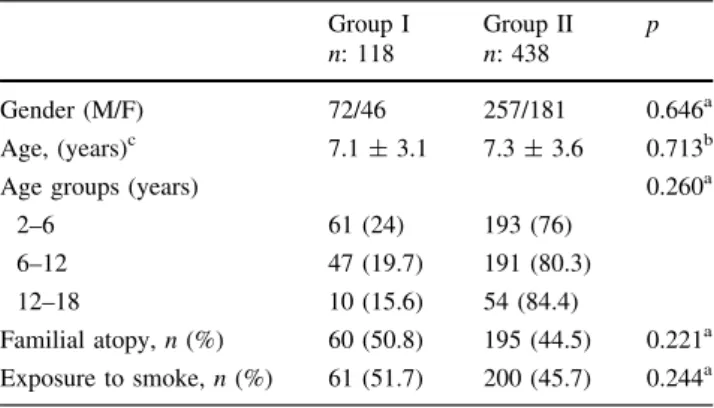
Does adenoid hypertrophy affect disease severity in children with allergic rhinitis?
Tam metin
Şekil
Benzer Belgeler
Adenoid hipertrofisi gelişiminde atopinin ve küf mantarı duyarlılığının rolünün araştırıldığı bu çalış- mada, adenoid hipertrofisi olan hastalarda deri testi
(2) reported that left ventricle functions preserved in chronic obstructive pulmonary disease patients with mild hypoxemia by a study with MRI (magnetic resonance imaging).. Amano
In conclusion, although the GAGS score was higher in male patients and males had more severe acne lesions clinically, it was found that female patients were more
(6) compared preanesthetic effects of transmucosal DEX 1 μg kg -1 , oral midazolam 0.5 mg kg -1 and oral clonidine 4 μg kg -1 on postoperative pain and anxiety in children,
The differ- ences of both groups according to gender, age, antithyroglobuline (anti-Tg), anti thyroid peroxidase (anti-TPO), thyroid stimulating hormone (TSH), free
Aim: To evaluate the prevalence of adenotonsillar Actinomyces with histopathological findings and to determine the relationship of Actinomyces with allergic rhinitis
Comparison of the oral steroid group and macrolide group revealed significantly better radiological grading and odour test changes for the oral steroid group, but no
The reduction of the inferior turbinates with RFA seems to be effective, especially in patients with allergic rhinitis, not only for nasal obstruction but also for the reduction
