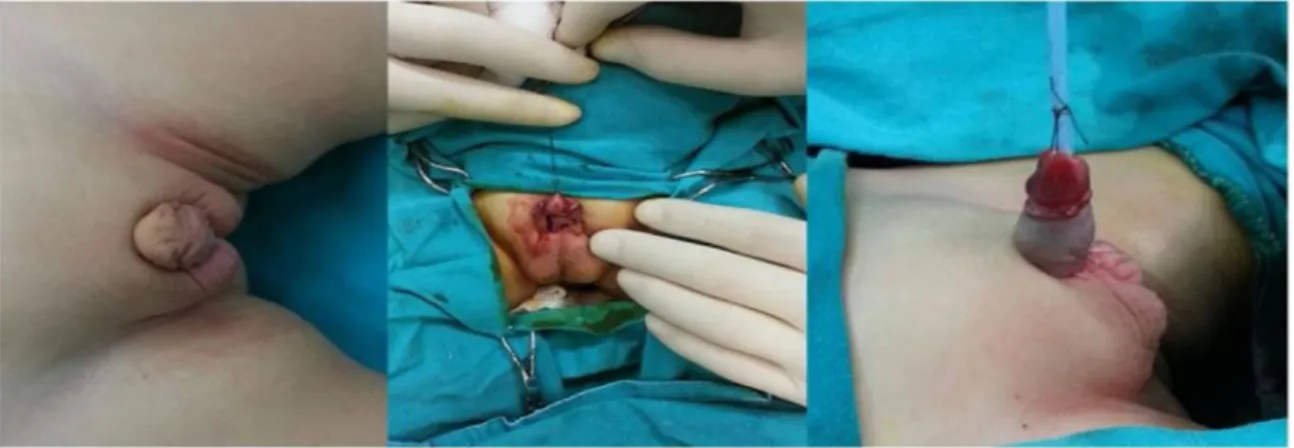
Modified Hinderer's Technique for Serious Proximal Hypospadias with Ventral Curvature: Outcomes and Our Experience
Tam metin
Şekil

Benzer Belgeler
Proksimal hipospadyaslı primer vakalarda TIPU sonrası başarı oranlarımız ilk operasyon son- rası penoskrotal seviyede %33,3, proksimal penil seviyede %55,6 olmuştur; ilk
Conclusion: We suggest that microdiscectomy and implantation of the artificial cervical disc prosthesis is a safe and effective procedure for reduction of pain and improvement of
In this study, the surgical results of patients, in whom the pupil dilatation was inadequate during the cataract surgery via PHACO and foldable iris hooks were used, were
While conservative follow-up was sufficient for 75 (92.59%) of 81 patients with laryngomalacia, supraglottoplasty was performed in three patients (3.7%) be- cause of
After atrial switch operations arrythmias, baffle leak, systemic or pulmonary return obstructions, RV and tricuspid valve insufficiencies can be observed as late
As a single catheter was used for coronary can- nulation in a great majority of patients undergoing TRA, the mean catheter number used for TRA was significantly
asır Türkmen Edebiyatının önemli isimlerinden Molla Nefes'in hayatı, Ģiirleri, onunla ilgili yapılan çalıĢmalar hakkında bilgi verilmiĢtir. Molla Nefes'in 119
As for tourism carrying capacity, ecological footprint and environmental valuation, this study utilized reliable and valid resources to determine environmental limit and thus
