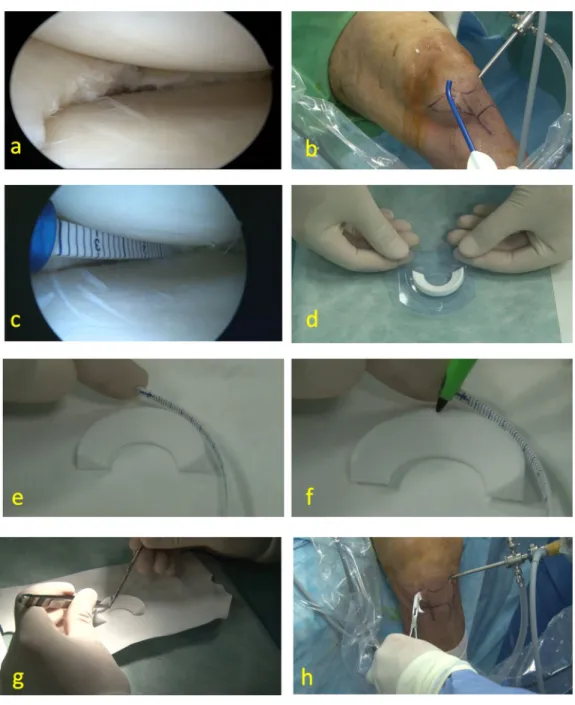
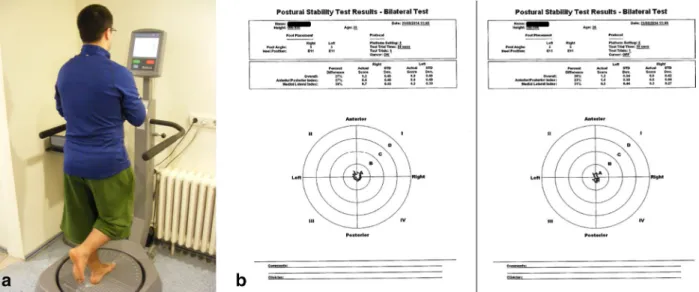
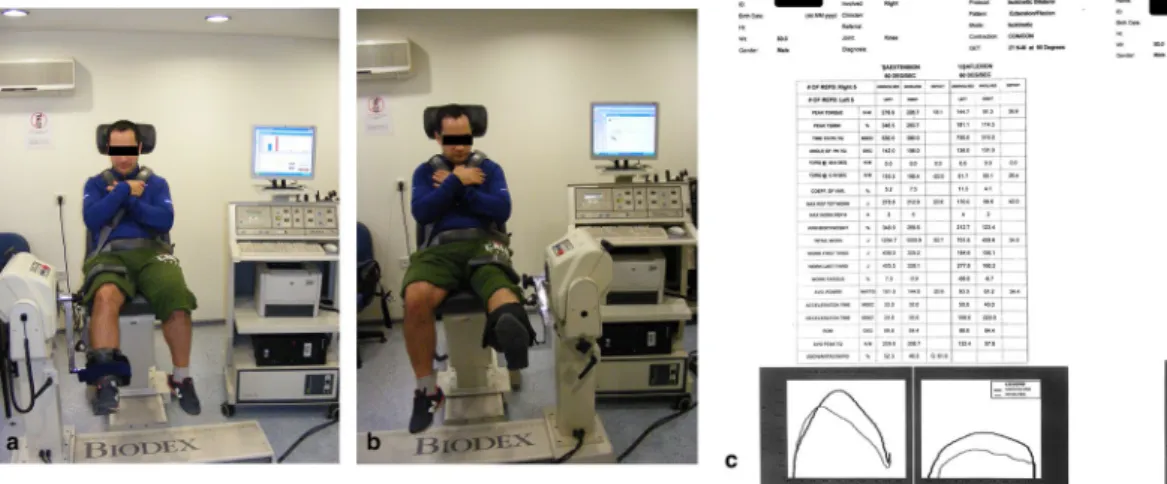
Muscle strength but not balance improves after arthroscopic biodegradable polyurethane meniscus scaffold application
Tam metin
Şekil
Benzer Belgeler
elemanlarında Ģu değiĢimler olur. i) Pozitif plakalar, kurĢun peroksitten, kurĢun sulfata dönüĢür. ii) Negatif plakalar, sünger kurĢundan, kurĢun sulfata dönüĢür.
In the first step, they have collected data of the students, which can be used for matching the face detection result. As a part of the image acquisition, the high definition
Atılması planlanan tüm adımların Fakültemizde eğitim ile ilgili dört kurulumuz olan Eğitim Öğretim Koordinasyon Kurulu (EÖKK), Program Geliştirme ve
Kronik obstrüktif akciğer hastalığı (KOAH) tüm dünyada morbidite ve mortalitenin en önemli sebebidir. Hastaların çoğu için KOAH’ın en son tedavisi semptomları
[r]
Bezmialem Vakıf Üniversitesi Dahili Yoğun Bakım ünitesinde 25 Ekim 2010 ile 30 Nisan 2011 tarihleri arasında yoğun bakım ünitemizde 24 saatten fazla yatmış olan
Büyü ve büyücülüğün mahiyeti ve bu eylemin fıkhî hükümleriyle ilgili temel bilgilerin akabinde çalışmamızın temel problematiği olan büyücülüğün ceza hukuku yönü
Bu çalışmada Türk Gıda Kodeksi’nde özel tıbbi amaçlı diyet gıdalar altında yer alan enteral bes- lenme ürünlerinin Mezofilik Aerobik Bakteri ve C.sakazakii
