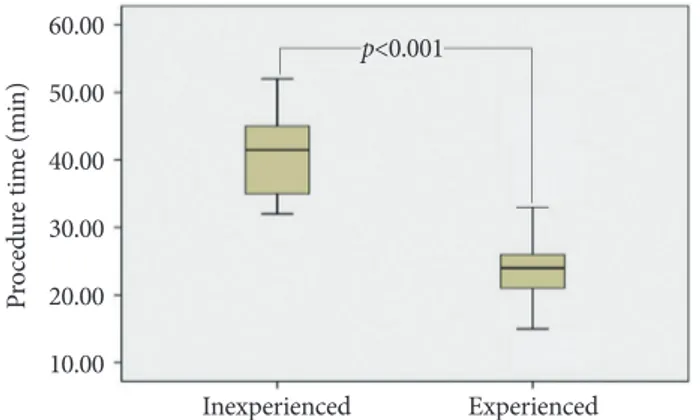
Experience of the endoscopists matters in endoscopic retrograde cholangiopancreatography in billroth II gastrectomy patients
Tam metin
Şekil
Benzer Belgeler
Though present study had some limitations when evaluating the effects of hyperthyroidism on flow-volume loops, some significant changes in MMEFR, FEF 25 , FEF 50 , FEF 75
In patients who developed delirium, the ages were significantly lower, the infection rates were significantly higher, and the length of hospitalization was significantly
Bu yazıda ERCP girişimi yapılan morbit obez bir hastada ameliyathane dışı sedoanaljezi uygulaması sunuldu ve sedoanaljezi uygulaması sırasında oluşabilecek
Objective: This study aimed to make an early diagnosis of endothelial dysfunction, the initial pathology of atherosclerosis in metabolic syndrome (MS) patients, and to investigate
Endoscopic retrograde cholangiopancreatography (ERCP) is an appropriate diagnostic and therapeutic modality that can be used both preoperatively for cysts
We suggest that emergency or early ERCP should be performed within 24–48 hours in elderly patients with acute cholangitis and biliary sepsis irrespective of the severity of the
17 performed ERCP for 127 patients with acute biliary pancreatitis and found a decrease in rates of mortality caused by biliary sepsis in patients who underwent early
To overcome these difficulties some technical modifications of conventional ERCP technique requiring changes in the position of the patient at the beginning,
