
3.3.3.5. Molecular diagnosis: PCR (Saidin, Othman & Noordin, 2019:15) 3.4. TRICHINOSIS
Disease Synonyms Agent Transmission Reservoir
Trichinosis
Trichinellosis, Trichiniasis, Trichinelliasis
Trichinella spiralis, T. nativa, T. britovi, T. murrelli, T. nelsoni, T. pseudospiralis, T. papuae, T. zimbabwensis Trichinosis is transmitted to humans by eating raw or undercooked wild game meat or pork
Carnivorous animals such as bear or cougar, or omnivorous animals such as domestic pigs or wild boar.
3.4.1. Epidemiology:
Trichinosis is a zoonotic nematode disease which is occur 10.000 cases each year. This disease is common all over the world and the most common species is T. spiralis found in pigs. Other species are often isolated from wild animals. The number of trichinellosis cases reported in the United States is declining (CDC, 2020). While the cases of trichinellosis caused by eating pork are decreasing, eating undercooked wild game meat increases the risk of getting this disease. Turkey reported an outbreak in December 2003. T. britovi is a factor in this epidemic (Akbaş et al., 2015).
3.4.2. Clinic:
Symptoms of trichinellosis occur 1-2 days after eating raw or undercooked animal meat. Gastrointestinal symptoms (Nausea, diarrhea, vomiting, abdominal pain) occur first. Later findings can be listed as hemorrhages around the cornea, conjunctiva, retina, skin rash, muscle aches, respiratory complaints, chest pain, nervous system symptoms such as headaches, dizziness, tinnitus, extreme weakness, and myocardial failure due to brain involvement of larvae (Beshbishi, Ahmed, Mostafa & El-Ganainy, 2012: 1).
3.4.3. Diagnosis:
3.4.3.1. Microscopic methods: Usually not found in microscopic examination of stool. But sometimes adult forms or larvae can be seen in the faeces within 5-15 days.
3.4.3.2. Serology: ELISA, IHA, IFA, WB
3.4.3.3. Seeing larvae in muscle biopsy: It can be seen in histopathological examinations. 3.4.3.4. Molecular diagnosis: PCR (Gottstein, Pozio, & Nöckler, 2009)
A fact that is not sufficient notification of infectious diseases in Turkey. The same applies to the notifiable condition parasitic diseases. Reporting of all notifiable diseases can lead to serious measures for public health. With these notifications, precautions can be taken against infection threats to be encountered throughout the country and rapid response can be given. In order to establish national and international surveillance networks and to obtain official data on diseases, notifiable diseases should be followed carefully. There are problems with parasites in Turkey as in other diseases in disease notification. It is necessary to be sensitive about the reporting
of parasitic diseases, which are systematically considered as a single health concept and are very important for public health.
References:
Abd-Ella, O.H. (2014). Diagnosis and treatment of cryptosporidiosis: an update review. J Egypt Soc Parasitol.,
44(2):455-466.
Akbaş, E., Abacioğlu, H., & Ötgün, S. N. (2015). National Microbiology Standards Infectious Diseases
Laboratory Diagnosis Guide (UMS) Parasitology / Microbiological Identification Volume 3. Ankara,
Türkiye: Public Health Agency of Turkey Ministry of Health Publication.
Beshbishi, S.N.E., Ahmed, N.N., Mostafa, S.H. & El-Ganainy, G.A. (2012). Parasitic İnfections an myositis.
Parasitol Res.,110(1):1-18. doi: 10.1007/s00436-011-2609-8. Epub 2011 Sep 1.
Bulaşıcı Hastalıkların Saha Rehberi (BHSR) (2020) Kistik Ekinokokkoz. Retireved from file:///C:/Users/FUJITSU/Downloads/Kistik-ekinokokkoz_Saha_Rehberi%20(1).pdf
Centers for Disease Control and Prevention (CDC) (2020a). Leishmaniasis. Retireved from https://www.cdc.gov/dpdx/leishmaniasis/index.html
Centers for Disease Control and Prevention (CDC). (2020b). Echinococcosis. Retireved from
https://www.cdc.gov/dpdx/echinococcosis/index.html.
Centers for Disease Control and Prevention (CDC) (2020c). Leishmaniasis. Retireved from https://www.cdc.gov/parasites/leishmaniasis/gen_info/faqs.html
Centers for Disease Control and Prevention (CDC) (2020d). Cryptosporidiosis. Retireved from https://www.cdc.gov/dpdx/cryptosporidiosis/index.html
Centers for Disease Control and Prevention (CDC) (2020e). Trichinellosis. Retireved from https://www.cdc.gov/parasites/trichinellosis/epi.html
Dhaliwal, B.B.S., & Juval, P.D. (2013). Parasitic Zoonoses. New Delhi, İndia: Springer.
Dillingham, R.A., Lima,A.A. & Guerrant, R.L. (2002). Cryptosporidosis: epidemiology and impact. Microbes
Infect. 2002 Aug;4(10):1059-66. doi: 10.1016/s1286-4579(02)01630-1.
Eckert. J., & Deplazes. (2004). Biological, epidemiological, and clinical aspects of echinococcosis, a zoonosis of increasing concern. Clin Microbiol Rev, 17(1):107-135. doi: 10.1128/cmr.17.1.107-135.2004.
Gangneux, F.R., & Darde, M.L. (2012). Epidemiology of and diagnostic strategies for toxoplasmosis. Clin
Microbiol Rev., 25(2):264-296. doi: 10.1128/CMR.05013-11.
Garcia, L.S. (2010). Malaria. Clin Lab Med. 30(1):93-129. doi: 10.1016/j.cll.2009.10.001.
Gryseels, B. (2012). Schistosomiasis. Infect Dis Clin North Am, 26(2):383-397. doi: 0.1016/j.idc.2012.03.004. Gottstein, B., Pozio, E., & Nöckler, K. (2009). Epidemiology, diagnosis, treatment, and control of trichinellosis.
Gürel, M. S., Yeşilova, Y., Ölgen, M. K., & Özbel, Y. (2012). Türkiye’de kutanöz leishmaniasisin durumu.
Turkiye Parazitol Derg, 36, 121-129.
Halonen, S.K., & Weiss, L.M. (2013). Toxoplasmosis. Handb Clin Neurol., 114:125-145. doi: 10.1016/B978-0-444-53490-3.00008-X.
Lagardere, B., Chevallier, B., & Cheriet, R. (1992) Kala-azar. Ann Pediatr, 39(3):159-164.
Leung, A.K.C., Leung, A.A.M, Wong, A.H.C., Sergi, C.M., & Kam J.K.M. (2019). Giardiasis: An Overview.
Recent Pat Inflamm Allergy Drug Discov.,13(2):134-143. doi: 10.2174/1872213X13666190618124901.
Official newspaper (2004). Infectious Disease Notification System Directive. Retrieved from
https://www.mevzuat.gov.tr/mevzuat?MevzuatNo=8580&MevzuatTur=9&MevzuatTertip=5.
Olszok, I., & Kucharz, E.J. (1996) Giardiasis. Przegl Lek., 53(7):579-81.
Özbilgin, A., Topluoglu, S., Es, S., Islek, E., Mollahaliloglu, S., & Erkoc, Y. (2011). Malaria in Turkey: successful control and strategies for achieving elimination. Acta tropica, 120(1-2), 15-23.
Ramasamy, R. (2014). Zoonotic malaria–global overview and research and policy needs. Frontiers in public
health, 2, 123.
Reithinger, R., Dujardin, J.C., Louzir, H., Pirmez, C., Alexander, B., & Brooker, S. (2007). Cutaneous leishmaniasis. Lancet Infect Dis. 7(9):581-596. doi: 10.1016/S1473-3099(07)70209-8.
Roush, S., Birkhead, G., Koo, D., Cobb, A., & Fleming, D. (1999). Mandatory reporting of diseases and conditions by health care professionals and laboratories. Jama, 282(2), 164-170.
Saidin S., Othman, V., & Noordin, R. (2019). Update on laboraory diagnosis of amoebiasis. Eur J Clin
Microbiol Infect Dis., 38(1):15-38. doi: 10.1007/s10096-018-3379-3. Epub 2018 Sep 25.
Thomas, M.N., Zwingelberg, S., Angele, M., Guba, M., & Werner, J. (2017). Diagnosis and treatment of cystic
and alveolar echinococcosis. MMV fotschr Med. 159(14):38-42. doi: 10.1007/s15006-017-9948-z. Zimmerman P.A., & Howes, R.E. (2015). Malaria diagnosis for malaria elimination. Curr Opin
Infect.Dis.28(5):446-454. doi: 10.1097/QCO.0000000000000191.
World Healt Organizations (WHO) (2020a). Malaria. Retireved from
https://www.who.int/news-room/fact-sheets/detail/malaria.
World Healt Organizations (WHO) (2020b). Leishmaniasis. Retireved from
https://www.who.int/health-topics/leishmaniasis#tab=tab_1.
World Healt Organizations (WHO) (2020c). Echinococcosis. Retireved from
https://www.who.int/news-room/fact-sheets/detail/echinococcosis.
World Healt Organizations (WHO) (2020d). Schistosomiasis. Retireved from https://www.who.int/health-topics/schistosomiasis#tab=tab_1.
World Healt Organizations (WHO) (2020e). Schistosomiasis. Retireved from https://www.who.int/news-
World Healt Organizations (WHO) (2020f). Intestinal Protozoon and helmitic infections. Retireved from https://apps.who.int/iris/bitstream/handle/10665/41519/WHO_TRS_666.pdf?sequence=1&isAllowed=y World Healt Organizations (WHO) (2020g). Amoebiasis. Retireved from
THE EVALUATION OF ADOPTION AND SUCCESS OF HEALTHCARE INFORMATION SYSTEMS İbrahim TÜRKMEN İsmail Erkan ÇELİK Barış SARDOĞAN
Abstract
Within the scope of health transformation program in Turkey access to health services was facilitated and significant investments were made in health care technologies. It is not possible to record, classify, analyze and save billions of data on paper with the increase in the number of applications to the hospital and the widespread use of imaging services. Therefore, it has become necessary to transfer the records in health sector to electronic media. With the development of information technologies, health information systems have been developed to help make the records in health sector electronic. Health information systems are generally regarded as technical systems and evaluated by technical experts. Behavioural and organization dimensions of these systems can usually be ignored. Information systems are considered as social systems as well as technical systems. System-user harmony should have to be ensured to get benefits from information systems. In this context, the adoption and satisfaction of users and affordable demands of users for the system are considered as the most important factors for the success of the information systems. In this part, recommendations have been made by giving information about the "technology adoption model", "information systems success model" and "electronic medical record adoption model" developed for the evaluation of the adoption and success of health information systems.
Keywords: Electronic Health Records, Healthcare Information Systems, Technology Adoption Model, Information Systems Success Model, Electronic Medical Record Adoption Model.
Introduction
Developments in the economic, socio-cultural, political-legal and technological fields have been a trigger of many changes also in the field of health. These changes led countries to develop new policies regarding the delivery of health services. Developed countries initiated the health reform efforts in 1980’s. Health reform efforts in Turkey was put into practice in 2003 with "Health Transformation Program (HTP)". Within the scope of HTP, general health insurance practice covering all citizens was initiated and access to health services was facilitated. As a result of this practice, the number of applications to the hospital increased by 288% compared to 2002 and reached 813 million people in 2019 (Ministry of Health, 2020a). Increasing and aging population and prolongation of life expectancy also have an effect on the increase in the number of hospital applications. Turkey's population of 64.7 million in 2000 reached 83 million in 2019. Again, life expectancy from birth, which was 71.0 in 2000, increased to 78.3 in 2019 (TSİ, 2020a). The population rate of people at the age 65 and above who are considered to be elderly has increased by 21.9% in the last five years to 9.1% in 2019 (TSİ, 2020b). Factors such as population growth, urbanization, changes in lifestyle and dietary habits, prolongation of life span, full coverage of compulsory health insurance and the widespread use of private insurance increased the need for health services and also facilitated the access to health services.
From the process started with the HTP until today, significant investments have been made in the field of medical technology in Turkey. While the number of MR used in public hospitals was 18 in 2002, it increased to 338 in 2019, while the number of CT was 121, it increased to 550 and while the number of USGs was 495, it
increased to 2.580. Turkey is in the first rank among the 25 OECD countries when examined in terms of imaging numbers (Ministry of Health, 2020a). In the field of health hospital management systems based on information systems emerged in order to record information about personal and treatment processes of patients, as well as technologies used for diagnostic purposes. The increase in elderly population rate in Turkey as well as the increase in general population and expected life span boosts the demand for health sector and therefore leads to the development in health sector. As a result of rapidly increasing number of applications due to ease of access to health services billions of data are produced. It is not possible to save, classify, analyze, turn into information and make useful such large amount of data produced in the health sector on paper or CD media. It is also impossible for an important and large sector such as the health sector to be managed, to develop policies and to achieve success without relying on data. For those reasons, it has become necessary to use information and communication technologies in health sector. Since 2003, hospitals in Turkey have been providing information systems through outsourcing (Ak, 2009). The companies providing hospital information systems are accredited by the Ministry of Health and there are 57 accredited companies providing HIMS services as of 2020. HIMS are used in all hospitals providing health services in Turkey (Ministry of Health, 2020b).
Computer and internet-based information systems which have become mandatory to be used in the health sector as in all sectors today are generally considered as technical systems; however, behavioral and organizational dimensions of these systems can usually be ignored. Problems concerning the implementation of information systems are related to the interaction of human, organizational and technical factors. Therefore, information systems should be regarded as social systems, not just technical systems with behavioral consequences (Walsham et al. 1988). In this context, HIMS is defined as a socio-technical infrastructure of a hospital. Today health sector professionals have become both users and parts of the system. Ensuring HIMS productivity and user satisfaction also affects the quality of health services (Haux et al. 2004). For that reason, not to have information technologies, but to increase the benefits that users generate through information systems is important (Kanjo, 2017). The return of investments in technology in the health sector depends on the effective use of the implemented information systems and user satisfaction which is one of the important determinants of the success of these systems. The purpose of this study is to give information about the models developed in order to evaluate the adoption and success of HIMS. Firstly, information about health informatics will be given in the first part. In the second part, Technology Adoption Model, in the third part Information Systems Success Model and in the fourth part HIMSS EMRAM Model will be included. In the final part conclusion and recommendations will be included.
Health Information Systems
Health informatics is “a discipline related to the systematic processing of data, information and knowledge in medicine and healthcare services” (Hasman et al. 1996). Information systems are the systems which provide information and knowledge to relevant employees in appropriate time, place and form by allowing the transactions to be recorded, classified, saved and analyzed (Haux et al. 2004). Information systems are defined as the systems which collect, process, classsify, save and share the data, information and knowledge and complete each other in order to support decision-making, coordination and control of an organization (Laudon and Laudon 2014). Health information systems, information management and technologies are accepted as a strong tool
systematically used in the planning and delivery of high quality and low cost health services (Norris and Brittain 2000).
The use of information technologies in hospitals contributes to reducing errors in health care, providing quality and safe service to patients, increasing the productivity of staff and reducing costs (Bates et al. 2001). The purpose of health information systems is to contribute the delivery of high quality and efficient health services (Haux, 2006). Information systems used in hospitals provide an institutional framework containing different information about the medical, financial and administrative functions of a certain hospital. The first applications of these systems are limited to recording patient information and invoicing the provided health services. Today new modules have been added to information systems such as online appointment, patient follow-up, demand analysis and imaging results. Information systems provide convenience to patients and doctors especially in the delivery of preventive and curative health services (Demirel, 2017).
The following development stages are considered important for information systems used in the health sector (Haux 2006):
Transition to computer-based processing and storage because the increasing number of data in healthcare services makes papers dysfunctional,
Transition to national and international information systems from institution-centered information systems, Inclusion of healthcare consumers as the users of information system as well as healthcare professionals and managers,
The use of informations systems not only for patient care and administrative purposes but also for clinical and epidemiological research as well as healthcare services,
Transition to change management and strategic information management from problem-based managements through information systems,
Transition to images and the data at molecular level from numerical data in information systems,
Continuous increase today in new technologies that will begin to include computer usage platforms and cencor-based technologies for health monitoring.
Technology Adoption Model
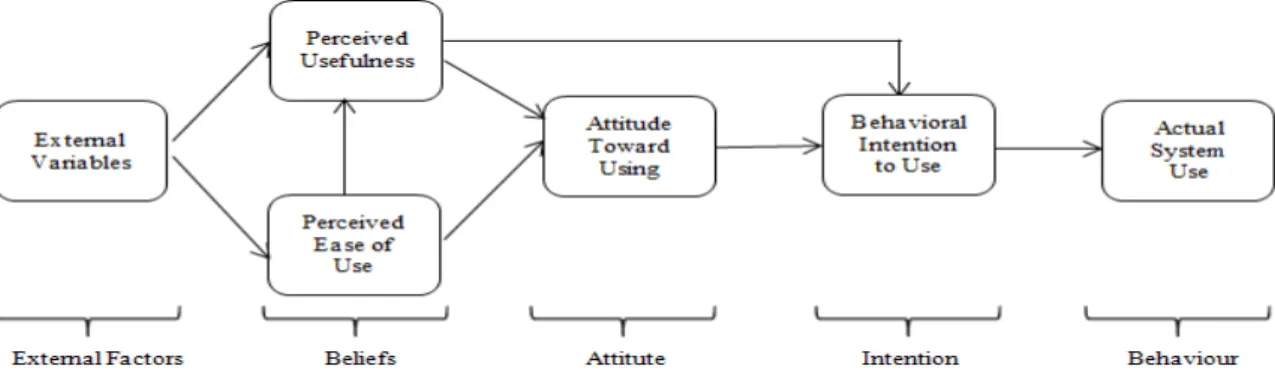
As well as owning, voluntary use and adoption by users are required so that information systems can produce benefits (Al-Emran, Mezhuyev and Kamaludin, 2018). One of the most important models developed for the use and adoption of information systems in businesses is Technology Adoption Model (TAM). TAM developed in phd thesis written by Davis (1986) was prepared based on the "Planned Behavior Theory" (Fishbein and Azjen, 1975) to model the adoption of information systems by users. TAM aims to explain the factors affecting the use and adoption of information technologies by end users. For that reason, the main purpose of TAM is to provide a reference to determine the effect of external factors on internal factors such as beliefs, attitudes and intentions. The first model developed was updated by Davis, Bagozzi and Warshaw (1989) and took its final form (Figure 1).
Figure 1. Technology Adoption Model (Davis, Bagozzi and Warshaw, 1989)
According to the model, different external variables affect the belief for information systems (Kalyoncuoğlu, 2018). Different external variables are included in the model according to the sector that information systems are used and their users. Different variables such as personal innovation, mobile skills, perceived entertainment (Wong et al., 2015), availability/ compatibility (Turan, 2008), convergence, image (Şıklar, Tunalı and Gülcan, 2015), financial risk, security risk (Doğan, Şen and Yılmaz, 2015), education system, software knowledge, hardware knowlegde, programming knowledge (Aras, Özdemir and Bayraktaroğlu, 2015) were included in relevant variables as external variables. TAM assumes that two specific beliefs as perceived usefulness and perceived ease of use are of primary importance for technology adoption behavior (Davis, Bagozzi and Warshaw, 1989). These two factors are the variables used for measuring the beliefs of users for information system (Koul and Eydgahi, 2017). The beliefs of end users for information system form their attitudes towards usage and the attitudes towards usage provide voluntary use of information systems by affecting behavioural intention to use (Davis, Bagozzi and Warshaw, 1989).
Information Systems Success Model
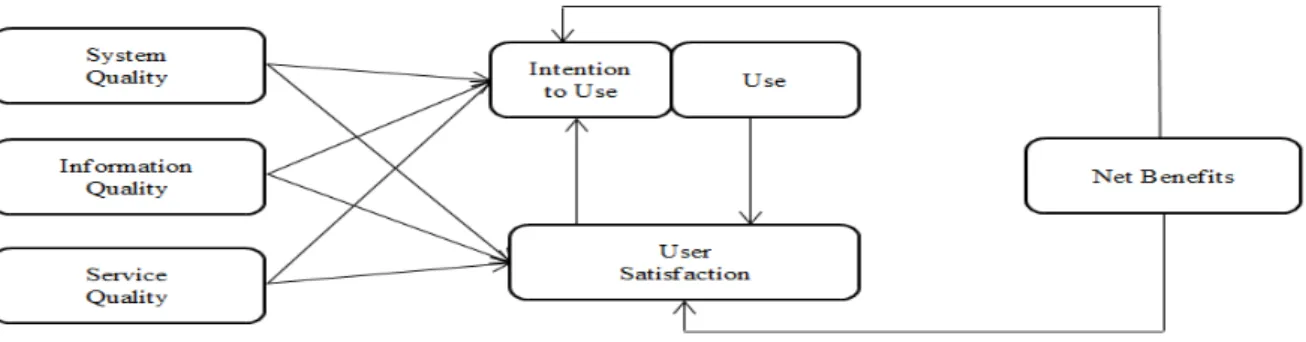
One of the most commonly used models in literature to evaluate the success of information systems in Information Systems Success Model (ISSM) developed by Delone and McLeon (1992) based on TAM. The relevant model consists of interrelated six variables as “system quality, information quality, system usage, user satisfaction, personal effect and organizational effect” (DeLone and McLean 1992). Personal effect and organizational effect in the model were combined by Seddon (1997) and stated as net benefit. DeLone and McLean (2003) revised ISSM and used the concept of net benefit by combining the concepts of personal effect and organizational effect in order to reflect the general consequence for the use of information systems. In addition, they included the service quality to quality dimension.
This model measuring the success of an information system in a multi-dimensional way indicates that the features of the system can be represented by the system quality, system-related services can be represented by the service quality and the output quality can be represented by the information quality. The effects of information system can be stated as intention to use, user satisfaction and net benefit. Intention to use means the strength of willingness to use by users. User satisfaction defines the perceptional reaction of users for the system. The net benefit takes into account the overall effects of the system (Chang et al. 2011). Each success dimension can be evaluated by the system users through the survey. Then, the success of information systems can be evaluated for each dimension. A low score for any success dimension indicates a deficiency in this field and efforts can be made accordingly to correct the deficiency (Holsapple and Lee-Post 2006).
Figure 2. Information Systems Success Model (DeLone and McLean, 2003)
System quality: Quality of an information system is evaluated in terms of some qualities such as reliability, flexibility, integration, availability, fast and adaptability to user demands and easy to use and learn (Hamilton and Chervany, 1981). Reliability used in the evaluation of information quality refers to the reliability of system quality, flexibility refers to adaptability of the system to changing demands of users, integration refers to the system allowing data to be integrated with various sources, availability refers to the ease of entering information to the system or getting information from the system, punctuality refers to system’s response level to transaction and information demands on time (Wixom and Todd 2005).
Information quality: It refers to the characteristics of the information and outputs produced by the information system such as being complete, accurate, up-to-date, reliable, sufficient, complete, precise and useful (DeLone and McLean 1992; Seddon,1997). Being complete used in the evaluation of information quality represents that the system provides all the necessary information, accuracy represents the user’s perception that information is correct, being up-to-date represents the user's perception of how up-to-date the information is(Wixom and Todd 2005). Since the information quality obtained from health information systems plays an important role in decision making and planning, the information needed by health professionals should presented. Poor information quality may increase medical errors and thus negatively affect patient care quality (Mohammed and Yusof 2012).
Service quality: It refers to the quality of the support that users receive from the IT department and support personnel. It is for the quality of the support provided by the information system designers for the problems and demands of the end users. Technical support for end users given by technical staff or businesses developing the information system will have a positive effect on the development of positive attitudes towards system use, system use and user satisfaction (Petter, Delone and McLean, 2008).
User satisfaction: It expresses satisfaction levels about whether the expectations of the employees using the information system and the administrators making decisions using system outputs are met or not. The most important criterion used in order to evaluate information system success is user satisfaction (DeLone and McLean 1992). Meeting user needs increases the satisfaction from the system and has a key role in the development of more useful information systems (Farzandipour et al. 2018). It is generally accepted that user attitudes are important determinants of information systems success. When users are satisfied with the information system, they are known to use it more frequently (Barki and Huff 1985).