Evaluation of Nursing Students' Knowledge, Belief, and Practice of Hand Hygiene
Tam metin
Şekil

Benzer Belgeler
Ancak klinik uygulama yapan öğrencilerin COVID-19 sürecinde bireye temas etmesi ile Merhamet Ölçeği toplam puan ortalamaları arasında istatistiksel olarak anlamlı
Muramatsu ve arkadaşları (2019) tarafından geliştirilen “Hemşirelik Öğrencileri İçin Etik Duyarlılık Anketi (EDA-HÖ)” hemşirelik öğrencilerinin etik
This study is important because it is the first study showing the perceptions of nursing students about the profession by metaphor and the effect of school climate on these
Academic environment is characterized by the conditions of education under theoretical aspects which contribute to develop knowledge on the practical aspects to which
Superficial muscle on the ulnar side of the hand O: palmar apon.+flexor retinaculum.. i: skin on the ulnar margin of the hand n.:
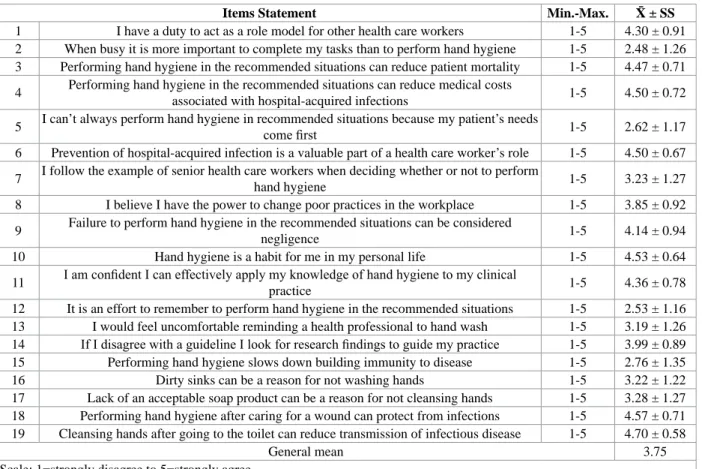
In accordance with all these findings on hand hygiene, it was discovered that participants have knowledge about general hand cleanness and care, cross contamination between
The course content includes the concept of communication, types of communication, factors affecting communication, effective communica- tion skills, factors affecting
During the nursing practices, it was determined that the average total “negative discrimination against the elderly” score of the stu- dents who worked with the elderly
