A N A T O M I C V A R I A T I O N S
B. Durgun Æ A.H. Yu¨cel Æ E.D. Kizilkanat Æ F. Dere
Multiple arterial variation of the human upper limb
Received: 6 September 2001 / Accepted: 2 December 2001 / Published online: 8 June 2002 Ó Springer-Verlag 2002
Abstract A case report of multiple variations involving
the arteries of the upper limb in a single cadaver is
presented. In addition to the proximal origin of the
ar-teries unusual arterial patterns on both the right and left
sides were present. On the right side, the subscapular
artery gave rise to a large posterior circumflex humeral
artery in addition to the thoracodorsal and circumflex
scapular arteries. On the left side, the radial and ulnar
arteries arose from the brachial artery at the level of
arm, with their origins being opposite to the usual
ar-rangement. There was an arciform anastomosis between
the radial and ulnar arteries, with the radial recurrent
artery arising from the concavity of the arch. The course
of both the radial and ulnar arteries was normal at the
wrist and hand, except for the absence of the first palmar
metacarpal artery and an early bifurcation of the second
palmar metacarpal artery. The French version of this
article is available in the form of electronic
supplemen-tary material and can be obtained by using the Springer
LINK
server
located
at
http://dx.doi.org/10.1007/
s00276-002-0011.
Variations arte´rielles multiples du membre supe´rieur
Re´sume´ Nous rapportons un cas de variations multiples
inte´ressant les arte`res du membre supe´rieur rencontre´es
sur le meˆme cadavre. En plus de l’origine proximale des
arte`res, on trouvait une disposition inhabituelle des
coˆte´s droit et gauche. A droite, l’arte`re subscapulaire
abandonnait
une
volumineuse
arte`re
circonflexe
hume´rale poste´rieure en plus de l’arte`re thoraco-dorsale
et de l’arte`re circonflexe de la scapula. Du coˆte´ gauche,
les arte`res radiale et ulnaire naissaient de l’arte`re
brac-hiale au niveau du bras et leurs origines e´taient dispose´es
inversement a` la disposition habituelle. Les arte`res
rad-iale et ulnaire e´taient relie´es par une anastomose
arci-forme.
L’arte`re
re´currente
radiale
naissait
de
la
concavite´ de cette arche. Les arte`res radiale et ulnaire
avaient un trajet normal au poignet et a` la main, a`
l’exception de l’absence de la premie`re arte`re
me´ta-carpienne palmaire et de la bifurcation pre´coce de la
deuxie`me arte`re me´tacarpienne palmaire.
Keywords Axillary artery Æ Brachial artery Æ
Arterial variation Æ Embryology
Introduction
The arterial pattern of the human upper limb shown in
textbooks is rarely encountered [16], withmajor and
minor variations being well documented. While
Tied-eman [13] was the first to describe these variations
sys-tematically, Quain’s series [11] was the first to provide
sufficient data for statistical evaluation. Some reports
have classified these variants and subdivided them into
groups [1, 4, 6, 8, 14], while others deal only with
indi-vidual examples of unusual patterns [2, 3, 7, 9, 10, 15].
These arterial variations can best be explained on the
basis of the embryological development of the vascular
networks in the upper limb.
The present case showed different arterial patterns on
the left and right sides. Its importance is explained from
anatomical, embryological and clinical viewpoints.
Case report
The dissection was conducted on both upper limbs and axilla of a 50-year-old-male cadaver as part of a teaching programme. The unusual branching of the principal arteries on the right side was different from those on the left. No scarring or surgical incisions Surg Radiol Anat (2002) 24: 125–128
DOI 10.1007/s00276-002-0011-z
The French version of this article is available in the form of electronic supplementary material and can be obtained by using the Springer LINK server located at http://dx.doi.org/10.1007/s00276-002-0011
B. Durgun (&) Æ A.H. Yu¨cel Æ E.D. Kizilkanat Æ F. Dere Department of Anatomy, Faculty of Medicine,
C¸ukurova University, 01330 Adana, Turkey E-mail: [email protected]
Tel.: +90-322-3386530 Fax: +90-322-3386572
were apparent in the skin. The nomenclature used in this report is the Terminologia Anatomica authorized by the FCAT in 1998 [12].
On the right side, the thoracoacromial and lateral thoracic aa. arose from the 1st part of the axillary a.; however these had been sacrificed by the students. The subscapular a. arose from the medial aspect of the 2nd part of the axillary a. Arising from the sub-scapular a. the posterior circumflex humeral a. then passed poste-riorly with the axillary n. through the lateral axillary space, after which its course and distribution followed the usual pattern (Fig. 1). The thoracodorsal a. arose from the subscapular a. as an anterior terminal branch, while some 4 cm distal to the origin of the subscapular a. the circumflex scapular a. arose as a posterior terminal branch. The latter curved around the lateral border of the scapula to supply the muscles on the dorsum of scapula and con-tributed to an extensive arterial anastomosis.
The subscapular n. passed behind the axillary and posterior circumflex humeral aa. The musculocutaneous n. passed between the axillary a. and coracobrachialis; the remaining branches of the brachial plexus were normal. The anterior circumflex humeral a. and a. profunda brachii arose from the lateral and inferior aspect of the 3rd part of the axillary a., respectively: both then followed their normal course.
On the left side, the subscapular a. arose from the 1st part of the axillary a.; however, its course and branching were usual (Fig. 2A). The profunda brachii, arising from the origin of the brachial a., had neither middle nor radial collateral branches. The most striking variation on the left side, however, was the high division of the brachial a., 3.5 cm distal to the inferior border of teres major (15.5 cm proximal to the intercondylar line), giving rise to the radial and ulnar aa. deep to biceps brachii (Fig. 2B). Two centimetres distal to its origin from the medial side of the brachial a. the radial a. crossed anteriorly and laterally to the ulnar a. and then followed the median n. down the lateral side of the arm. It gave muscular branches to biceps brachii at the crossing point and then passed down the arm between the medial border of the short head of biceps brachii and the median n. (Fig. 2A). The radial a. initially passed medial to the median n. and then anterior, leaving the nerve 2.5 cm proximal to the apex of the cubital fossa. In the forearm, it was situated between bra-chioradialis and pronator teres until 8 cm proximal to the wrist, where it became superficial, being covered only by skin, subcuta-neous tissue and deep fascia.
The ulnar a., the larger terminal branch of the brachial a., arose from the lateral side of the brachial a. and curved medially to lie on the medial side of the arm and forearm. As well as maintaining a close relationship with the ulnar n. and its usual branches, the ulnar a. gave rise to the superior and inferior ulnar collateral aa. 3 cm and 13 cm distal to its origin, respectively (Fig. 2B). The common interosseous a., a branchof the ulnar a., was approximately 1 cm in length, passing initially deep to pronator teres, then flexor digito-rum profundus, continuing distally on the anterior surface of the interosseous anterior a. The anterior interosseous a. gave off muscular branches as well as nutrient branches to radius and ulna. At the proximal border of pronator quadratus it pierced the int-erosseous membrane to gain access to the dorsum of the forearm and anastomosed with the posterior interosseous a.; however, it was most closely related to the anterior interosseous n.
Two centimetres above the lateral border of pronator teres an arciform anastomosis passing anterior to supinator was present as an oblique connection between the radial and ulnar aa.: it was 2.5 cm in length (Fig. 3). The recurrent radial a. arose from the concavity of the arch, while four rami arose from its convexity supplying supinator, and the long and short extensor carpi radialis mm. Both the radial and the ulnar aa. showed a normal position at the wrist and in the hand forming the superficial and deep palmar arches. There were, however, some exceptions: the radial a. passed under the flexor retinaculum, the 1st palmar metacarpal a. was absent, there was an early bifurcation of 2nd metacarpal a., and the connection between the 2nd dorsal metacarpal a. and the perfo-rating a. was via an anastomosis. No major variations in the muscles or brachial plexus were observed.
Discussion
The distribution and course of the arteries of human
upper limb are highly variable. The variations reported
to date can be classified into six groups to facilitate
discussion:
i) anomalous branching of the axillary a. [1, 7, 9, 17],
ii) variations in the point of origin of brachial branches
[3, 6, 8, 9, 14, 17],
iii) unusual course and distribution of brachial branches
[3, 8, 10],
iv) absence of the radial a. [10],
v) presence of an accessory brachial a. [8, 10, 15],
vi) variations in the arteries of hand [3, 4, 6].
In the present case the right subscapular a. that
normally arises from the 3rd part of the axillary a. arose
instead from the 2nd part. In addition to the
thoraco-dorsal and circumflex scapular aa., it also gave rise to
the posterior circumflex humeral a. The profunda
bra-chii also arose from the 3rd part of axillary a. Pestemalci
et al. [9] reported a common trunk of the subscapular
and posterior circumflex humeral aa. in 32% of their
Turkishcases.
In the present case the radial and ulnar aa. not only
arose high up, but also on the opposite side to usual. The
radial a. then crossed the ulnar to pass laterally in the
arm and forearm. This differs from the observations of
Danenow [2], in which the variation of the upper limb
vessels was at the level of forearm; however, it is similar
to the case described by Yu¨cel [17]. The radial and ulnar
aa. in the present case may not be regarded as either a
superficial brachial or a superficial ulnar a. because both
Fig. 1. Branches of the right axillary a. and their relationship withthe nerves. 1, pectoralis minor; 2, musculocutaneous n.; 3, thoracoacromial a. (sacrificed); 4, lateral thoracic a. (sacrificed); 5, axillary a.; 6, muscular branches of the axillary a.; 7, anterior circumflex humeral a.; 8, subscapular a.; 9, subscapular n.; 10, posterior circumflex humeral a.; 11, axillary n.; 12, vascular pedicle of vastus medialis; 13, thoracodorsal a.; 14, circumflex scapular a 126
arteries were deep and did not bifurcate in the cubital
fossa.
The arterial supply of biceps brachii in the present
case was not classified in the study by Kanbayashi et al.
[5]. An oblique arciform vessel directly connecting the
radial and ulnar aa. as reported here has not been
pre-viously reported.
Absence of the left 1st metacarpal palmar a., early
bifurcation of the left 2nd metacarpal palmar a., and the
course of these branches along the metacarpals, together
with the presence of an anastomosis between the
per-forating and the 2nd dorsal metacarpal aa. in the present
case, differ from those reported previously. The 2nd
dorsal metacarpal a. is particularly important because of
its high incidence, as well as in providing a collateral
pathway from the dorsum to the palm of hand [4].
Variation of the axillary branches was limited to the
right side, while those of the brachial branches were on
the left side. Although these variable branches of the
axillary a. are well known as individual occurrences, the
multiple patterns described here have not previously
been reported in a single individual.
On the basis of the embryological development of
these arteries and the reported adult anomalies, the
de-velopment of this arterial pattern may be explained as
the follows:
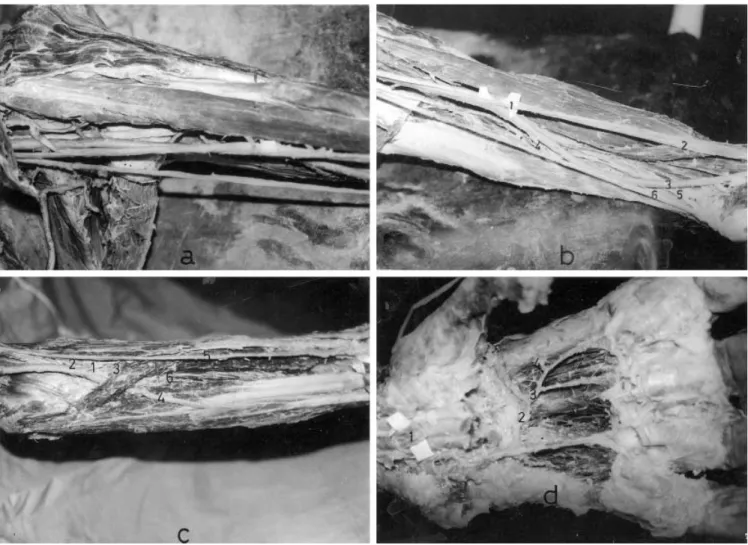
Fig. 2. A Left axillary a. and the muscular branches of the left radial a. to biceps brachii. B Proximal origin of the radial and ulnar aa. from the left brachial a. 1, radial a.; 2, median n.; 3, ulnar a.; 4, superior collateral ulnar a.; 5, inferior collateral ulnar a.; 6, ulnar n. C Course of the left radial and ulnar aa. at the level of the forearm. 1, anastomosis between the radial and ulnar aa. in the cubital fossa; 2, radial recurrent a.; 3, muscular branches; 4, ulnar a.; 5, radial a.; 6, anterior interosseous a. D Arterial pattern of the left hand. 1, radial a.; 2, deep palmar arch; 3, 2nd metacarpal palmar a.; 4, perforating a.
Fig. 3. Diagram of the proposed embryological development of the arteries in the present case. u, ulnar a.; sr, superficial radial a.; a, axial a.; c, anastomotic connection; ia, anterior interosseous a.; dotted line, regression part
i) The normal relationship between the arteries and the
nerves in the present case suggests that the axial a.
is normally derived from the 7th cervical
interseg-mental a.
ii) The proximal branching of the main arteries,
to-gether with the presence of unusual compound
ar-terial segments, suggests that the longitudinal
anastomoses occurring between intersegmental aa.
did not degenerate.
iii) The aberrant vessel connecting the radial and ulnar
aa. at the level of cubital fossa may occur as a result
of the regression of the primitive axial a. along the
arm, with the anastomoses between the primitive
axial, radial and ulnar aa. persisting.
iv) Not only regression of the primitive axial a. along
the arm, but also regression of the proximal part of
the superficial brachial-radial a., as reported by
Poteat [10] and Gonzales-Compta [3], may be the
cause of the high origin of the radial and ulnar aa.
from the brachial a. In the present case it appears
that the ulnar a. developed prior to the median a., as
postulated by Poteat. In addition, there may also be
an anastomotic connection between the primitive
ulnar and brachial-radial system in the present case.
Regression of the proximal part of the
brachial-ra-dial system and the distal part of the ulnar system,
together with a persistent anastomotic connection
between the radial and ulnar systems at the level of
arm, may be responsible for the main branches of
the brachial a. arising opposite to normal. This type
of arterial development is consistent withthe studies
of De Vriese, Mu¨ller and Senior as cited by
Mc-Cormack et al. [8] (Fig. 3). The presence of the
an-terior interosseous a. suggests that the primitive
axial a. at the level of forearm did not regress in the
present case.
v) The variations observed in the left hand may
rep-resent retention of the primitive pattern established
during prenatal growth.
The increasing use of invasive diagnostic and
inter-ventional procedures in cardiovascular diseases makes it
important that the type and frequency of vascular
variations
are
well
documented
and
understood.
Branches of the upper limb arteries have been used for
coronary bypass and flaps in reconstructive surgery. The
atypical distribution of the subscapular system, as in the
present case, may result in modified arches of rotation or
foreshortened pedicular lengths for latissimus dorsi and
serratus anterior, as well as for ortho- and parascapular
flaps. The anomalous origin and course of the radial a.
may result in some surprise and potential errors during
elevation of a radial forearm flap. Modifications of the
palmar arterial supply are also of practical importance
in hand reconstructive microsurgery. If the distal part of
the radial a. passes under the flexor retinaculum and
gives rise to a modified 1st palmar metacarpal a. this
may influence the reliability of vascularized skin islands,
which are usually harvested to reconstruct soft tissue
defects of the thumb or index finger.
References
1. Adachi B (1928) Das Arteriensystem der Japaner, vol I. Maruzen, Kyoto, pp 375–423
2. Danenow NA (1973) Rare variant of the vessels of the upper extremity (Englishabstract). ArkhAnat Histol Embriol 64:77– 78
3. Gonzales-Compta X (1991) Origin of the radial artery from the axillary and associated hand vascular anomalies. J Hand Surg [Am] 16:293–296
4. Ikeda A, Ugawa A, Kazihara Y, Hamada N (1988) Arterial patterns in the hand based on a three-dimensional analysis of 220 cadaver hands. J Hand Surg [Am] 13:501–509
5. Kanbayashi T, Takafuji T, Sato Y (1993) On the arterial supply in the human biceps brachii muscle. Folia Anat Jpn 69:289–310 6. Karlsson S, Niechajev IA (1982) Arterial anatomy of the upper
extremity. Acta Radiol Diagn 23:363–373
7. Maral T, C¸elik H, Hayran M, Kec¸ik A (1993) An anatomical variation of the thoracodorsal artery with comments on flaps based on the axillary artery. Eur J Plast Surg 16:231–233 8. McCormack LJ, Cauldwel MD, Anson BJ (1953) Brachial and
antebrachial arterial patterns: a study of 750 extremities. Surg Gynecol Obstet 96:43–45
9. Pestemalci T, Kahraman G, Yildiz Z, Yildirim M (1999) Common trunk variation of arteria subscapularis and arteria circumflexa humeri posterior with early origin. J Morphol 7:64-65
10. Poteat WL (1986) Report of a rare human variation: absence of the radial artery. Anat Rec 214:89–95
11. Quain R (1844) The anatomy of the arteries of the human body. Taylor & Walton, London, p 273
12. Terminologia anatomica. International anatomical terminology (1998) Thieme, Stuttgart
13. Tiedeman F (1831) Plates of arteries of human body. McLachlan & Stewart, Edinburgh
14. Uglietta JP, Kadir S (1989) Arteriographic study of variant arterial anatomy of the upper extremities. Cardiovasc Intervent Radiol 12:145–148
15. Weathersby HT (1956) Unusual variation of the arterial pattern of the human upper limb. Anat Rec 124:245–248
16. Williams PL, Bannister LH, Berry MM, et al (1995) Gray’s anatomy, 38th edn. Churchill-Livingstone, Edinburgh, pp 319– 320
17. Yu¨cel AH (1999) Unilateral variation of the arterial pattern of the human upper extremity with a muscle variation of the hand. Acta Med Okayama 53:61–65