A new, objective radiographic classification system for the
assessment of treatment results in developmental dysplasia
of the hip
Hakan O
¨ merog˘lu
a, D. Hakan Uc¸ar
band Yu¨cel Tu¨mer
cThe new, objective radiographic classification system for the assessment of treatment results in developmental dysplasia of the hip includes three quantitative parameters: centre–edge angle of Wiberg, acetabular angle of Sharp and the centre–trochanter distance. Each parameter is divided into three subgroups and assigned a point score (0, 1 and 2) according to their previously determined values. Besides this, three corrective items on the existence of middle/posterior acetabular deficiency, secondary operation and resubluxation/redislocation are added to the classification system and in the presence of any of these items, one point for each item is extracted from the total points. A total of five or six points represents a satisfactory outcome and less than five points, an unsatisfactory outcome. The new system was found to have adequate intraobserver and interobserver agreement levels. It was also observed that, the gold standard Severin system could lead the raters to obtain somewhat more optimistic results with respect to the new system before and after skeletal maturity. It was concluded that the present system could evaluate both the final radiographic
status of the hip and the success or failure of the primary treatment and could be capable of leading orthopaedic surgeons to speak the same language while assessing radiographic results in developmental dysplasia of the hip. J Pediatr Orthop B 15:77–82 c 2006 Lippincott Williams & Wilkins.
Journal of Pediatric Orthopaedics B2006, 15:77–82
Keywords: developmental dysplasia of the hip, pelvic radiography, classification, treatment result
a
Department of Orthopaedics and Traumatology, Faculty of Medicine, Eski ¸sehir Osmangazi University, Eski ¸sehir,bClinics of Orthopaedics and Traumatology, Mesa Hospital andcDepartment of Orthopaedics and Traumatology, Faculty of Medicine, Ufuk University, Ankara, Turkey
Correspondence and requests for reprints to Professor Dr Hakan O¨ merog˘lu, Eski ¸sehir Osmangazi University Hospital, Department of Orthopaedics and Traumatology, 26480 Eski ¸sehir, Turkey
Tel: + 90 532 317 5352; fax: + 90 312 418 6494; e-mail: [email protected]
Sponsorship: None of the authors received any financial support for this study.
Introduction
A lot of studies have dealt with the treatment results in developmental dysplasia of the hip (DDH) for many years. To date, several clinical and radiological classifica-tion systems have been developed for the assessment of the results of several treatment procedures in DDH [1] and the Severin radiographic classification system [2] is widely accepted and the most frequently used for this purpose. The Severin system has several subjective parameters which include the description of the radi-ological appearance of the hip joint and an objective parameter, the centre–edge angle of Wiberg (CEA) (Table 1) [3]. Some controversy has arisen, however, on its reliability and reproducibility after publication of two recent articles [4,5]. Based on the findings of these studies, a need for construction of a more precise system for the classification of the radiographic results of several treatment procedures in DDH has occurred. The aim of the present study was to introduce a new, objective radiographic classification system for the assessment of the treatment results in DDH and to assess its use by both analysing its intraobserver and interobserver
agree-ment levels and comparing it with the Severin classifica-tion system, which is still considered the ‘gold standard’.
Patients and methods
Definition of the new systemThe new radiographic classification system can be used in patients of 5 years of age or older. It includes three quantitative radiographic parameters: CEA [3] is used for the assessment of lateral femoral head coverage by the acetabulum in the frontal plane (Fig. 1), the acetabular angle of Sharp (AA) [6] for the assessment of the acetabular slope in the frontal plane (Fig. 2) and the centre–trochanter distance (CTD) [7] for the assessment of the proximal femoral anatomy (Fig. 3). Each parameter is divided into three subgroups and assigned point scores: scoring – no points, severely pathologic; one point, slightly/ moderately pathologic; and two points, normal – according to their previously determined values in skeletally immature and mature hips (Figs 1–3) [1,3, 6–10]. A hip was considered skeletally mature if the proximal femoral epiphyseal growth line, greater trochan-teric apophyseal growth line and acetabular triradiate cartilage were not visible on the radiograph. If one or more of these mentioned items were visible on the radiograph, then the hip was considered skeletally immature.
A part of this study was presented as a poster at the 24th EPOS Meeting, Palma de Mallorca, Spain, 6–9 April 2005 and 7th EFORT Congress, Lisbon, Portugal, 4–7 June 2005.
There are three corrective items in the classification system and in the presence of any of these items one point for each item is subtracted from the total points.
The first minus point is given if the acetabulum is considered a type-4 acetabulum according to Ogata et al. [11], in which there is a considerable distance between the most lateral point of subchondral sclerosis and the most lateral point of the acetabular roof and the subchondral sclerosis is ill-defined and irregular. A second minus point is given if a secondary operation (pelvic or proximal femoral osteotomy or open reduction) has been performed. A third minus point is given if an early redislocation or resubluxation has occurred following primary treatment. A total of six points represents an ‘excellent outcome’, five points a ‘good outcome’, four points a ‘fair-plus outcome’, three points a ‘fair-minus outcome’ and less than three points a ‘poor outcome’. The outcome can be considered ‘satisfactory’ in those hips scoring five or six points and ‘unsatisfactory’ in those scoring under five points.
Assessment of the use of the new system
Two standard anteroposterior (AP) pelvic follow-up radiographs (after and before skeletal maturity) of 29 Table 1 Severin radiographic classification system
Group Charaecteristics
1 Normal hips
1a CEA > 191 (6–13 years), CEA > 251 ( Z 14 years) 1b 151r CEA r 191 (6–13 years), 201 r CEA r 251
( Z 14 years)
2 Moderate deformity of the femoral head or neck or acetabulum, but otherwise normal conditions in the joint
2a CEA > 191 (6–13 years), CEA > 251 ( Z 14 years) 2b 151r CEA r 191 (6–13 years), 201 r CEA r 251
( Z 14 years)
3 Dysplastic hips without subluxation, Shenton line is not broken CEA < 151 (6–13 years), CEA < 201 ( Z 14 years)
4 Subluxation, Shenton line is broken
4a CEA Z 01
4b CEA < 01
5 The head articulates with the false acetabulum in the upper part of the original acetabulum
6 Redislocation
CEA, centre–edge angle of Wiberg. Modified from Severin [2].
Fig. 1
Mature hip ≥20° (2), 5°−19° (1), <5° (0)
Immature hip (≥5 years) ≥15° (2), 0°−14° (1), <0° (0)
CEA (°) C E
The centre–edge angle of Wiberg (CEA) [3] is measured between the line starting from the centre of the femoral head (C) and parallel to the longitudinal body axis and the line between the C point and the most lateral point of the acetabular roof (E). The scoring system for CEA is mentioned below the drawing.
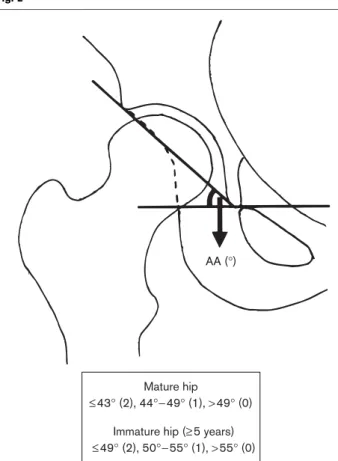
Fig. 2
Mature hip
≤43° (2), 44°−49° (1), >49° (0) Immature hip (≥5 years) ≤49° (2), 50°−55° (1), >55° (0)
AA (°)
The acetabular angle of Sharp (AA) [6] is formed by a horizontal line connecting the tips of the both pelvic teardrops and by a line connecting the inferior tip of the pelvic teardrop with the most lateral point of the acetabular roof. The scoring system for AA is mentioned below the drawing.
patients (43 hips) who were initially treated by the senior author (Y.T.) due to DDH by the posteromedial approach open reduction [12] were included the study. Mean age of the patients at operation was 11 months (range 2–19 months), at the mid-term follow-up (skeletally imma-ture) was 9 years (range 5–12 years) and at the latest follow-up (skeletally mature) was 21 years, (range 13–29 years).
The first step of the study included the assessment of the intraobserver and interobserver agreement levels of the new system. For this purpose, the first two authors (H.O¨. and D.H.U.) who were not involved in the treatment of the patients, independently assessed twice, the radio-graphs of the skeletally immature hips, 3 weeks apart. Three months later, they independently assessed twice, the radiographs of the same hips, obtained after skeletal
maturity, 3 weeks apart. After measuring the CEA, AA and CTD, two radiographic results for each hip were drawn. The first one included the exact classification of the results according to the new system as excellent, good, fair-plus, fair-minus or poor. The second one included the classification of the results as satisfactory (5 or 6 points) or unsatisfactory (less than 5 points). The same pencil and goniometer was used in all measurements. Each rater did not know how the other rated the radiographs. The second step of the study included the comparison of the Severin and new systems using the same hip radiographs. Mean values of two observers’ total four measurements of each parameter in each hip was considered as the ‘definitive value’. After the determina-tion of the definitive values of each radiographic para-meter in each hip, the hips were classified according to the Severin and the new classification systems according to these definitive values by the first two authors, concomittantly.
The k coefficient [13] was used to evaluate the intraobserver and interobserver agreements. The level of agreement was assessed by the classification system in which a k coefficient of 0–0.20 indicated poor agreement, 0.21–0.40, fair agreement, 0.41–0.60, moderate agree-ment, 0.61–0.80 substantial agreement and 0.81–1.0, excellent agreement [14]. The w2test and the Fisher’s exact test were used for comparison of the two systems and a P value less than 0.05 was considered significant.
Results
Mean intraobserver agreement level on exact hip typing was substantial in both skeletally immature and mature hips and the obtained interobserver agreement level on exact hip typing was moderate in both skeletally immature and mature hips (Table 2). When the radio-graphic outcomes of the hips were classified as satisfac-tory or unsatisfacsatisfac-tory, mean intraobserver agreement level was excellent in both skeletally immature and mature hips and the obtained interobserver agreement level was moderate in skeletally immature hips and substantial in mature hips (Table 2).
Before skeletal maturity, 41 hips (95%) were considered to have a satisfactory outcome (group 1 and 2) according to the Severin system and 36 hips (84%) were considered to have a satisfactory outcome (excellent or good) according to the new system (Table 3). There was no significant statistical difference between the mentioned outcome ratios of two classification systems (P = 0.156). Prior to the mid-term follow-up examination, 10 hips (23%) already underwent a secondary operation (iliac or proximal femoral osteotomy) due to acetabular or proximal femoral dysplasia. After skeletal maturity, 36 hips (84%) were considered to have a satisfactory Fig. 3 −11 to +1 mm −12 to −17 & +2 to +7 mm <−17 & >+7 mm 0 to +10 mm −1 to −5 & +11 to +15 mm <−5 & >+15 mm (2) (1) (0) (2) (1) (0) T CTD (mm) C Mature hip
Immature hip (≥5 years)
The centre–trochanter distance (CTD) [7] is measured in millimetres between two parallel lines which are perpendicular to the femoral shaft axis and pass through the centre of the femoral head (C) and the tip of the greater trochanter (T), respectively. CTD is expressed as a positive or a negative value if the C point is superior or inferior to the T point, respectively. The scoring system for CTD is mentioned below the drawing.
outcome (group 1 and 2) according to the Severin system and 29 hips (67%) were considered to have a satisfactory outcome (excellent or good) according to the new system (Table 4). No significant statistical difference was found between the mentioned outcome ratios of two classifica-tion systems (P = 0.079). At the latest follow-up the rate of secondary operation was 28% (12 hips).
Discussion
An AP pelvic radiograph still plays an important role both in the decision of treatment modality and assessment of the treatment outcome in DDH. These are often based on different radiographic measurements and scores. None of the previously defined radiographic classification or scoring systems for the assessment of the treatment
results in DDH, however, seems to lead orthopaedic surgeons to speaking the same language exactly.
We believe that the current system is superior with respect to the gold standard Severin system in three main ways: firstly, a classification system can be considered valid and reliable if its accuracy and reproducibility are exactly demonstrated [5]. Although widely used, the Severin system has been shown to have an unacceptable level of observer agreement that may limit its use. The main reason for this situation seems to be the lack of universal agreement on the definitions of the terms such as moderate deformity, dysplasia and subluxation used in the Severin system [4,5]. Also, the parameter ‘continuty of the Shenton line’ may have a considerable level of Table 2 Assessment of the observer agreement in two age groups
Observer agreement ratios (k coefficient)
Intraobserver Interobserver
Observer 1 Observer 2
Skeletally immature hips (mean age 9 years)
Exact hip typing 81% (0.73) 72% (0.58) 62% (0.42)
Hip typing as satisfactory or unsatisfactory outcome
98% (0.94) 95% (0.85) 85% (0.55)
Skeletally mature hips (mean age 21 years)
Exact hip typing 72% (0.62) 93% (0.90) 66% (0.53)
Hip typing as satisfactory or unsatisfactory outcome
91% (0.80) 95% (0.89) 88% (0.73)
Table 3 Radiographic results of the skeletally immature hips according to the Severin and new classification systems
New system Total (Severin)
Excellent Good Fair-plus Fair-minus
Severin system
Group 1 24 (a) 6 (a) 31
0 (b) 1 (b)
Group 2 5 (a) 2 (a) 1 (a) 10
0 (b) 1 (b) 1 (b)
Group 3 2 2
Total (new system) 24 12 5 2 43
The letters in parentheses represent the subgroup (a or b) of the Severin hip typing.
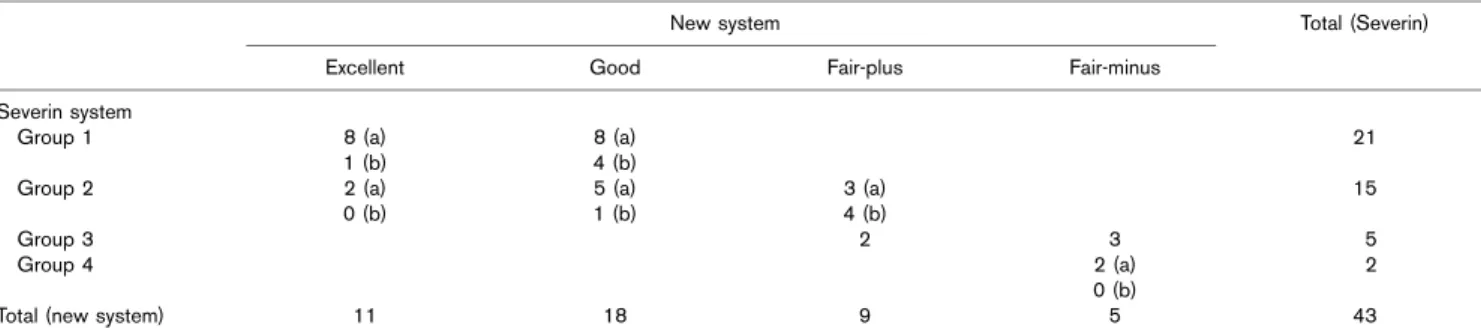
Table 4 Radiographic results of the skeletally mature hips according to the Severin and new classification systems
New system Total (Severin)
Excellent Good Fair-plus Fair-minus
Severin system
Group 1 8 (a) 8 (a) 21
1 (b) 4 (b)
Group 2 2 (a) 5 (a) 3 (a) 15
0 (b) 1 (b) 4 (b)
Group 3 2 3 5
Group 4 2 (a) 2
0 (b)
Total (new system) 11 18 9 5 43
observer disagreement. The new system includes only quantitative parameters and we believe that this is the main reason for having acceptable levels of observer agreement in different age groups. Besides this, all the radiographic parameters used in the new system (CEA, AA, CTD and acetabular typing) have previously been shown to have adequate levels of intraobserver and interobserver agreements, in different age groups [7,15– 19]. Second, the CEA is the single quantitative aspect of the Severin system. It is a useful index for the assessment of the lateral femoral head coverage by the acetabulum but not for the acetabular slope and proximal femoral anotomy, which are also disrupted in DDH. These parameters may not correlate well with each other in the dysplastic hips. For example, a hip joint with a severe proximal femoral deformity due to trochanteric over-growth may have a CEA in normal limits, but one should not consider the radiographic result as satisfactory after measuring only the CEA. On the other hand, the new system includes three quantitative radiographic para-meters: AA and CTD besides CEA. AA and CTD define the acetabular and proximal femoral anatomies in an objective manner, respectively. The severity of acetabular dysplasia can easily be classified according to the previously determined values of AA [1,6,9]. A significant decrease in the CTD is mainly due to the relative overgrowth of the greater trochanter, decreased neck– shaft angle or decreased femoral neck length. On the other hand, a significant increase is mainly due to increased neck–shaft angle or antetorsion of the femoral neck [7]. Finally, the Severin system evaluates the final status of the hip joint not the success or failure of the primary treatment. For example, although the rate of secondary operation in the present series is more than 20%, the rate of unsatisfactory radiographic results according to the Severin system is less than 20% before and after skeletal maturity. The new system, however, evaluates both the final radiographic status of the hip joint and the success or failure of the primary treatment by taking into account the complications. This situation may be considered another advantage of the new system. On the other hand, it may be thought that the final result is important rather than the number of operations required to achieve it.
In the new system, congruity of the femoral head is not scored as it is considered to be a subjective entity. This system is also not capable of predicting degenerative osteoarthritis, which is an important late complication. The reasons for the addition of three corrective items to the new classification system after completing the radiographic measurements are as follows: in a hip with type-4 acetabulum according to Ogata et al. [11], CEA and AA cannot exactly verify the radiographic femoral head coverage and acetabular anatomy as in such hips mid/ posterior acetabular deficiency exists and the
radio-graphic measurements can be optimistic if the most lateral point of the acetabular roof is used as the reference point [11,15,19,20]. Also, following a secondary operation, the obtained radiographic measurements can reflect the outcome of the secondary treatment rather than the one of the primary treatment. Finally, if an early redislocation or resubluxation has occurred following primary treat-ment, it should always be taken into consideration while assessing the outcome, even if treated properly.
As the centre of the femoral head on a plain radiograph cannot be accurately defined due to eccentric localization of the ossific nucleus under 5 years of age [1], the use of two parameters of the new system; CEA and CTD is limited in that age group and we do not recommend the use of this system in children under 5 years of age. There are two additional findings of the present study which should be emphasized. Raters can obtain slightly more optimistic results by using the Severin system with respect to the new system, in the same hips, before and after skeletal maturity. This difference seems to be mainly due to the existence of the corrective items in the new classification system. All of the ‘excellent’ and ‘good’ rated hips according to the new system were also considered Severin group 1 or 2, before and after skeletal maturity. All of the Severin group 3 and 4 rated hips were also rated as ‘fair’ according to the new system, before and after skeletal maturity. A significant incompatibility between two systems was seen in Severin group 2 rated hips. Five of seven and seven of 14 ‘fair’ rated hips in the new system before and after skeletal maturity, respec-tively, were rated as Severin group 2. This finding may draw two possible conclusions about Severin group 2 rated hips. The first is that all Severin group 2 hips may not always have a successful primary treatment and the second that the moderate deformity of the proximal femur or acetabulum stated in Severin group 2 cannot always be accepted as a satisfactory radiographic result in DDH. The radiographic results of the same hips are considerably different between two different follow-up periods (before and after skeletal maturity). Better radiographic results have been obtained before skeletal maturity, by using both of the classification systems. This finding again reveals that the exact comments on the radiographic results of DDH can only be made after skeletal maturity.
We can conclude that the new system has the ability to evaluate both the final radiographic status of the hip joint and the success or failure of the primary treatment. Besides this, the new system seems to be capable of leading orthopaedic surgeons to speak the same language while assessing the radiographic results of the different treatment procedures in DDH before and after skeletal maturity.
References
1 Tonnis D. Congenital dysplasia and dislocation of the hip in children and adults. Berlin Heidelberg: Springer-Verlag; 1987.
2 Severin E. Contribution to the knowledge of congenital dislocation of the hip; late results of closed reduction and arthrographic studies of recent cases. Acta Chir Scand 1941; 84 (Suppl 63):1–142.
3 Wiberg G. Studies on dysplastic acetabula and congenital subluxation of the hip joint; with special reference to the complication of osteoarthritis. Acta Chir Scand 1939; 83 (Suppl 58):1–135.
4 Ali AM, Angliss R, Fujii G, Smith DM, Benson MKD. Reliability of the Severin classification in the assessment of developmental dysplasia of the hip. J Pediatr Orthop B 2001; 10:293–297.
5 Ward WT, Vogt M, Grudziak JS, Tu¨mer Y, Cook PC, Fitch RD. Severin classification system for evaluation of the results of operative treatment of congenital dislocation of the hip; A study of intraobserver and interobserver reliability. J Bone Joint Surg Am 1997; 79A:656–663.
6 Sharp IK. Acetabular dysplasia. The acetabular angle. J Bone Joint Surg Br 1961; 43B:268–272.
7 O¨ meroglu H, Uc¸ar DH, Tu¨mer Y. A new measurement method for the radiographic assessment of the proximal femur; the center-trochanter distance [in Turkish]. Acta Orthop Traumatol Turc 2004; 38:261–264. 8 Fredensborg N. The CE angle of normal hips. Acta Orthop Scand 1976;
47:403–405.
9 O¨ zc¸elik A, O¨meroglu H, Inan U, O¨zyurt B, Seber S. Normal values of several acetabular angles on hip radiographs obtained from individuals living in the Eskisehir region [in Turkish]. Acta Orthop Traumatol Turc 2002; 36:100–105. 10 O¨ zc¸elik A, O¨meroglu H, Inan U, Seber S. Center-edge angle values in
normal hips of children and adults in Turkish population [in Turkish]. J Arthroplasty Arthroscopic Surg 2001; 12:115–119.
11 Ogata S, Moriya H, Tsuchiya K, Akita T, Kamegaya M, Someya M. Acetabular cover in congenital dislocation of the hip. J Bone Joint Surg Br 1990; 72:190–196.
12 Ferguson AB Jr. Primary open reduction of congenital dislocation of the hip using a median adductor approach. J Bone Joint Surg Am 1973; 55: 671–689.
13 Cohen JA. A coefficient of agreement for nominal scales. Educat Psychol Measure 1960; 20:37–46.
14 Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics 1977; 33:159–174.
15 Agus H, Bic¸imoglu A, O¨ meroglu H, Tu¨mer Y. How should the acetabular angle of Sharp be measured on a pelvic radiograph? J Pediatr Orthop 2002; 22:228–231.
16 Broughton NS, Brougham DI, Cole WG, Menelaus MB. Reliability of radiological measurements in the assessment of the child’s hip. J Bone Joint Surg Br 1989; 71B:6–8.
17 Nelitz M, Guenther KP, Gunkel S, Puhl W. Reliability of radiological measurements in the assessment of hip dysplasia in adults. Br J Radiol 1999; 72:331–334.
18 O¨ meroglu H, Agus H, Bic¸imoglu A, Tu¨mer Y. Analysis of a radiographic assessment method of acetabular cover in developmental dysplasia of the hip. Arch Orthop Trauma Surg 2002; 122:334–337.
19 O¨ meroglu H, Bic¸imoglu A, Agus H, Tu¨mer Y. Measurement of center-edge angle in developmental dysplasia of the hip: a comparison of two methods in patients under 20 years of age. Skeletal Radiol 2002; 31: 25–29.
20 Kim HT, Kim JI, Yoo CI. Diagnosing childhood acetabular dyaplasia using the lateral margin of the sourcil. J Pediatr Orthop 2000; 20: