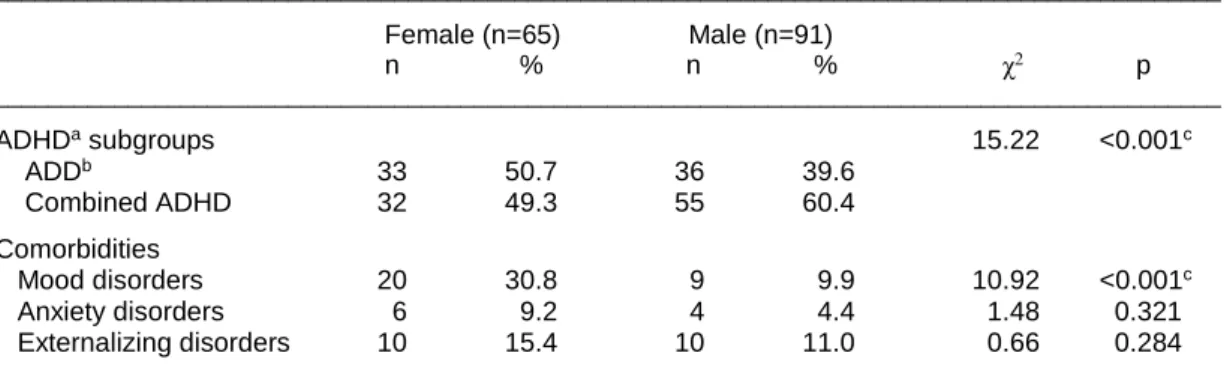
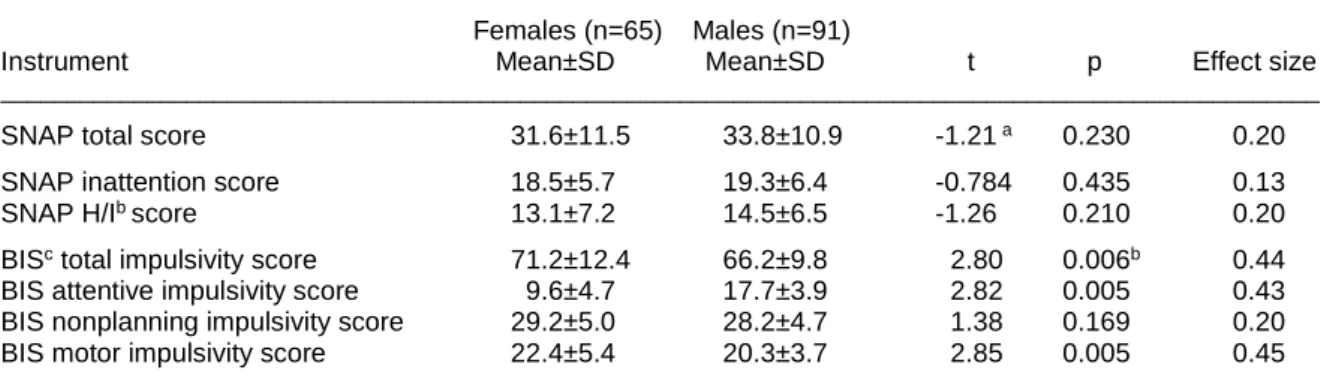
Effect of gender differences on impulsivity in adolescents with attention-deficit/hyperactivity disorder
Tam metin
Şekil
Benzer Belgeler
By using optical flow motion estimation, Eigen values and particle swarm optimization techniques, the underlying problem of person recognition has been
It can be inferred from this study that organizational democracy is an considerable factor that can be utilized by managers to encourage the positive behaviors of staff members
Çalışmaya Aralık 2014 - Mayıs 2014 tarihleri arasında zayıflık şikâyeti ile başvuran ve çalışmaya katılmayı kabul eden 45 kişi ve hasta grubunun yaş ve
Kuramsal anlamda eldeki bilgilerin ve aile hekimli¤i- nin biyopsikososyal model ve birey odakl› anlay›fl› üze- rinden, aile yönelimli bir model olarak sistemik aile he-
İnsan ve Toplum Bilimleri Dergisi FSM SCHOLARLY STUDIES Journal of Humanities and Social Sciences. Danışma Kurulu /
Al-Subaiegh ve ark., (1), %15 kuru madde düzeyinde gerek yaş gerekse de kuru damıtık tahıl kullanılmasının benzer düzeylerde süt üretimi, komposizyonu ile kuru
26.03.2010 tarihinde Resmi gazetede yayınla- nan 5957 sayılı Kanunun 1.maddesine göre kanunun amacı; “sebze ve meyveler ile arz ve talep derinliğine göre belirle- necek
Acil Durum Barınağı Armadillo Biyomimikri Doğadan Esinlenme Mekansal Tasarım Keywords: Emergency Shelter Armadillo Biomimicry Inspiration by Nature Spatial Design
