Original Article
Gynecol Obstet Invest 2012;73:99–105 DOI: 10.1159/000328447
Effects of Percutaneous Tibial Nerve
Stimulation Therapy on Chronic Pelvic
Pain
Sule Gokyildiz
a
Nezihe Kizilkaya Beji
b
Onay Yalcin
c
Ayse Istek
d
a Cukurova University Adana Health High School, Adana , and b Faculty of Nursing, c Istanbul Faculty of Medicine, Istanbul University, Istanbul , and dHospital of Genc Devlet, Bingol , Turkey
Introduction
Chronic pelvic pain (CPP) is a common problem with a high impact on patients’ quality of life. As its etiology and pathophysiology are mostly unknown, treatment is often empirical and polypragmatic. Neuromodulation has been reported to reduce pelvic pain by means of sacral nerve stimulation, while there are also reports on positive effects of neuromodulation in pain complaints accompa-nying conditions like interstitial cystitis. Percutaneous tibial nerve stimulation (PTNS) has been shown to be an effective therapeutic option for patients with lower uri-nary tract dysfunction, e.g. urge incontinence, urgency/ frequency, nonobstructive retention. Only a few studies have been carried out concerning this minimally invasive treatment option for CPP [1–3] .
Studies on tibial nerve stimulation (TNS) conducted in our country were on overactive detrusor cases [4–7] , but none were about CPP. This is the first study concern-ing women with CPP and havconcern-ing experimental and con-trol groups.
This study aims to identify the effect of TNS treatment on patients’ quality of life and sexual life.
Key Words
Chronic pelvic pain ⴢ Neuromodulation ⴢ Quality of life ⴢ Sexual function ⴢ Tibial nerve stimulation
Abstract
Objective: This research is a prospective study which was designed to determine the effects of percutaneous tibial nerve stimulation (PTNS) therapy on the quality of life and sexual life of patients with chronic pelvic pain (CPP).
Meth-ods: The sample consisted of an experimental group (n = 12)
and a control group (n = 12), in total 24 patients. The experi-mental group was treated with PTNS once a week (in total 12 sessions), while the control group received routine interven-tion. Results: The pain frequency and intensity in women who underwent PTNS decreased considerably. Women had less pain during sexual intercourse after PTNS. We deter-mined in our study that PTNS improved the quality of life of women with CPP by decreasing the intensity of pain and contributed to a more comfortable performance of their dai-ly activities. Conclusions: PTNS is a type of treatment which contributes to the quality of life of women with CPP by de-creasing the intensity of pain. Copyright © 2012 S. Karger AG, Basel
Received: July 5, 2010
Accepted after revision: April 13, 2011 Published online: January 20, 2012
Method
This is an experimental research study aiming to identify the effect of TNS treatment on patients’ quality of life and sexual life. In order to determine the cases to be used in the research, 8,872 gynecology patient records in the year 2006, 10,427 in the year 2007 and 500 in the year 2008 were reviewed at Istanbul Medical School Department of Obstetrics and Gynecology, Istanbul Uni-versity. Sixty-five patients who had pain in the pelvis/lower abdo-men (http://www.tureng.com/search/hypogastric+region) for at least 6 months were identified and these patients were called and asked whether they still had pain. Those who still did were in-vited to the Urogynecology Unit and 52 patients applied to the unit. A flowchart is displayed in figure 1 . Before beginning the study, it was approved by the Ethics Committee of Istanbul Uni-versity.
Of the women with CPP 26 met the inclusion criteria. The women who came to the Urogynecology Unit were randomized using envelopes. As a result, 12 subjects were included in the ex-perimental group and 12 in the control group. All the patients were evaluated through CPP history, physical examination, gyne-cological examination and ultrasound, and no statistically sig-nificant difference was detected between the experimental and control groups.
Inclusion Criteria • Diagnosis of CPP • Voluntary participation
• Pain score 1 5 according to the visual analogue scale (VAS) • Cessation of analgesic at least 2 weeks before PTNS treatment • Cessation of physiotherapy or electrotherapy at least 3 months
before PTNS treatment Exclusion Criteria
• Pregnancy or planning a pregnancy • Heart disease or cardiac pacing • Nerve damage
• Use of anticoagulant medicine
• Active or recurrent urinary tract infection (more than five in last 12 months)
Procedure
PTNS was applied according to Stoller [8] and Govier et al. [9] using a neuromodulation system composing a needle set and a stimulator that runs with a 9-volt battery and creates an adjustable current between 0.5 and 10 mA, 200 s and 20 Hz frequency. The patients lay on their backs in a supine position with the knees ab-ducted and flexed (frog position). The 34-gauge needle was in-serted approximately 3–4 cm above the inner malleolus, by
enter-Population – women referring to gynecology department (n = 19,799)
Women having pain in pelvis and lower abdomen for at least 6 months (n = 65)
Not appropriate for the research criteria (n = 26) Met (n = 52)
Appropriate for the research criteria (n = 26)
Having PTNS treatment (n =13)
Randomized
Not having PTNS treatment (n = 13)
Improvement in complaints (n = 17) Treatment
Surgical operation (n = 3) VAS below 5 (n = 2) Deep vein thrombosis (n = 1) Crohn‘s disease (n = 1) Pregnant (n = 2) Experimental (n = 13)
Monitoring in the 1st week PTNS for 12 sessions Monitoring in the 12th week Dropped (n = 1)
Control (n = 13)
Monitoring in the 1st week Monitoring in the 12th week Dropped (n = 1)
Not met (n = 13)
(could not be reached from the communication information given)
ing at the place appropriate to the posterior tibial nerve line with a 60° angle, the adhesive electrode was placed on the inner side of the heel and the set was connected to the stimulator. The stimula-tor was run and the current was adjusted according to the patient’s tolerance. When the current is flowing correctly, if the inserted needle is in the right place, toes should have plantar flexion (mov-ing downwards) and/or 2nd to 5th f(mov-ingers should release or have plantar flexion. The application continued for 12 weeks, each ses-sion lasting 30 min.
Data were collected through (1) a questionnaire to identify pa-tients’ socio-demographical and general state of health, (2) VAS at 0–10 range to determine pain intensity, (3) SF-36 quality of life scale to identify patients’ quality of life, (4) McGill pain questionnaire (MPQ) to identify the features of the pelvic pain and (5) female sexual function index (FSFI) to evaluate sexual functions. The SF-36 questionnaire consists of SF-36 items covering eight distinct health status concepts and one item measuring self-reported health tran-sition: physical function, role, emotional health, social functioning, energy/fatigue and change in general health. The scale was adapted to Turkish society by enhancing its reliability and validity in Pınar’s study with diabetics [10] . MPQ is composed of four sections and it has a multidimensional evaluation of pain. Kuguoglu et al. [11] en-hanced the validity and reliability of MPQ and translated the form to Turkish. As a result, the test was found to have a high internal reliability and sufficient construct validity. The FSFI, a 19-item questionnaire, has been developed as a brief, multidimensional self-report instrument for assessing the key dimensions of sexual function in women, which include desire, subjective arousal, lubri-cation, orgasm, satisfaction and pain [12] . The reliability and valid-ity of the adaptation of the scale into Turkish was enhanced by Ay-gin and Aslan [13] , and FSFI was determined to be valid and reliable in evaluating the sexual functions of Turkish women.
The forms were administered to the patients at the beginning of the research and at the end of the 12-week treatment.
The data obtained were calculated using SPSS (statistical pro-gram for social science) 11.5 for Windows and evaluated through frequency, mean, standard deviation, median, minimum and maximum, 2 , Fisher certain 2 , Wilcoxon rank and
Mann-Whit-ney U test [14] .
Results
In this research, there is no significant difference be-tween the women in the control and experimental groups in terms of age, education, occupation, financial situa-tion, pregnancy and number of births, health problems, pain duration, operations and drug usage.
Pain duration of the women was detected at 3.91 8 2.15 years (min. 1 year, max. 8 years) on average for the experimental group and at 3.95 8 2.26 years (min. 1 year, max. 7 years) for the control group.
Pain intensity of the women in the experimental group was 8.08 8 1.72 on average in VAS before PTNS and 2.62 8 2.70 on average after PTNS. As for the control group, the means were detected at 7.95 8 1.03 on average at the beginning and 7.87 8 0.88 afterwards ( fig. 2 ).
When the pain intensity of both groups was compared before and after the treatment, no statistically significant difference was detected between the experimental and
8.08 2.62 7.95 7.87 0 5 10 Experimental Control
Before treatment After treatment
Co lo r v e rs io n av a il a b le o n li n e
Fig. 2. Comparison of VAS scores.
Table 1. Findings of the McGill pain questionnaire
Pain dimension
Experimental, mean 8 SD Control, mean 8 SD Experimental
BT/AT1 Control FM/SM1 Experimental/control before treatment after treatment first meeting second meeting ZWK p ZWK p BT2 A T2 ZMWU p ZMW U p Sensory 20.8387.69 12.50812.07 23.1684.13 23.8383.85 –1.93 0.06 –1.23 0.21 –0.46 0.64 –2.20 0.02 Affective 7.1683.15 3.5084.29 7.4181.44 7.7581.21 –2.40 0.01 –1.63 0.10 –0.20 0.83 –2.56 0.01 Evaluation 2.9181.44 1.5881.88 3.0081.27 3.3381.23 –2.20 0.02 –1.41 0.15 –0.20 0.83 –2.30 0.02 Miscellaneous 8.4183.62 3.9184.27 10.2584.53 10.1684.42 –2.43 0.01 –1.00 0.31 –0.81 0.41 –2.87 0.004 PRI 39.33812.39 21.5821.04 43.8385.32 43.8385.32 –2.22 0.02 0.00 1.00 –0.49 0.62 –2.46 0.01 PPI 21.3384.09 15.0886.03 21.8382.48 22.5082.19 –3.07 0.02 –1.84 0.66 –0.03 0.97 –3.31 0.001
1 Wi lcoxon rank test. 2 Mann-Whitney U test. FM = First meeting; SM = second meeting; BT = before treatment; AT = after
control groups before the treatment, whereas the signifi-cance was quite high after PTNS. Pain intensity of the patients in the experimental group significantly de-creased (before treatment: Z MWU = –0.46, p = 0.72; after
treatment: Z MWU = –3.61, p = 0.00).
Table 1 shows the scores of replies given in relation to MPQ subscales. When the women in the experimental group were compared before and after treatment in terms of aspects related to pain, a significant decrease was de-tected after the treatment in all aspects except for sensory. No significant difference was found between the first and the second meeting conducted with the women in the control group. When both groups were compared in terms of pain aspects, no statistically significant differ-ence was found between the experimental and control
groups before the treatment whereas the experimental group showed a significant difference in all aspects, in the pain-rating index (PRI) and in the present pain intensity (PPI), after the treatment ( table 1 ).
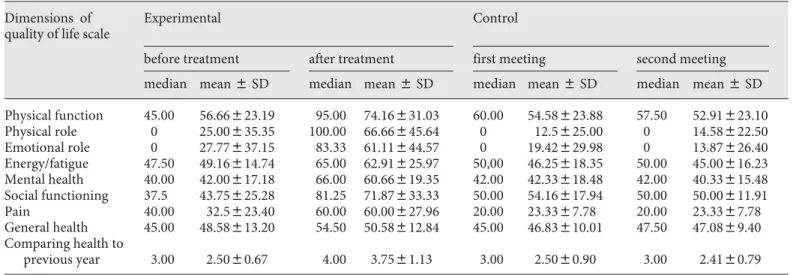
Average scores of women in the experimental and con-trol groups on SF-36 quality-of-life scale are displayed in table 2 . After PTNS, the women in the experimental group were found to have positive changes in physical functions, emotional functions, mental health, social functions and pain aspects and, when compared to the previous year, their state of health was found to be better than before PTNS and better than women in the control group ( table 2 ).
Sexual functions of women in this study were evalu-ated through FSFI sexual desire, stimulation, lubrication,
Table 2. Findings of the SF-36 quality of life scale Dimensions of
quality of life scale
Experimental C ontrol
before treatment after treatment first meeting second meeting
median mean 8 SD median mean 8 SD median mean 8 SD median mean 8 SD
Physical function 45.00 56.66823.19 95.00 74.16831.03 60.00 54.58823.88 57.50 52.91823.10 Physical role 0 25.00835.35 100.00 66.66845.64 0 12.5825.00 0 14.58822.50 Emotional role 0 27.77837.15 83.33 61.11844.57 0 19.42829.98 0 13.87826.40 Energy/fatigue 47.50 49.16814.74 65.00 62.91825.97 50,00 46.25818.35 50.00 45.00816.23 Mental health 40.00 42.00817.18 66.00 60.66819.35 42.00 42.33818.48 42.00 40.33815.48 Social functioning 37.5 43.75825.28 81.25 71.87833.33 50.00 54.16817.94 50.00 50.00811.91 Pain 40.00 32.5823.40 60.00 60.00827.96 20.00 23.3387.78 20.00 23.3387.78 General health 45.00 48.58813.20 54.50 50.58812.84 45.00 46.83810.01 47.50 47.0889.40 Comparing health to previous year 3.00 2.5080.67 4.00 3.7581.13 3.00 2.5080.90 3.00 2.4180.79
1 Wi lcoxon Rank test. 2 Mann Whitney U test. FM = First meeting; SM = second meeting; BT = before treatment; AT = after
treat-ment.
Table 3. Findings of FSFI pain and total scores
FSFI Experimental Control Experimental
BT/AT1 ControlFM/SM1 Experimental/control
before treatment after treatment first meeting second meeting ZWK p ZWK p BT2 AT2
me dian mean 8 SD median mean 8 SD median mean 8 SD median mean 8 SD ZMWU p ZMWU p
Pain 3.60 3.4581.55 5.20 4.6981.58 3.60 3.4680.68 3.60 3.2680.53 –2.25 0.02 –1.89 0.06 –0.15 0.87 –2.35 0.01
Total
FSFI 20.60 20.8786.76 23.80 23.0388.23 21.80 21.4785.87 21.75 20.9585.49 –0.80 0.42 –1.92 0.06 –0.36 0.71 –0.52 0.60
satisfaction, pain during sexual intercourse, and total FSFI scores. Before treatment, total FSFI scores of the women in the experimental group were 20.87 8 6.76 and the scores in the control group were 21.47 8 5.87. These are below 26.55, which is below FSFI approximation point. It was found that the women in the experimental group had significant difference only in the FSFI pain subscale. Women had less pain during sexual intercourse after PTNS. Although there is an increase in FSFI total score after PTNS, this increase is not statistically signifi-cant ( table 3 ).
During PTNS, 2 patients had slight pain in the 3rd ses-sion, 1 patient had slight pain in the 8th and 10th sessions and 1 patient had hematoma, and in the 12th session 1 patient had slight pain. No other complications were de-tected in other sessions.
Discussion
CPP is one of the most important reasons for many women during their reproductive age to consult a gyne-cologist [1] . Research conducted by Zondervan et al. [15] shows that when all diseases common among women be-tween the ages of 15 and 73 are taken into account, with a 3.8% proportion, CPP is even more frequent than mi-graine (2.1%) and asthma (3.7%).
The first study to identify the effect of PTNS in pa-tients with CPP as their main complaint was conducted
by Van Balken et al. [2] and studies about this are limited. Literature reviews show that there are no studies con-ducted in our country.
In this research, there is no significant difference be-tween the control and experimental groups in terms of age, education, occupation, financial situation, pregnan-cy and number of births, health problems, pain duration, operations and drug usage. This similarity between the groups enhances the reliability of the data obtained in this study.
Pain intensity of the women in the experimental group according to VAS was 8.08 8 1.72 before PTNS and 2.62 8 2.70 after PTNS, and pain intensity of the women in the control group was 7.95 8 1.03 on average at the first meeting and 7.87 8 0.88 at the second meeting. Unlike the studies of Van Balken et al. [2] (VAS 6.5, range = 5.3– 7.7 before PTNS; VAS 5.4, range = 4.2–6.8 after PTNS) and Kim et al. [3] (VAS 8.1 8 0.2 on average before PTNS and 4.1 8 0.6 after PTNS), our study involves only female patients and experimental/control groups, but the results obtained from our study share similarity. Pain intensity was decreased significantly in the experimental group af-ter PTNS.
Van Balken et al. [2] evaluated the number of words chosen score and PRI in MPQ. Except for PRI, no sig-nificant difference was detected at the end of the 12-week treatment, and total PRI decreased from 21.5 to 17.2 (p ! 0.05).
Unlike the study of Van Balken et al. [2] , we evaluated PPI sections in addition to the chosen words in MPQ, sensory and affective, evaluative, ‘others’ and total PRI scores ( table 1 ). The women in the experimental group reported a decrease in pelvic pain frequency and inten-sity after PTNS.
Studies show that daily activities of most women with CPP are affected by the tension caused by pain and their quality of life decreases significantly [16–18] . In their community-based study conducted in England, Zonder-van et al. [19] found that approximately 70% of the wom-en reported moderate or severe pain, 58% stated that the pain limited their activities, 8.7% said they could not do any activities without taking analgesic or relaxing. They also stated that they had to limit their housework (6.6%), social activities (6.2%) and movements (walking and moving) (6.4%). 1.9% had difficulty in concentrating, and 33% reported that they could not go to work for at least 1 day in the last 12 months. In their research with 1,160 women, Grace and Zondervan [18] found that CPP had negative effects on women’s general state of health. It was found that patients with CPP had more sleeping
Experimen-tal BT/AT1 Control FM/SM1 Experimental/control
ZWK p ZWK p BT2 AT2 ZMWU p Z MWU p –1,61 0.10 –1.63 0.102 –0.26 0.79 –1.68 0.09 –2,10 0.03 –0.57 0.56 –0.93 0.35 –2.62 0.009 –2,13 0.03 –1.00 0.31 –0.53 0.59 –2.71 0.007 –1,33 0.18 –1.00 0.31 –0.17 0.86 –1.94 0.06 –3,07 0.002 –1.63 0.10 –0.06 0.95 –2.54 0.01 –2,19 0.03 0.00 1.00 –1.14 0.25 –2.71 0.04 –2,27 0.02 0.00 1.00 –0.94 0.34 –3.31 0.001 –0,67 0.50 0.00 1.00 –0.26 0.79 –1.13 0.25 –2.71 0.007 –1.00 0.31 –0.06 0.94 –2.68 0.007
problems, the pain affected their activities (52.7%), they were unable to do any activities without taking analgesic (12.2%) and they had to limit their movements (walking and moving) (14.3%). Zondervan et al. [19] and Grace and Zondervan [18] evaluated the SF quality-of-life scale as physical health components (physical component summary) and mental health components (mental com-ponent summary). Physical comcom-ponent summary scores were 48.2 8 11 and 47.3 8 9.2, respectively, on average and mental component summary scores 44.4 8 11.5 and 45.2 8 12, respectively. Van Balken et al. [2] found that women’s SF-36 quality-of-life scale had significant changes in physical functions, physical roles, pain and general health aspects. This study revealed that women in the experimental group had positive improvements in physical function, emotional function, mental health, social function and pain aspects after PTNS, and the present state of health of women in the experimental group, when compared to their health in the previous year, was found to be better than before PTNS and also better than women in the control group ( table 2 ). Wom-en’s quality of life improved after PTNS. It can be seen that PTNS improves quality of life positively by reducing pain.
Studies show that CPP has negative effects on women’s sexual functions [15, 19–23] . The study of Maruta et al. [22] , including 50 women with CPP, revealed that 78% of the women with CPP and 84% of their husbands reported a deterioration or interruption in their sexual life. In a study by Verit et al. [23] , involving 112 women with CPP and 108 healthy women and aiming to identify sexual function disorder prevalence and related factors, it was found that the sexual function disorder prevalence in women with CPP was 67.8% and 32.2% in women without CPP. This study also identifies sexual function cycle and related risk factors of women with CPP. When compared to those in the control group, women with CPP experi-enced less desire, stimulation, lubrication, orgasm, satis-faction and pain scores; total FSFI score in the case group was 21.35 8 7.74 on average, and 27.29 8 6.54 on average in the control group, which indicates a significant differ-ence. Verit et al. [23] found that women with CPP had sexual pain disorder most frequently (74.3%) followed by hypoactive sexual desire disorder (53.8%). Van Balken et al. [24] claimed that the sexual lives of many patients with lower urinary system function disorder improve after treatment (PTNS) and they have fewer urological com-plaints. Their multicentric prospective study included 121 patients (45 men, 76 women): 83 with overactive blad-der (22 men, 61 women), 23 with CPP (17 men, 6 women)
and 15 with nonobstructive urinary retention (9 men, 6 women). Most of the patients reported having sexual function disorder before treatment, but they were found to have more desire, more frequent intercourse and be more satisfied in their sexual lives after treatment. Al-though positive changes after treatment were detected in women with overactive bladder, no statistically signifi-cant difference was found in patients with CPP [24] . Women’s total FSFI scores obtained in our study were 20.87 8 6.76 for the experimental group before treatment and 21.47 8 5.87 for the women in the control group. These scores are below the FSFI approximation score (26.55). Similar to the studies conducted previously, women had negative effects on their sexual lives. The only significant difference detected in the women in the ex-perimental group after treatment was in FSFI pain reduc-tion. Women had less pain during sexual intercourse af-ter PTNS. Although there is an increase in the FSFI total scores after PTNS, this increase is not significant ( ta-ble 3 ). This might be caused by the limited number of cases.
Interval PTNS is a new treatment option that is minimally invasive, easily applicable and has no side ef-fects [9, 25, 26] . In a multicentric, prospective study by Govier et al. [9] including 53 patients with overactive bladder, 3 displayed minor side effects: 1 patient had mild pain in the needle insertion site, 1 patient had moderate pain in her right foot, and 1 patient had stom-achache. Klingler et al. [26] found no complications ex-cept for 1 patient having minimal pain in the needle insertion site. Similarly, no serious complications were detected in our study. In only 4 of the 12 sessions con-ducted, 4 patients had mild pain in the needle insertion site and 1 patient had mild hematoma in the needle in-sertion site.
Our findings support the fact that PTNS is a treatment option that is minimally invasive, easily applicable and has no side effects.
Conclusion
In conclusion, this study shows that TNS treatment decreases pain, resulting in an improvement in the pa-tients’ quality of life, and helping them carry on their daily activities more comfortably. However, studies with long-term monitoring and more participants are need-ed.
Acknowledgements
We would like to thank Istanbul University Urogynecology Unit who gave permission for this study and all the patients who agreed to participate in the study.
Disclosure Statement
The authors have no conflicts of interest to disclose.
References
1 Duffy S: Chronic pelvic pain: defining the scope of the problem. Int J Gynaecol Obstet
2001; 74(suppl 1):S3–S7.
2 Van Balken MR, Vandoninck V, Messelink BJ, Vergunst H, Heesakkers JPFA, Debruyne FMJ, Bemelmans BLH: Percutaneous tibial nerve stimulation as neuromodulative treat-ment of chronic pelvic pain. Eur Urol 2003;
43: 158–163.
3 Kim SW, Paick JS, Ku JH: Percutaneous pos-terior tibial nerve stimulation in patients with chronic pelvic pain: a preliminary
study. Urol Int 2007; 78: 58–62.
4 Akkoç Y, Ozdedeli S: Percutaneous tibial nerve stimulation in the treatment of neuro-genic overactive detrusor – preliminary study. 1st Congress of Pelvic Floor Health and Miction Disorders, Antalya, 2007, poster N:80.
5 Ozkurkcugil C, Yaşar H, Culha M: Percuta-neous tibial nerve stimulation in the treat-ment of persistent overactive detrusor. 1st Congress of Pelvic Floor Health and Miction Disorders, Antalya, 2007, poster N:79. 6 Karademir K, Baykal K, Sen B, Senkul T, Iseri
C, Erden D: A peripheric neuromodulation technique for curing detrusor overactivity: Stoller afferent neurostimulation. Scand J
Urol Nephrol 2005; 39: 230–233.
7 Nuhoglu B, Fidan V, Ayyıldız A, Ersoy E, Germiyanoğlu C: Stoller afferent nerve stim-ulation in women with therapy resistant over active bladder: a 1-year follow-up. Int
Uro-gynecol J Pelvic Floor Dysfunct 2006; 17:
204–207.
8 Stoller ML: Afferent nerve stimulation for pelvic floor dysfunction. Eur Urol 1999; 35(suppl 2):16.
9 Govier FE, Litwiller S, Nitti V, Kreder KJ, Rosenblat P: Percutaneous afferent neuro-modulation for the refractory overactive bladder: results of a multicenter study. J Urol
2001; 165: 1193–1198.
10 Pınar R: Quality of life of patients with dia-betes mellitus and examination of the factors affecting the quality of life (in Turkish). Is-tanbul, Istanbul University Health Sciences Institute thesis of doctorate, 1995.
11 Kuguoglu S, Aslan FE, Olgun N: The Turkish adaptation of the McGill Melzack pain
ques-tionnaire (MPQ) (in Turkish). Pain 2003; 15:
47–51.
12 Rosen R, Brown C, Heiman J, Leiblum S, Meston C, Shabsigh R, Ferguson D, D’agostino R: The female sexual function in-dex (FSFI): A multidimensional self-report instrument for the assessment of female
sex-ual function. J Sex Marital Ther 2000; 26:
191–208.
13 Aygin D, Aslan FE: The Turkish adaptation of the female sexual function index (in
Turk-ish). Turkish Clinics J Med Sci 2005; 25: 393–
399.
14 Ozdamar K: Biostatistic with SPSS, ed 5 (in Turkish). Eskisehir, Kaan Publication, 2003. 15 Zondervan KT, Yudkin PL, Vessey MP,
Dawes MG, Barlow DH, Kennedy SH: Preva-lence and incidence of chronic pelvic pain in primary care: evidence from national gen-eral practice database. Br J Obstet Gynaecol
1999; 106: 1149–1155.
16 Zondervan KT, Yudkin PL, Vessey MP, Jen-kinson CP, Dawes MG, Barlow DH, Kennedy SH: The community prevalence of chronic pelvic pain in women and associated illness
behaviour. Br J Gen Pract 2001; 51: 541–547.
17 Demir F: Investigation gynecological, uro-logical, psychiatric factors in chronic pelvic pain: diagnostic laparoscopy in chronic pelvic pain (in Turkish). Thesis of expertise, Isparta, 2006.
18 Grace VM, Zondervan KT: Chronic pelvic pain in women in New Zealand: comparative well-being, comorbidity, and impact on work and other activities. Health Care
Wom-en Int 2006; 27: 585–599.
19 Zondervan KT, Yudkin PL, Vessey MP, Jenkinson CP, Dawes MG, Barlow DH, Ken-nedy SH: Chronic pelvic pain in the com-munity – symptoms, investigations, and
diagnoses. Am J Obstet Gynecol 2001; 184:
1149–1155.
20 Jamieson DJ, Steege JF: The prevalence of dysmenorrhea, dyspareunia, pelvic pain and irritable bowel syndrome in primary care
practices. Obstet Gynecol 1996; 87: 55–58.
21 Mathias SD, Cupperman M, Liberman RF, Lipschutz RC, Steege JF: CPP prevalence health related quality of life and economic
correlates. Obstet Gynecol 1996; 87: 321–327.
22 Maruta T, Osborne D, Swanson DW, Halling JM: Chronic pain patients and spouses: mar-ital and sexual adjustment. Mayo Clin Proc
1981; 56: 307–310.
23 Verit FF, Verit A, Yeni E: The prevalence of sexual dysfunction and associated risk fac-tors in women with chronic pelvic pain: a cross-sectional study. Arch Gynecol Obstet
2006; 274: 297–302.
24 Van Balken MR, Vergunst H, Bemelmans BL: Sexual functioning in patients with low-er urinary tract dysfunction improves aftlow-er percutaneous tibial nerve stimulation. Int J
Impot Res 2006; 18: 470–475.
25 Van Balken MR, Vergunst H, Bemelmans BL: The use of electrical devices for the treat-ment of bladder dysfunction: a review of
methods. J Urol 2004; 172: 846–851.
26 Klingler HC, Pycha A, Schmidbauer J, Mar-berger M: Use of peripheral neuromodula-tion of the S3 region for treatment of detru-sor overactivity: a urodynamic-based study.
Urology 2000; 56: 766–771.