Are perioperative near-infrared spectroscopy values correlated with clinical and biochemical parameters in cyanotic and acyanotic infants following corrective cardiac surgery?
Tam metin
Şekil

Benzer Belgeler
Hint-İran geleneğin- den doğarak Türk ve İslami gelenekle harmanlanmış daire-i adalete içkin yö- netim bilgisi Osmanlı Devleti’ne aktarılmış; Osmanlı Devleti’nin
Systemic right ventricle in elderly patients with congenitally corrected transposition of the great arteries: Clinical profile, cardiac.. biomarkers, and
This study examined the relationship between congenital heart disease and oxidative stress by measuring the total antioxidant status (TAS), total oxidant status (TOS), and
Whi- le analysing the rheograms, the following values had been assessed: A (in ohm) – reflecting blood supply to cerebral vascular basin dependent on cardiac out- put and tension
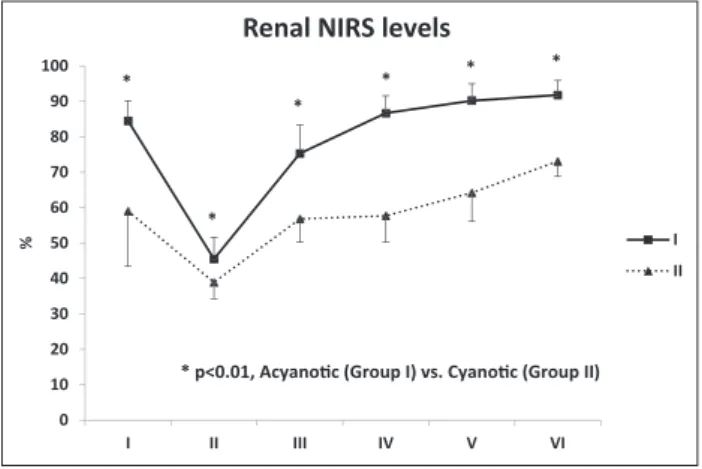
Background: This study aims to investigate cerebral oxygenation differences between cyanotic and non-cyanotic pediatric cardiac surgery patients using near-infrared
Prior to attempting surgery, it is important to consider the presence of preoperative pneumonia, acidosis, and poor postoperative forced expiratory volume in 1 second and
高血壓自我保健 返回 醫療衛教 發表醫師 李彩鳳醫師 發佈日期 2010/09/07 高血壓自我保健 中醫科李彩鳳主治醫師
Abbreviations: RScO 2 , right cerebral oxygen saturation; LScO 2 , left cerebral oxygen saturation; NS, not significant.. determine the baseline NIRS values of patients who
