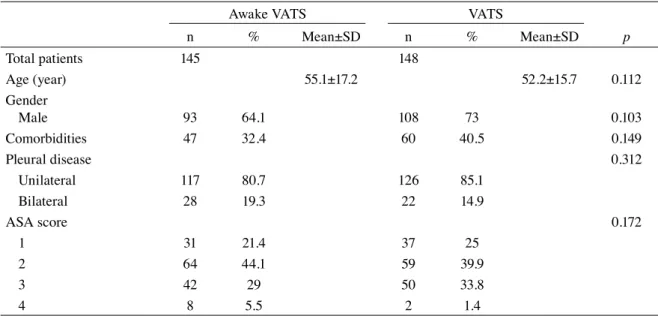
Comparison of awake and intubated video-assisted thoracoscopic surgery in the diagnosis of pleural diseases: A prospective multicenter randomized trial
Tam metin
Şekil

Benzer Belgeler
Bu çalışmada, yarı oturur pozisyonda, küçük tek bir port kullanılarak kamera ve diğer enstrümanların toraks içine alındığı (uniportal) bilateral sempatekto-
In conclusion, WALANT technique was associated with reduced early postoperative pain, opioid consumption and DSOR compared to that in general anesthesia plus tourniquet method
Single-port VATS applications with advantages of shorter port incision length, operation , and drainage time and shorter hos- pital stay will become commonly used in
The du- ration of intervention (time between the skin preparation to completion of the intervention), the time to achieve surgical anesthesia (the time between the completion of
Using wide-awake anesthesia in hand surgery, especial- ly in finger surgeries, decreases anesthesia cost, shortens hospital stay, and increases patient satisfaction.. During
Awake VATS and VATS patients were compared in terms of operative time, reason for conversion to general anesthesia, complications, diagnostic accuracy, procedure
Conclusion: Transbronchial biopsy can be performed safely in elderly patients, with similar diagnostic success and complication rates to younger patients.. Key words:
Conclusion:As a result, as all the groups have preconditioning potential, although we did not find a significant difference between fentanyl-based TIVA group and
