www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
The
efficacy
of
esmolol,
remifentanil
and
nitroglycerin
in
controlled
hypotension
for
functional
endoscopic
sinus
surgery
Aslı
Alkan
a,
Mehtap
Honca
b,
Ali
Alkan
c,∗,
Handan
Gülec
¸
d,
Eyüp
Horasanlı
daMu˘glaSıtkıKoc¸manUniversityEducationandResearchHospital,DepartmentofAnesthesiologyandReanimation,Mu˘gla,Turkey
bYozgatBozokUniversitySchoolofMedicine,DepartmentofAnesthesiologyandReanimation,Yozgat,Turkey
cMu˘glaSıtkıKoc¸manUniversitySchoolofMedicine,DepartmentofInternalMedicine,DivisionofMedicalOncology,Mu˘gla,Turkey
dAnkaraYıldırımBeyazıtUniversity,SchoolofMedicine,DepartmentofAnesthesiologyandReanimation,Ankara,Turkey
Received26July2018;accepted28August2019 Availableonline3October2019
KEYWORDS Remifentanil; Esmolol; Nitroglycerin; Functional endoscopicsinus surgery; Controlled hypotension Abstract
Introduction:Controlled hypotensionisareversible procedure inwhich thepatient’s base-linemeanarterialbloodpressureisreducedby30%andsustainedat60---70mmHgduringthe procedure.Itdecreasesbloodlossandprovidesclearsurgicalfieldduringtheprocedures.
Objectives:Thepurposeofthisstudywastocomparetheefficacyofcontrolledhypotension agentsesmolol,remifentanil,andnitroglycerininfunctionalendoscopicsinussurgery,interms ofhemodynamicchangesandimpactonthesurgicalefficiency.
Methods:Theresearchwascarriedoutasacohortstudy.Patientswhounderwentfunctional endoscopicsinussurgerywererandomizedinto3groups.Controlledhypotensionwasachieved withremifentanil(GroupR),esmolol(GroupE)andnitroglycerin(GroupN).Theefficacyofthe drugswastestedby comparingthelengthoftimewiththetargetedmeanarterialpressure, theamountofanestheticsused,surgicalfieldbleedingscoreandsurgeon’ssatisfaction.
Results:BetweenMaytoDecember2015,60patientswereincludedandrandomizedequally into3differentstudygroups.Themedianofthelengthoftimewiththetargetedmean arte-rialpressurewasshorterintheGroupRwhencomparedwithGroupE(p=0.01)andGroupN (p=0.14).Theamountofvolatileanestheticsusedwas25.0mL(15---51),43.0mL(21---105)and 40.0mL(26---97)inGroupsR,EandN,respectively(p<0.001).Whiletherewasmorebleeding withnitroglycerin,surgicalfieldbleedingscoreswerelowerinGroupRwhencomparedwith esmolol(p=0.001)andnitroglycerin(p<0.001).Theanalysis ofsurgeon’ssatisfactionscores concludedthatsurgeons weremoresatisfiedwiththegroup R(100%),whencomparedwith groupE(60%)andgroupN(30%)(p<0.001).
∗Correspondingauthor.
E-mail:[email protected](A.Alkan).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial. https://doi.org/10.1016/j.bjorl.2019.08.008
1808-8694/©2019Associac¸˜aoBrasileiradeOtorrinolaringologiaeCirurgiaC´ervico-Facial.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBYlicense(http://creativecommons.org/licenses/by/4.0/).
Conclusion: Lessvolatileagent,short time toachievecontrolled hypotension, stableblood pressure, lower surgical field bleeding scores and largerlength of time with the targeted meanarterialpressurewerefound astheadvantagesofRemifentanil.Lesscostly,efficiency ofachievingthetargetedmedianarterialpressureandlesspostoperativecomplicationswere theadvantagesofnitroglycerin.Infunctionalendoscopicsinussurgeryprocedures,appropriate controlledhypotensiveagentsshouldbeselectedaccordingtothepatients’characteristicsand advantages/disadvantagesofthedrugs.
© 2019 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
Introduction
FunctionalEndoscopicSinusSurgery(FESS)isanimportant wayofapproach,mostlyusedinpathologiesobstructingthe sinuses.In additiontoitsefficacy,the procedureprovides drainageofsinuseswithoutdamagingthenormalphysiology andanatomyofthenasalcavity.1TheFESSisgenerallyused
for the treatment of nasalpolyposis,recurrent acute rhi-nosinusitis,leakageofcerebrospinalfluid,fungalinfections, foreign objects in the nasal cavity, mucocele, periorbital abscess, epistaxisand tumors.2 The main complication of
theprocedure is bleeding.The bleedingcan decreasethe qualityofFESSandincreasetheriskofcomplications.Good control of bleeding provides better surgical success, less surgicaltraumaandshortsurgicaltime.3Forbleeding
con-trol,hypotensivemeasuresaregenerallypracticed,suchas appropriate patientpositioning, positive pressure ventila-tion,andhypotensiveagents.
Controlled Hypotension (CH) at a moderate level is defined as a reversible and controlled reduction of Mean ArterialPressure(MAP)to60---70mmHgora30%reduction ofbaselineMAP.4NumerousagentsareusedforCH.Volatile
anesthetics, opioids, sodium nitroprusside, nitroglycerin, hydralazine,trimethaphan,adenosine,␣-2blockersand -blockersarethemostcommonlyuseddrugsforCH.5There
arebothprosandconsfortheuseoftheseagents. The purposeof thisstudy istocompare theCHagents Esmolol,Remifentanil,andNitroglycerinforFESS,interms ofhemodynamicchangesandimpactsonsurgicalefficacy.
Methods
The study was conducted in Keciören Education and ResearchHospital,DepartmentofAnesthesiologyand Rean-imation.InstitutionalEthicsCommitteeapprovedthestudy protocol (no
B.10.4.˙ISM.4.06.68.49) and the study was in accordancewiththeethicalstandardslaiddowninthe1964 DeclarationofHelsinki.Allparticipantsgavetheirinformed consentpriortotheirinclusioninthestudy.
Between2015Mayand2015December,ASAI---IIpatients, betweentheagesof18---50andwhowerescheduledforFESS wereincludedinthestudy.ThepatientswithASAscoreof IIIandmore,medicationsincluding-blockers,opioidsand ones havingimpact onthecardiovascular system,chronic hypertension,coronaryarterydisease,arrhythmias,chronic obstructivepulmonarydisease,chronicrenalorhepatic
fail-ure, history of cerebrovascular disease, diabetes, severe anemia(less than 7gr/dL), coagulopathy, history of sinus surgery,historyofallergytooneofthestudydrugsandwho werepregnantorlactating wereexcludedfromthestudy. Sealedenvelopeswereusedtoassignthepatientsto treat-mentgroups;GroupR(remifentanil),GroupE(esmolol)and GroupN(nitroglycerin).Thepatientswererandomizedafter signed awritten informedconsentjust before the proce-dure.Twoanesthesiologistsfollowed thepatients:onefor randomizationand preparationof thedrug,onefor moni-toringanddocumentationoftheresults.Thustheobserver wasblinded.
Thepatients’gender,age,weight,ASAscoreand indica-tionsoftheFESS wererecorded.Patientsweremonitored byECG,pulseoximetry,invasive/noninvasivebloodpressure andBispectral Index (BIS).Thus HeartRate (HR), systolic arterialpressure,diastolicarterialpressure,MeanArterial Pressure (MAP), Oxygen Saturation (SpO2) and Bispectral
Index(BIS)(QuatroTM,AspectMedicalSystem,NewtonMA, USA)wererecorded.Afterrecordingpreoperative measure-ments,inductionofanesthesiawasperformedwith1mg/kg lidocaine (2%), propofol 2---3mg/kg and fentanyl 1g/kg IV.Patientswereintubatedwith0.6mg/kgrocuroniumand maintenanceof anesthesiawassustainedbywith sevoflu-rane2---4%,nitrousoxide50% andoxygen50%tokeepthe BIS in the 40---60 range. In addition, mechanical ventila-tionwascontinuedtoprovideanend-tidalcarbondioxide levelof32---36 mmHg.Allthepatientswerein45degrees supineposition.BeforestartingtheprocedureCHwas per-formedinstudygroups.InGroup R,remifentanilwasused with a loading dose of 1mcg/kg in 60sec. The mainte-nance of anesthesia was sustained with 0.1mcg/kg/min remifentaniland the dose increased to provide a MAP of 60---65mmHg.InGroupE,esmololwasusedwithaloading doseof1mg/kgin60sec.Themaintenancewassustained with0.4mg/kg/h esmolol and the dose increased to pro-videa MAPof60---65mmHg.InGroup N,nitroglycerinwas usedwitha maintenance dose of 2mcg/min toprovide a MAPof60---65mmHg.DuringtheprocedureHRlessthan50 beats/minweredefinedasbradycardiaanditwastreated with0.015mg/kgatropine.Inaddition,iftheMAPdecreased to less than 60mmHg for more than 60s, the dosage of thedrugis halvedandfollowed further.Iftheintolerable hypotensioncontinued,thentheCHmedicationwas termi-nated. AfterFESS wascompleted and thestudy drug was terminated,thepatientswerefolloweduptoopeningtheir eyesandextubationtime.
Table1 Thecharacteristicsofpatients.
Characteristics GroupR(n,range) GroupE(n,range) GroupN(n,range) Total(n,range) p
Age 36.5(18---56) 33.5(20---55) 47.5(19---65) 39(18---65) 0.02 Weight(kg) 78.0(60---100) 75.0(50---96) 74(60---96) 75(50---100) 0.90 Height(cm) 170(161---185) 171.5(163---176) 170(160---185) 170(160---178) 0.50 BMI(kg/m2) 26.9(20.3---35.0) 26.5(18.4---31.4) 25.4(20.7---32.4) 26.3(18.4---35.0) 0.83 Obese(n,%) 4(20.0%) 4(20.0%) 5(25.0%) 13(21.7%) 0.90 Male(n,%) 13(65.0) 17(85.0) 13(65.0) 43(%71.7) 0.26 ASAscore 0.62 ASA1 10(50.0%) 8(40.0%) 11(55.0%) 29(48.3%) ASA2 10(50.0%) 12(60.0%) 9(45.0%) 31(51.7%) PreoperativeSBP(mmHg) 135(118---157) 135(110---152) 133(117---155) 135(110---157) 0.92 PreoperativeDBP(mmHg) 76(61---89) 85(60---102) 77(60---107) 78(60---107) 0.02 PreoperativeMAP(mmHg) 96.5(83---111) 103.5(82---117) 100(88---120) 100(82---120) 0.41 PreoperativeHR(beats/hour) 79.7(51---107) 87.5(61---107) 84(55---100) 81(51---107) 0.61 PreoperativeSpO2(%) 96(92---98) 97.5(93---100) 97(91---100) 97(92---100) 0.19
ASA,Americansocietyofanesthesiologists;DBP,diastolicbloodpressure;HR,heartrate;MAP,Meanarterialpressure;SBP,systolicblood pressure;SpO2,Capillaryoxygensaturation;BMI,Bodymassindex.
Duringprocedures;HR,SAP,DAP,MAP,SpO2,BIS, bleed-ingscores,extradrugsusedweremonitoredin5,10,15,20, 25,30,40,50,60,80,100,120min.Inaddition,thesame
parameterswere recordedin the periodoftime between
the terminationof CH andextubation. Other medications
usedwere recorded.BleedingScores (BLS) weredeclared
bytheprimarysurgeon.(BLS-0,Nobleeding;BLS-1,minimal bleeding,noneedforaspirationneed;BLS-2,minimal bleed-ing,theinfrequentnecessityofaspiration;BLS-3,minimal bleeding, frequentnecessity ofaspiration;BLS-4, moder-atebleeding,frequentnecessityofaspiration;BLS-5.Severe bleeding).Thetotalamountofthevolatileagent
(Sevoflu-rane)usedwasdocumented.Theefficacyofthedrugswas
evaluatedwithLTMAP,SurgicalFieldBleedingScore(SFBS)
and Surgeon’s Satisfaction (SS).SS were graded as
excel-lent,good,moderate,bad, andverybad.Foranalysis,SS
weregroupedassatisfied(goodandexcellent)andnot
sat-isfied(moderate, bad,verybad). To increasethe efficacy
andoptimal subjectivityofthe evaluationprocess,only 2 surgeonswereincludedinthestudy.
Baseline characteristics of the patient group were
described using proportionsfor dichotomous and
categor-ical variables. Differences between continuous variables
wereassessedwiththeStudentt-test andnon-parametric
tests for repeated measures (Friedman Test). Differences
between non-parametric variables were analyzed with
Mann---WhitneyUtest.TheChi-SquareorFisherexacttests
were used to compare categorical variables. All analyses
were performed using SPSS 17.0 for Windows(IBM Corp.,
Armonk,NY).Thep-valueoflessthan0.05wasconsidered
asstatisticallysignificant.
Results
BetweenMaytoDecember2015,60patientswereincluded
andrandomizedinto3differentstudygroups.Thebaseline characteristics ofthepatients aresummarizedin Table1. Themedian lengthofoperationswas60min(50---120min.) (Table2). Themedian lengthof operationswasshorter in
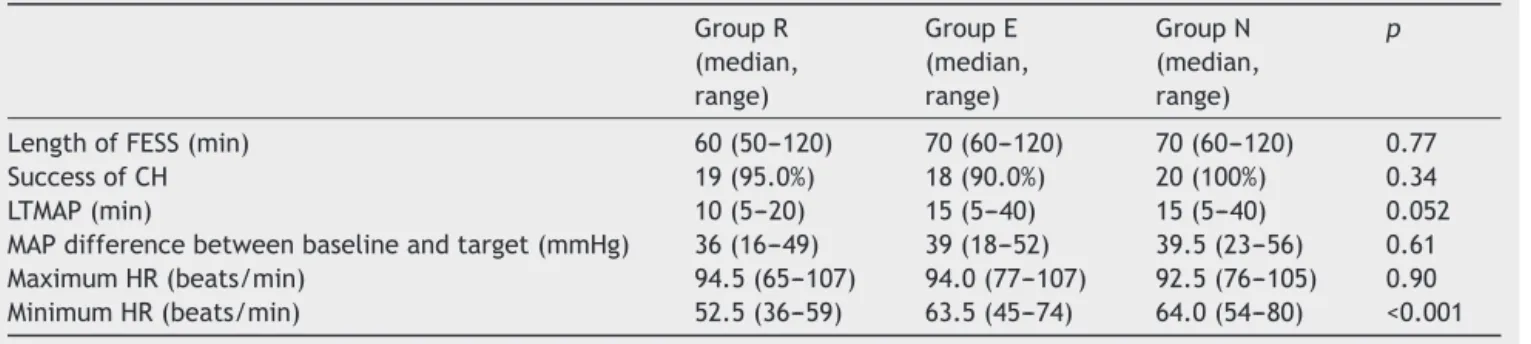
GroupR(60vs.70,p=0.43).In95%ofthepatients,CHgoals wereachieved.In allstudy groups success ratewasmore than90%anditwas100%inGroupN.ThemedianLTMAPwas 10(5---20)minutesinGroupR,15(4---40)minutesinGroupE and15(5---40)minutesinGroupN(p=0.052)(Fig.1a).Itwas shorterinGroupRwhencomparedwithGroupE(p=0.01) andGroupN(p=0.14).The analysisof HRconcludedthat themaximumHRduringproceduresweresimilarinallstudy armsgroups(p=0.90) andGroupRwereexposed tomore bradycardia(p<0.001)(Table2)(Fig.1b).
Duringtheperioperativeperiod,extramedicationswere usedin 10 (50%) patients inGroup N,7 (35%)in Group R and3(15%)patientsinGroupE(p=0.051)forhemodynamic changes(Table3).Inaddition,medicationsusedafter termi-nationofCHwerealsosimilarbetweengroups.Theamounts of sevofluraneas avolatile anesthetic usedwere 25.0mL (15---51),43.0mL(21---105)and40.0mL(26---97)inGroupsR, EandN,respectively(p<0.001).Therewerepostoperative complicationsin10%ofGroupR,5%ofGroupEandnoneof theGroupNpatients(p=0.34).Bronchospasmwasobserved asacomplicationinthesegroups.
The analysis of efficacy was performed by comparing LTMAP,SFBS,andSSinstudy arms.The SFBSwere2(1---2) in Group R, 2 (2---3) in Group E and 3 (2---4) in Group N (p<0.001).Whiletherewasmorebleedingwith nitroglyc-erin,SFBSscoreswerelessinGroupRwhencomparedwith esmolol(p=0.001)andnitroglycerin(p<0.001).The analy-sisofSSscoresconcludedthatsurgeonsweremoresatisfied withGroupR(100%),whencomparedwithGroupE(60%)and GroupN(30%)(p<0.001).Therewasapositivecorrelation withSFBSandSSscores(r=0.43,p<0.001).
Discussion
Inthepresent study,weaimedtocomparetheefficacyof threeCHagents,Remifentanil, esmolol,nitroglycerin.We concludedthatlessvolatileagent,shorttimetoapproach CH, stable blood pressure, less SFBS and short operation time length were the advantages of Remifentanil.
Effi-Table2 TheparametersunderFESSandCHinstudyarms. GroupR (median, range) GroupE (median, range) GroupN (median, range) p
LengthofFESS(min) 60(50---120) 70(60---120) 70(60---120) 0.77
SuccessofCH 19(95.0%) 18(90.0%) 20(100%) 0.34
LTMAP(min) 10(5---20) 15(5---40) 15(5---40) 0.052
MAPdifferencebetweenbaselineandtarget(mmHg) 36(16---49) 39(18---52) 39.5(23---56) 0.61
MaximumHR(beats/min) 94.5(65---107) 94.0(77---107) 92.5(76---105) 0.90 MinimumHR(beats/min) 52.5(36---59) 63.5(45---74) 64.0(54---80) <0.001 MAP(mmHg) HR(/min) 110 100 90 80 70 60 50 90 85 80 60 55 50 75 70 65 PREOPInduction 5’ 10’ 15’ 20’ 25’ 30’ 40’ 60’ 80’ 100’ 120’ 50’ PREOPInduction 5’ 10’ 15’ 20’ 25’ 30’ 40’ 60’ 80’ 100’ 120’ 50’ Group-R Group-E Group-N Group-R Group-E Group-N 65mmHg Minutes Minutes
a
b
Figure1 ThemedianvaluesofMAPandHRduringCH.
cacy of approaching targeted MAP and less postoperative
complicationsweretheadvantagesofNitroglycerin.
Functional endoscopic sinus surgery is widely used
becauseofitsfeasibilityandlowcomplicationrates. Bleed-ingisthemostcommoncomplicationofFESS.6Inadditionto
othersurgicalprocedures,CHisalsointegratedwithFESSto decreasethebleedingduringFESSandprovidebetter sur-gical field.7 Numerous agents areused for CH. The ideal
hypotensiveagentshould beeasy toadminister and safe. In addition,it should have a rapid onset of action, short half-life,easilypredictable andobservablesideeffects.8,9
The most commonly used agents are magnesium sulfate, vasodilators (sodium nitroprusside), nitroglycerin, potent inhaledanestheticsandBeta-adrenergicantagonists.5There
arebothprosandconsfortheseagentsandthereare numer-ousdataaboutcomparingtheseagents.Inthepresentstudy wetriedtocomparethreemostcommonlyusedmedications inCHandevaluatetheirefficacyinFESS:remifentanil (-opioidreceptoragonist),esmolol(short-acting-adrenergic receptorblocker)andnitroglycerin(vasodilator).
In the literature, there arenumerous studies compar-ing2drugs,especiallyesmololandnitroglycerin.However, therearelimitedstudiescomparingthreeagentsforCH. Sri-vastavaetal.concludedthatnitroglycerinwassuperiorto esmololwithitsshorter LTMAP,lowerbleedingscoresand producing lessreflex tachycardia.10 Inaddition,the study
whichcomparedesmololandnitroglycerininnasalsurgery showedthatesmololprovidedmorehemodynamicstability and better surgical fieldcontrol.11 Our results were
con-Table3 Theparametersevaluatingtheefficacyofgroups.
GroupR(n,%) GroupE(n,%) GroupN(n,%) p
Volatileuse(Sevoflurane),mL(median,range) 25.0(15---51) 43.0(21---105) 40.0(26---97) <0.001
Extramedicationforhemodynamicchanges 7(35.0) 3(15.0) 10(50) 0.062
ExtramedicationafterterminationofCH 1(5.0) 0(0) 0(0) 0.36
Postoperativecomplications 2(10) 1(5) 0(0) 0.34
MaximumSFBS(median,range) 2(1---2) 2(2---3) 3(2---4) <0.001
Surgeon’ssatisfaction <0.001 Verybad 0(0) 0(0) 1(5) Bad 0(0) 0(0) 5(25) Moderate 0(0) 8(40) 8(40) Good 10(50) 9(45) 6(30) Excellent 10(50) 3(15) 0(0)
sistent with the data in the literature. There was more
hypotension, worseSFBS,moreneed for extramedication
andworseSSscoresinthenitroglyceringroup.
Esmololisa-adrenergicreceptorblockerandhasbeen
usedforCHformanyyears.Inaddition,vasoconstrictionin arterioles andprecapillary sphincters providesless
bleed-ing and better operation field.12 The efficacy of esmolol
in CH has been compared with others in numerous stud-ies. Degoute et al. compared esmolol, Remifentanil, and nitroprussideandconcludedthat esmololwasmore effec-tivefordecreasingmiddleearbloodflow.13Pillietal.also
showed theefficacy andsafety ofesmolol in CH.14 In our
study, esmolol provided effective CH and stable hemody-namicparametersduringtheFESS.
Esmololandnitroglycerinprovidehypotensionbydirectly actingoncardiovascularstructures.However,Remifentanil is anultra-short-acting -agonistopioidreceptor.Itsmost important advantages are short half-life and not having effects on microcirculation.5---15 As a CH agent, its
supe-riority over fentanyl and sufentanil has been reported.1
AlthoughtheefficacyofRemifentanilhasbeendocumented in our study, it has a dose-dependent, depression effect on the sinoatrial node. The studies, comparing Remifen-tanil with others, documented more bradycardia with Remifentanil.16,17 Consequently, it is recommended to be
avoided in patients with a cardiac dysfunction or risk of bradyarrhythmia.18,19Inourstudy,weobservedlowerHRsin
GroupRandin3(15%)patientsweretreatedwithatropine. The study had some inevitable limitations. The evalu-ation of CH efficacy was performed by assessing SS and SFBS.However,thosearesubjective parameters.We tried to decrease the bias related with subjectivity by work-ing with 2 surgeons. Objective parameters could provide a more efficient analysis. The inclusion of more patients couldenableus todofurtheranalysis.The patients were older in the Group N when compared with others. How-ever,becausetherenal,hepaticfunctionsandperformance scoresofthepatientsweresimilar,weignoredtheage dif-ferencebetweengroups.
Conclusion
Remifentanilprovidesalowersurgicalfieldbleedingscore, stable blood pressure and short time to targeted mean arterial blood pressurewith theuse of less volatile anes-thetic agent. However the nitroglycerin group produces easy control of blood pressure with less postoperative complications.Asaresult,appropriateCHagentsshouldbe selectedaccording topatients’characteristics and advan-tages/disadvantagesofdrugsduringFESSprocedures.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.¸enocakS D. Otorinolaringoloji BvBC B. ˙Istanbul: Nobel Tıp Kitabevleri;2000.p.1730---80.
2.KingstonHG,HirshmanCA.Perioperativemanagementofthe patientwithasthma.AnesthAnalg.1984;6:844---55.
3.KayhanZ.KlinikAnesteziGenis¸letilmis¸.3.baskıAnkara:logos Yayincilik;2004.p.496---501.
4.MorenoDH,CacioneDG,Baptista-SilvaJC.Controlled hypoten-sionversusnormotensiveresuscitationstrategyforpeoplewith rupturedabdominalaorticaneurysm.CochraneDatabaseSyst Rev.2018;6:CD011664.
5.DegouteCS. Controlledhypotension:a guidetodrugchoice. Drugs.2007;67:1053---76.
6.Stammberger H, Posawetz W. Functional endoscopic sinus surgery.Concept,indicationsandresultsoftheMesserklinger technique.EurArchOtorhinolaryngol.1990;247:63---76. 7.Javer AR, Alandejani T. Prevention and management of
complicationsinfrontalsinussurgery.Otolaryngol ClinNorth Am.2010;43:827---38.
8.SimpsonP.Perioperativebloodlossanditsreduction:therole oftheanesthetist.BrJAnaesth.1992;69:498---507.
9.CincikasD,IvaskeviciusJ,MartinkenasJL,BalserisS.Aroleof theanesthesiologistinreducingsurgicalbleedinginendoscopic sinussurgery.Medicina.2010;46:730---4.
10.SrivastavaU,DupargudeAB,KumarD,JoshiK,GuptaA. Con-trolled hypotension for functional endoscopic sinus surgery: comparisonofesmololandnitroglycerine.IndianJOtolaryngol HeadNeckSurg.2013;65Suppl2:440---4.
11.GuneyA,Kaya FN,YavascaogluB,GurbetA, SelmiNH,Kaya S, et al. Comparison of esmolol to nitroglycerine in con-trolling hypotension during nasal surgery. Eurasian J Med. 2012;44:99---105.
12.NairS,Collins M,HungP,Rees G,Close D,Wormald PJ.The effectofbeta-blockerpremedicationonthesurgicalfieldduring endoscopicsinussurgery.Laryngoscope.2004;114:1042---6. 13.Degoute CS, Ray MJ, Manchon M, Dubreuil C, Banssillon V.
Remifentanil and controlled hypotension; comparison with nitroprussideoresmololduringtympanoplasty.CanJAnaesth. 2001;48:20---7.
14.Pilli G, Guzeldemir ME, Bayhan N. Esmolol for hypotensive anesthesia in middle ear surgery. Acta Anaesthesiol Belg. 1996;47:85---91.
15.RyuJH,SohnIS,DoSH.Controlledhypotensionformiddleear surgery: a comparison between remifentanil and magnesium sulphate.BrJAnaesth.2009;103:490---5.
16.Yun SH, Kim JH, Kim HJ. Comparison of the hemody-namiceffectsofnitroprussideandremifentanilforcontrolled hypotension during endoscopic sinus surgery. J Anesth. 2015;29:35---9.
17.ZhangX,HuQ, LiuZ,HuangH,ZhangQ,DaiH.Comparison between nitroglycerin and remifentanil in acute hyperv-olemic hemodilution combined with controlled hypotension during intracranial aneurysm surgery. Int J Clin Exp Med. 2015;8:19353---9.
18.KomatsuR,TuranAM,Orhan-SungurM,McGuireJ,RadkeOC, Apfel CC.Remifentanil forgeneral anaesthesia:asystematic review.Anaesthesia.2007;62:1266---80.
19.DelBlancoNarcisoBB,JimenoFernandezC,AlmendralGarrote J,AnadonBaselgaMJ,ZaballosGarciaM.Effectsofremifentanil onthecardiacconductionsystem.Ourexperienceinthestudy ofremifentanilelectrophysiologicalproperties.CurrPharmDes. 2014;20:5489---96.