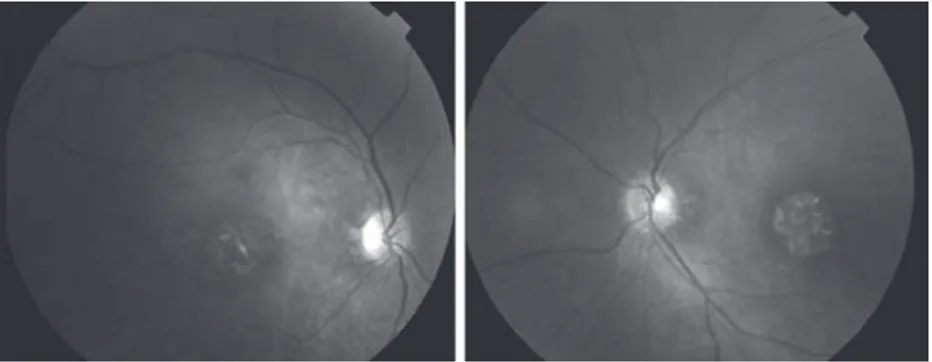
Neuro-ophthalmologic findings in humans with quadrupedal locomotion
Tam metin
Şekil
Benzer Belgeler
a fourth gene locus in a consanguineous family of two affected Table 1 Novel coding variants identified by targeted next-generation sequencing of 05-996.. Gene Position (hg19) Ref
To obtain the frequency range within which the negative refraction and the other peculiar properties incorporated with it, we have calculated the equal frequency contours of
Augusto Boal’in en bilindik ve en verimli yaklaşımı olan Forum Tiyatro yaklaşımında diğer yaklaşımlarda olduğu üzere seyirci oyuncular gerçek yaşamda var olan
Nevertheless, the pattern of correlations supports the overall scale's validity: the materialism scale is related to the proportion of items seen as necessities
We enlarge the M&A dataset to cover developed and emerging market countries and investigate: (i) whether M&A deals generate value, (ii) how the standard data filters used in
As our results show, for managers of the companies operating in Stage 1 countries, IPAB is not a very important factor affecting their perceptions of the level of business ethics
Bazı araştırmacılarsa, 4 trilyon kilometre uzaklıkta Güneş sistemini bir küre gibi saran trilyonlarca kuyrukluyıldız- dan oluşan Oort Bulutu içinde Jüpiter
Büyük musi kişinas, bir yandan besteleri üzerin de çalışırken diğer yandan yazı il mine ve edebiyata da merak sarmış, kısa zamanda mahir bir hattat
