Evaluation of Polycystic Ovary Syndrome Patients with Strain Echocardiography
Tam metin
Şekil
Benzer Belgeler
Assessment of left ventricular function with tissue Doppler, strain, and strain rate echocardiography in patients with familial
Although there was no relation in terms of tissue Doppler parameters between pseudoexfoliative glaucoma and pseudoex- foliation syndrome patients, plasma BNP concentrations were
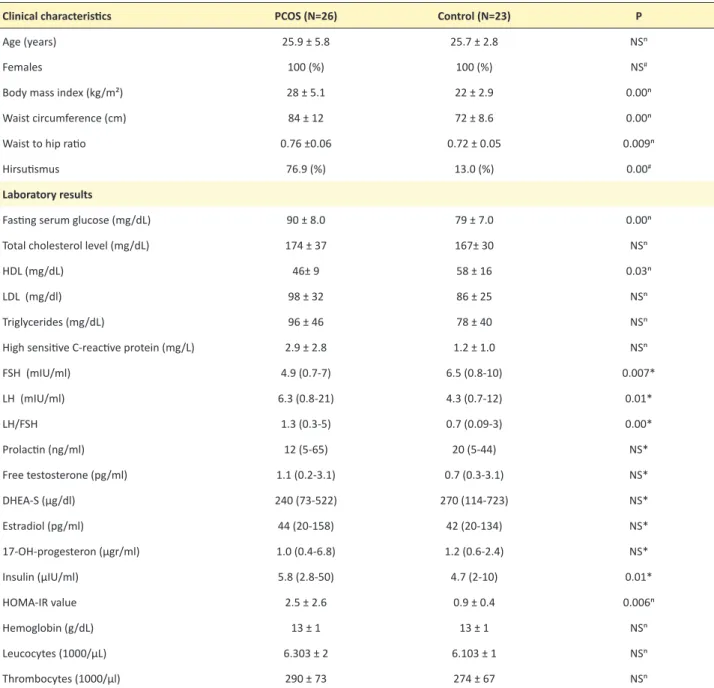
Clinical characteristics and laboratory findings of patients included in the study are shown in Table 1. Mean age of study population was 26.0±5.6 years with no difference between
Our aim was to investigate the relationship of body mass index (BMI) and IR with left venticular mass index (LVMI) in obese and nonobese, normotensive, nondiabetic women.. Methods:
[9] In our study, higher IR was detected in patients with PCOS, though not statistically significantly different, and mean plasma SeP level was lower than that of the
In the present study, the prevalence of uterine anomalies in infertile patients with PCOS admitted to our hospital was evaluated retrospectively, and a
Role of osteocalcin, tumor necrosis factor-alpha and adiponectin in polycystic ovary syndrome patients with insulin resistance.. Turk J Obstet
The aim of the study is to determine left ventricular (LV) functions by tissue Doppler imaging (TDI) and strain/strain rate echocardiography (SE/SRE) in mitral stenosis patients
